
Introduction
Cardiogenic shock is the most severe complication of ST-segment elevated myocardial infarction (STEMI) and develops in 8–10% of the patients diagnosed with STEMI. Of these patients developing cardiogenic shock, mortality is reported to be about 40–50% [1, 2]. Cardiogenic shock treatment involves urgent coronary revascularization and administration of inotropes, but this has not shown any significant improvement in the mortality rate [3]. The use of extracorporeal life support provides both blood circulation and oxygenation. Still, its regular use did not lead to better clinical outcomes in patients suffering from acute MI and cardiogenic shock. Additionally, it was associated with increased risk of bleeding complications and limb ischemia [1, 4, 5].
Percutaneous microaxial flow pumps represent another form of active mechanical circulatory support in cardiogenic shock [6]. These devices draw blood from the left ventricle via a catheter and pump it into the ascending aorta. While they help to unload the left ventricle, their effectiveness relies on sufficient blood oxygenation and proper right-heart function to maintain adequate left ventricle filling [7]. However, three small clinical trials found no benefit of these pumps in patients with infarct-related cardiogenic shock [8–10]. Recently, the DANGER-SHOCK trial, the largest randomized controlled trial (RCT) on this subject, was published. The study demonstrated a significantly reduced risk of all-cause mortality with the use of a microaxial flow pump as compared to routine standard care. These conflicting findings warrant the need for a meta-analysis with enhanced statistical power to analyze individualized clinical outcomes.
Methods
This systematic review and meta-analysis observed the guidelines established by the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [11]. The study was registered with PROSPERO (CRD42024578700).
Data sources and search strategy
Two authors independently searched PubMed/Medline, Embase, and the Cochrane Library from their inception until 16 June 2024, with no language restrictions. Additionally, the reviewers manually examined references from retrieved trials, previous meta-analyses, and review articles to ensure that all relevant studies were included. The search string employed the following keywords and related Medical Subject Headings (MeSH) terms: (((myocardial infarction) OR (cardiogenic shock) OR (infarct-related cardiogenic shock)) AND ((microaxial flow pump)) OR (percutaneous mechanical circulatory support)) OR (Impella device)) OR (heart pump)) OR (left ventricle assist device)) OR (coronary intervention))). The detailed search strings are provided in Supplementary Table SI.
Eligibility criteria
The studies were eligible for our systematic review and meta-analysis if they: (i) were RCTs with a follow-up duration of at least 2 weeks; (ii) enrolled patients with infarct-related cardiogenic shock; (iii) included adult male or female participants who were at least 18 years old; (iv) compared the microaxial flow pump with standard care or the intra-aortic balloon pump; (v) evaluated at least one of the predetermined efficacy and safety outcomes. Other studies excluded from our analysis included those with insufficient data, case reports, case series, letters, editorials, and reviews.
Outcomes
The primary outcome included all-cause death at 30 days and 6 months, and cardiac death. The secondary outcomes included major bleeding, limb ischemia, sepsis, stroke, and rehospitalizations.
Study selection and data extraction
All the studies from the literature search were imported to EndNote X9 (Clarivate Analytics), and duplicates were identified and removed. Two authors independently reviewed trials based on their titles and abstracts. The full texts of the articles were then examined, and any study that conformed to our eligibility criteria was included. In cases of disagreement, a third author (M.A.) was consulted.
The details of baseline characteristics and outcomes were extracted from eligible studies by two investigators. A pre-piloted Excel sheet was used for data extraction.
Quality assessment of included studies
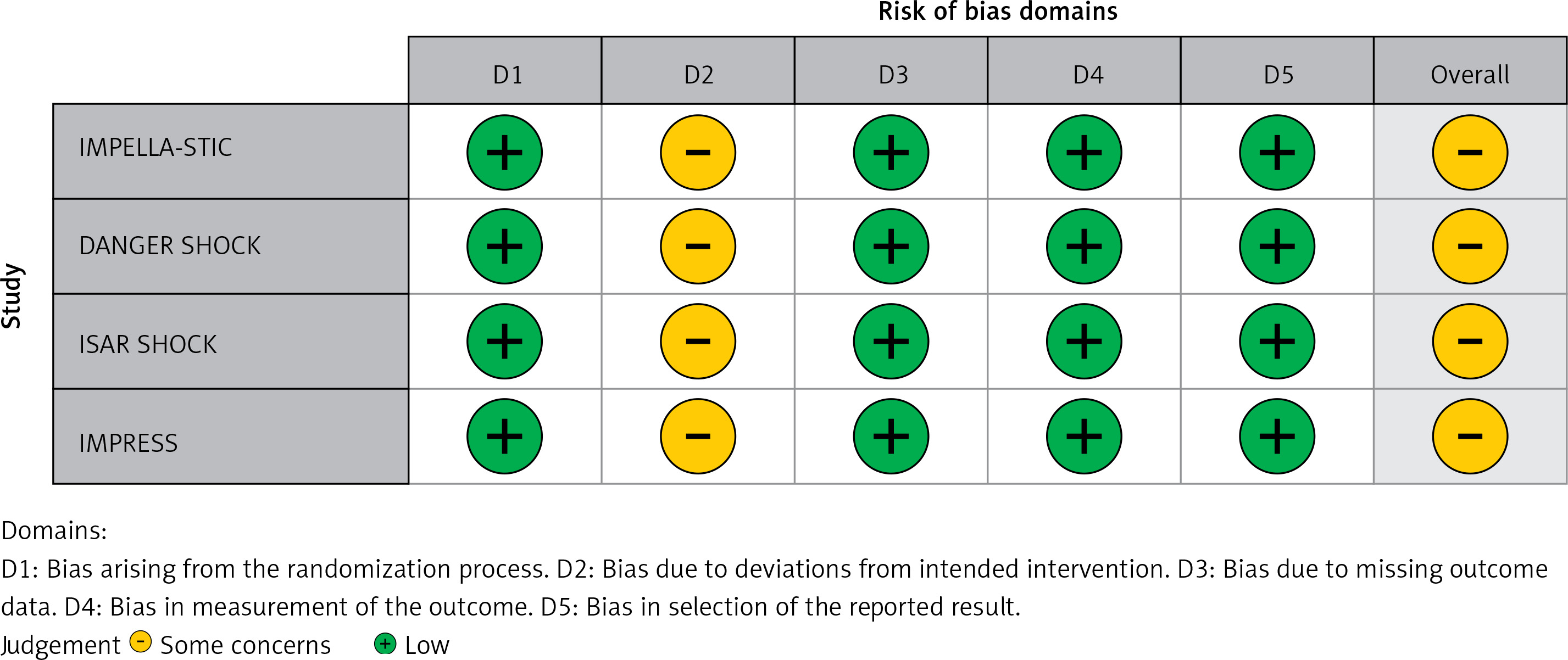
RoB 2 – a revised tool for assessing the risk of bias in randomized trials – was used to assess the risk of bias [12]. Risk of bias was assessed across five domains: randomization, deviations from intended variation, missing outcome data, measurement of outcome, and selection of reported results. The trials were scored as high, with some concerns, or low risk of bias in each domain.
Statistical analysis
Data analysis was performed using RevMan, Version 5.4 (Nordic Cochrane Center, Copenhagen, Denmark). Risk ratios (RRs) were pooled along with corresponding 95% confidence intervals (CIs) for all outcomes. The results were pooled using the DerSimonian and Laird random-effects model and visualized using forest plots [13]. Heterogeneity across the trials was assessed using the Higgins I2 test; a value < 25% indicates low heterogeneity, 25–75% indicates moderate heterogeneity, and > 75% indicates high heterogeneity [14]. A p-value of < 0.05 was considered significant in all cases.
Results
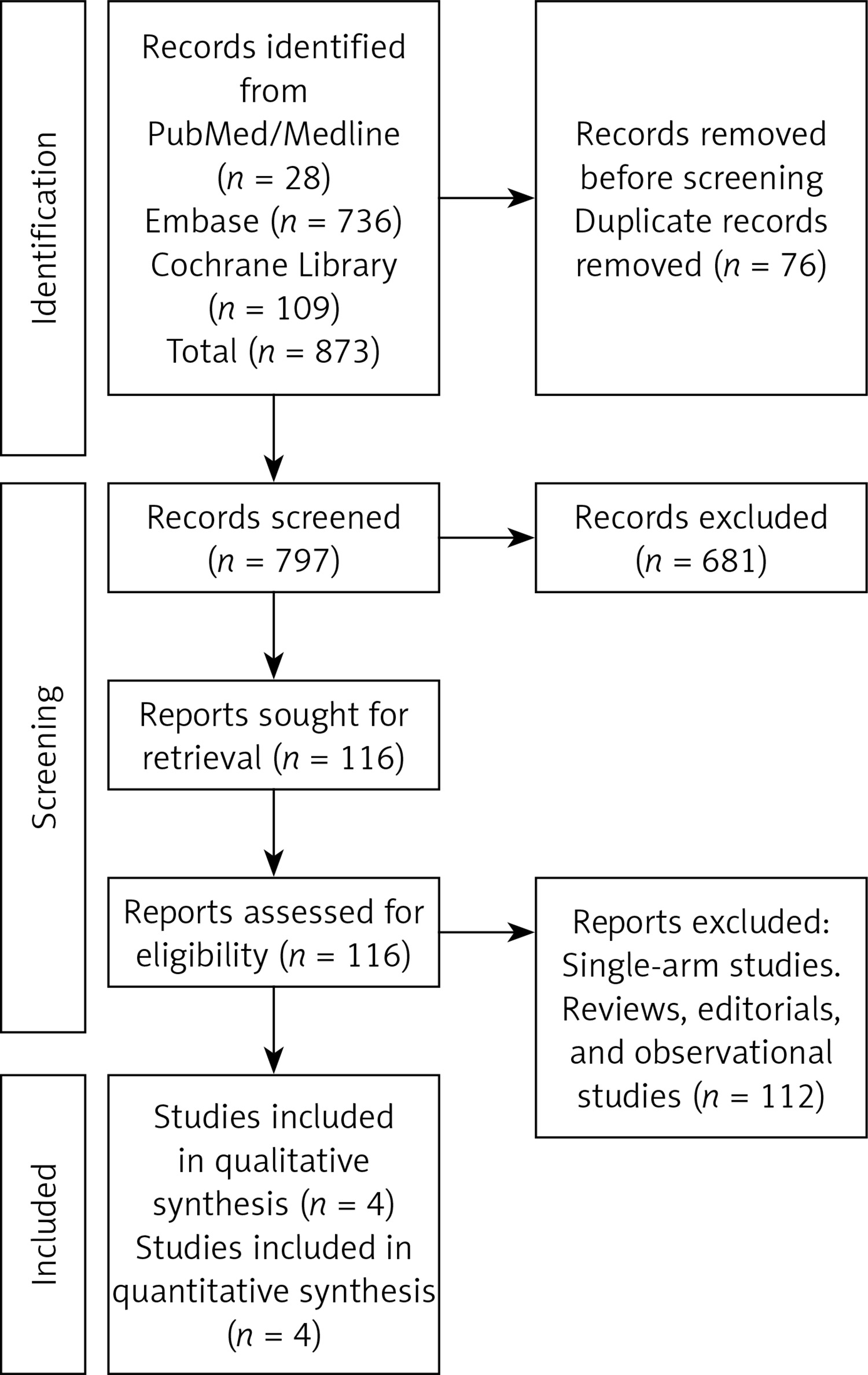
The literature search identified 873 articles. After the removal of 76 duplicate records, primary screening was conducted based on study titles and abstracts. This resulted in the exclusion of 681 records. Full-text reviews were then performed on 116 studies, identifying 4 RCTs that met the inclusion criteria and were included in the meta-analysis. The PRISMA flowchart (Figure 1) summarizes the study selection process.
Baseline characteristics and risk of bias
The 4 included RCTs [8–10, 15] reported data for 444 patients. The mean age of included patients was 57.7 ±10.2 years. The mean follow-up duration was 3.5 months. Male patients made up around 78.8% of the study sample. 61% of the patients presented with anterior wall MI leading to cardiogenic shock. Three studies [8–10] compared the use of a microaxial flow pump (Impella) with an intra-aortic balloon pump while 1 trial [15] compared the use of the Impella device with routine standard care. The details of baseline characteristics are provided in Table I. The bias assessment of included RCTs demonstrated some concerns in all studies mainly due to the non-blinding of study participants and investigators (Figure 2).
Table I
Baseline characteristics of included studies and patients
| Trial name | Year | Sample size N (IV/C) | Intervention | Control | Follow-up | Age [years] | Males N (%) | Hypertension N (%) | Diabetes N (%) | Anterior MI N (%) | LVEF % | SBP Mean ± SD | DBP Mean ± SD | Heart Rate Mean ± SD | Mean Arterial BP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IMPELLA-STIC | 2019 | 15 (7,8) | Impella LP5.0 + IABP | IABP | 30 days | IV = 60.3 ±12.3 C = 53.5 ±8.1 | IV = 6 (85.7) C = 6 (100) | IV = NA C = NA | IV = 2 (28.6) C = 0 | IV = NA C = NA | IV = 29 ±6 C = 30 ±8 | IV = NA C = NA | IV = NA C = NA | IV = 98.1 ±27.6 C = 103.8 ±14.4 | IV = 67.7 ±12.3 C = 69.9 ±7.8 |
| ISAR-SHOCK BASELINES | 2008 | 26 (13,13) | Impella LP 2.5 | IABP | 30 days | IV = 65 [57–71]* C = 67 [55–80]* | IV = 8 (62) C = 11 (85) | IV = 7 (54) C = 9 (69) | IV = 5 (39) C = 3 (23) | IV = 7 (54) C = 8 (62) | IV = 27 [20–39]* C = 28 [23–44]* | IV = 106 ±22 C = 101 ±23 | IV = 64 ±15 C = 58 ±14 | IV = 95 ±24 C = 97 ±24 | IV = 78 ±16 C = 72 ±17 |
| IMPRESS | 2017 | 48 (24,24) | Impella CP with IABP | IABP | 6 months | IV = 58 ±9 C = 59 ±11 | IV = 18 (75) C = 20 (83) | IV = 4(20) C = 6 (29) | IV = 2(9) C = 2 (9) | IV = 1 (5) C = 1 (4) | EF > 40% IV = 7 (32) C = 4 (22) | IV = 81 ±17 C = 84 ±19 | IV = 58 ±22 C = 57 ±13 | IV = 81 ±21 C = 83 ±28 | IV = 66 ±15 C = 66 ±15 |
| DANGER SHOCK | 2024 | 355 (179,176) | Impella CP 5.0 | Standard Care | 6 months | IV = 67 (58–76)* C = 69 (61–76)* | IV = 142 (79.3) C = 139 (79.0) | IV = 89 (49.7) C = 94 (53.4) | IV = 33 (18.4) C = 47 (26.7) | IV = 126 (70.4) C = 129 (73.3) | IV = 25 (20–31)* C = 25 (15–30)* | IV = 84 (72–91)* C = 82 (72–91)* | IV = NA C = NA | IV = 94 (77–110) C = 95 (76–111) | IV = 63 (55–72) C = 64 (55–73) |
Results of meta-analysis
All-cause death
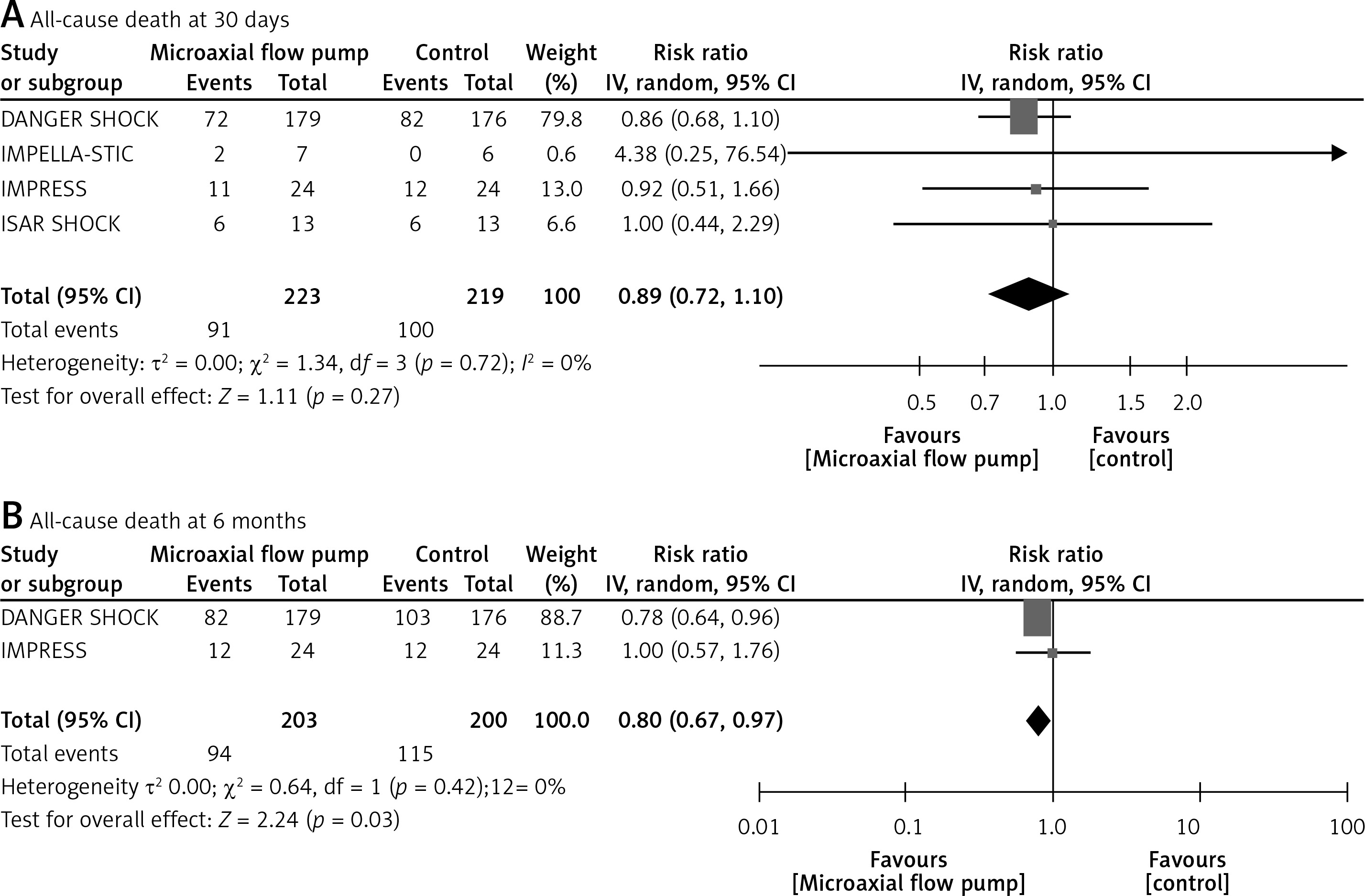
The pooled analysis demonstrated non-significantly reduced all-cause death at 30 days with the use of a microaxial flow pump (RR = 0.89; 95% CI: 0.72 to 1.10, p = 0.27, Figure 3 A). At a follow-up of 6 months, a statistically significant reduced risk of all-cause death was observed in patients who received a microaxial flow pump (RR = 0.80; 95% CI: 0.67 to 0.97, p = 0.03, Figure 3 B). No interstudy heterogeneity was observed; I2 = 0%.
Cardiac death
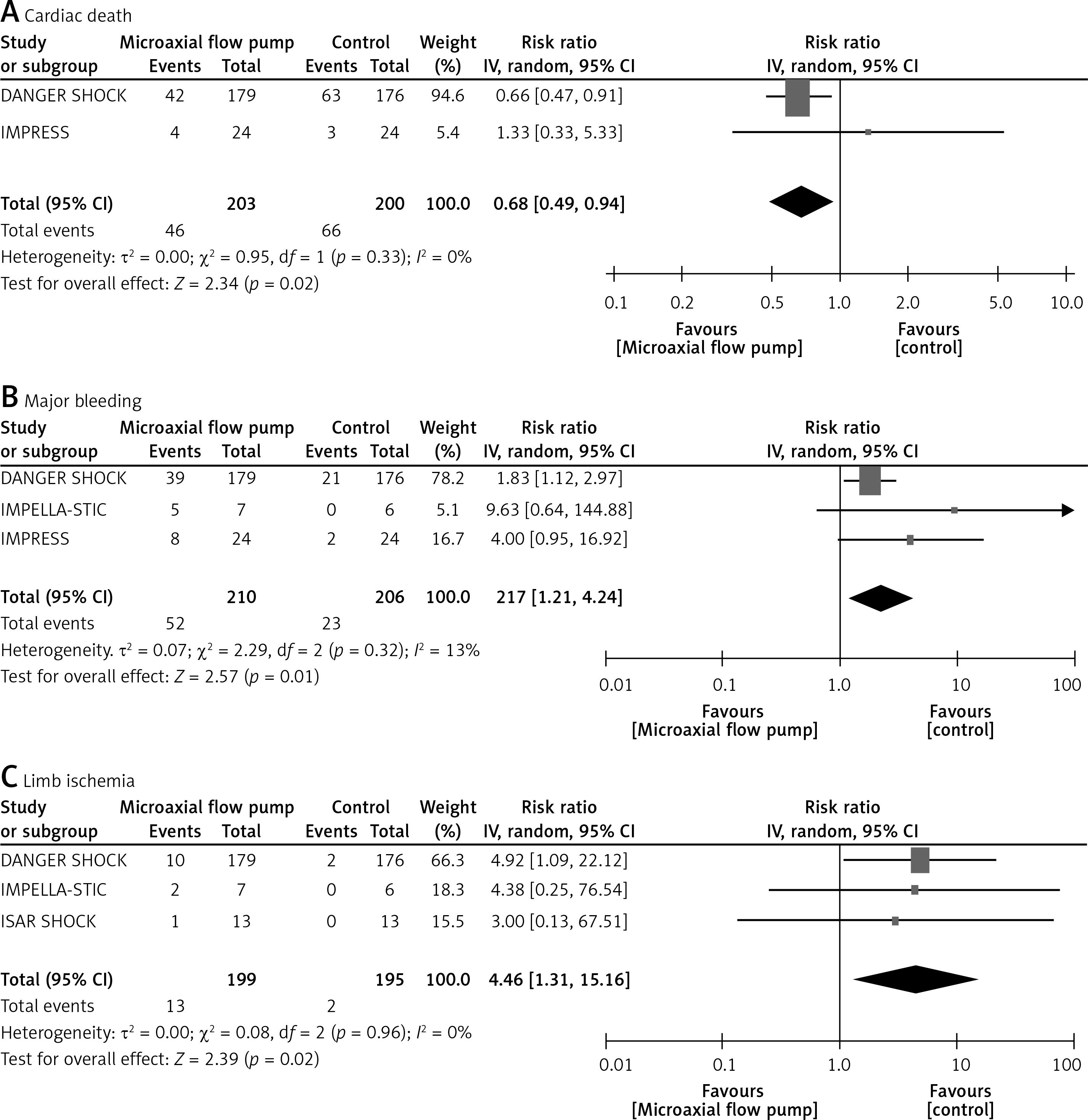
The use of a microaxial flow pump was associated with a significantly reduced risk of cardiac death (RR = 0.68; 95% CI: 0.49 to 0.94, p = 0.02, I2 = 0%, Figure 4 A).
Major bleeding, limb ischemia, and sepsis
The use of a microaxial flow pump was associated with a significantly increased risk of major bleeding (RR = 2.27; 95% CI: 1.21 to 4.24, p = 0.01, I2 = 13%, Figure 4 B), limb ischemia (RR = 4.46; 95% CI: 1.31 to 15.16, p = 0.02, I2 = 0%, Figure 4 C), and sepsis (RR = 2.01; 95% CI: 1.11 to 3.67, p = 0.02, I2 = 0%, Figure 5 A).
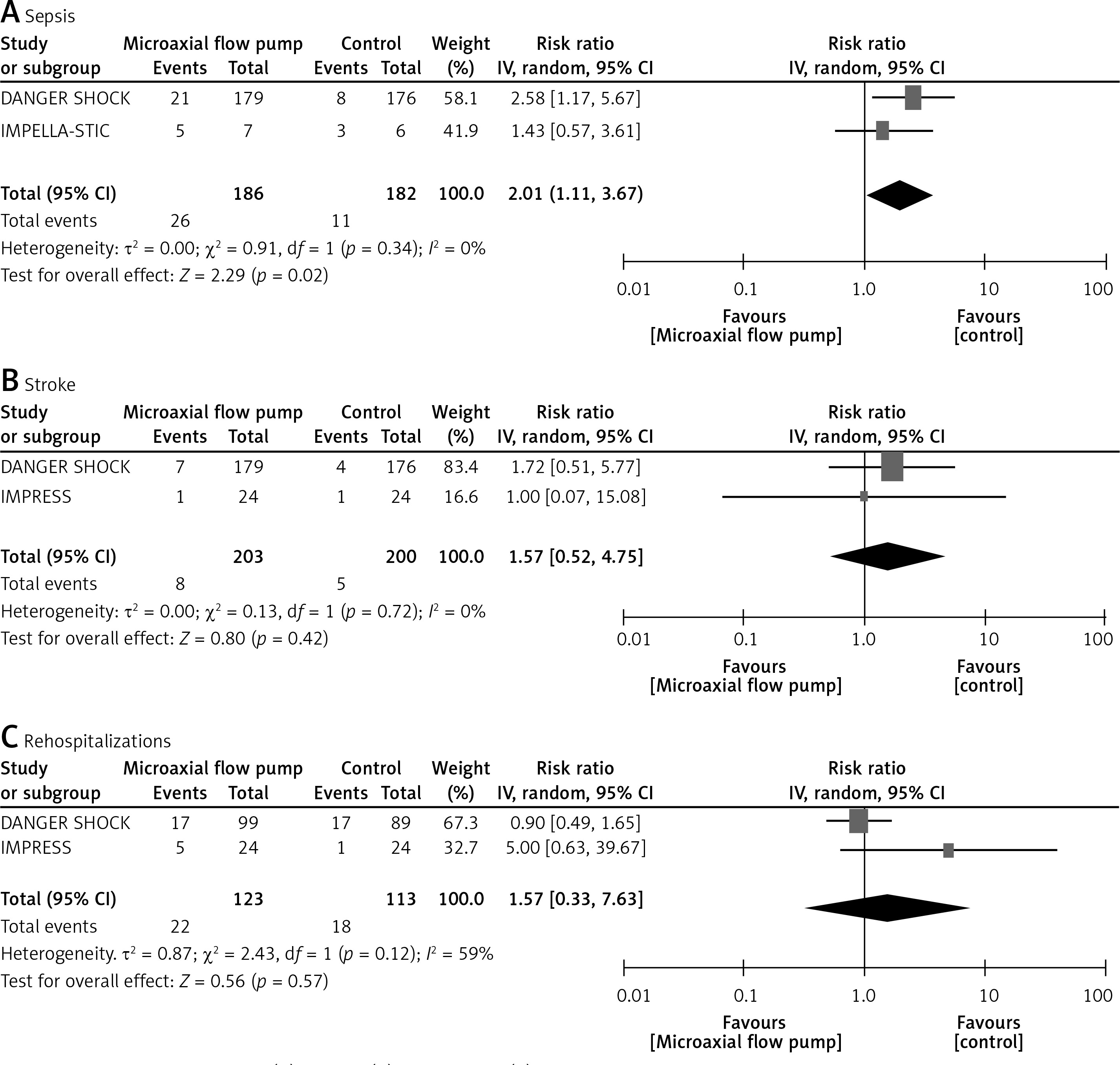
Stroke and rehospitalizations
The risk of stroke (RR = 1.57; 95% CI: 0.52 to 4.75, p = 0.42, I2 = 0%, Figure 5 B) and rehospitalizations (RR = 1.57; 95% CI: 0.33 to 7.63, p = 0.57, I2 = 59%, Figure 5 C) remained comparable across the two groups.
Discussion
This meta-analysis of 4 RCTs encompassing 444 patients demonstrated that the use of a microaxial flow pump is associated with a significantly reduced risk of all-cause mortality at 6 months and cardiac death in patients with infarct-related CS. However, the use of a microaxial flow pump was associated with a significantly increased risk of major bleeding, limb ischemia, and sepsis as compared to the control group. The results were comparable across the two groups for stroke and rehospitalizations.
There has been an increase in the use of mechanical circulatory support devices (MCS) in cardiovascular practice over the last decade [16–18]. Among MCS devices, Impella is the most popular for improving left ventricle function [8]. Studies have been conducted to investigate the role of the Impella in patients with cardiogenic shock, with conflicting results. In this meta-analysis, we comprehensively synthesized the available data from RCTs regarding the role of the microaxial flow pump (Impella). Our meta-analysis based on these trials demonstrated a significantly reduced risk of all-cause mortality at 6 months, and cardiac mortality in the microaxial flow pump group. Non-significantly reduced all-cause mortality at 30 days was observed. Several factors should be considered while interpreting these findings: The ISAR-SHOCK trial [8] evaluated the use of the Impella device in 25 patients. The microaxial flow pumps were employed after the initial treatment of patients with catecholamines and other inotropes. The investigators found that the use of a percutaneous microaxial flow pump was associated with a significantly improved cardiac index; however, the study was underpowered to investigate its impact on mortality. The IMPRESS trial [9] evaluated the use of the Impella CP in patients who were mechanically ventilated before randomization. The study found no statistically significant differences in all-cause mortality at 30 days and 6 months with the use of a percutaneous microaxial flow pump as compared to the control group. This could be attributed to the inclusion of extremely sick patients in the study, as all included patients were mechanically ventilated before the placement of the microaxial flow pump. The IMPELL-STIC trial [10] enrolled 15 patients to test whether the use of a percutaneous microaxial flow pump can improve hemodynamic outcomes. The study demonstrated no statistically significant improvement in cardiac power and left ventricular ejection fraction (LVEF) with the use of a microaxial flow pump. It is important to mention that only 13 patients were included in the final analysis, leading to decreased statistical power to detect any meaningful changes in intervention and control arms. DANGER-SHOCK [15] is the largest trial that has evaluated the outcomes with the use of a percutaneous microaxial flow pump in patients with infarct-related shock. This study differs from other RCTs evaluating the efficacy of MCS, as the investigators enrolled a uniform patient population. Patients were enrolled in the trial if they had elevated arterial lactate levels without cardiac arrest and a high rate of LVEF failure. The study met its primary endpoint with a statistically significant reduction in all-cause mortality at 6 months.
All trials observed an increased risk of bleeding, limb ischemia, and sepsis in patients with CS being treated with a microaxial flow pump. A similar trend was observed in our pooled analysis. These risk factors can lead to increased mortality in patients with infarct-related CS, but it is encouraging that these severe complications did not outweigh the benefits of treatment with a microaxial flow pump, as the overall mortality rates were low with the treatment. However, it remains essential to focus on preventing serious adverse events associated with microaxial flow pump placement.
The findings of our meta-analysis indicate that microaxial flow pumps reduce the risk of all-cause and cardiac death in patients with infarct-related cardiogenic shock. However, their use was associated with increased complications, including bleeding, which is found across all MCS devices. In patients with cardiogenic shock, the risk of these complications is further increased by concomitant use of antiplatelets, vasopressors, and anticoagulants. Future research should focus on minimizing the risk of these complications, which might translate to better survival rates as well. It is important to mention that there is a lack of large-scale RCTs on this topic, and further trials with high statistical power are required to validate our findings.
Several limitations should be considered while interpreting our findings. This is a study-level meta-analysis and the lack of individual patient-level data made it difficult to evaluate the impact of potential effect modifiers. There was a difference in the enrollment criteria among trials, time of microaxial flow pump placement, supportive therapy (catecholamines, inotropes), and the duration of follow-up, which might have influenced our findings. Moreover, DANGER-SHOCK had the largest sample size among all included studies and could have influenced our pooled analysis.
In conclusion, the use of a microaxial flow pump in patients with infarct-related cardiogenic shock leads to a significantly reduced risk of all-cause mortality at 6 months of follow-up and cardiac mortality. An increased risk of adverse events was associated with microaxial flow pump placement as compared to the control group. Additional RCTs with large sample sizes and uniform inclusion criteria of patients are required to reach a definitive conclusion.