Introduction
Cannabis is one of the most consumed substances worldwide. With the legalisation of marijuana over the last decades in different areas of the United States, a rise in social acceptance and recreational use was noted [1, 2]. Past studies have highlighted the potential nefarious impacts of cannabis, including inflammation and accelerated atherosclerosis via the cannabinoid receptor type 1 (CB1) [3–5]. Cannabinoids also influence platelet activation, which may trigger thromboembolism [6]. In light of these observations, a strong link between marijuana use and myocardial changes has been hypothesised [7, 8]. Cannabis has been shown to lower the anginal threshold by 48% and increase events of acute myocardial infarction (AMI) by up to 4.8 fold, which may be due to the direct impact of cannabinoids on myocardial tissue or indirectly via changes in parasympathetic-sympathetic balance [2, 7, 9–13].
Patel et al. documented a 32% rise in reported cannabis use among adults aged 18–49 years with AMI between 2010 and 2014, correlating with a 60% surge in mortality [11]. Beyond this relatively young cohort of patients, there remains a paucity of data about the in-hospital outcomes of cannabis users of all age groups admitted to hospital with AMI over a broader time scale. The objective of our research is to investigate any association between cannabis use and the outcomes following AMI in adults aged 18 to 80 years over a 20-year period using data available from a national database.
Material and methods
Our study relied on data from the National (Nationwide) Inpatient Sample (NIS), one of the most extensive all-payer databases of discharge records from the United States. It is produced yearly by the Healthcare Cost and Utilisation Project (HCUP), under the support of the Agency for Healthcare Research and Quality (AHRQ). This yearly database contains around 7 million records in its unweighted form, which can be converted into a national estimate via year-appropriate weights using HCUP’s recommendations. With up to 48 states contributing, the NIS database represents more than 97% of the US population. We identified data relevant to our study using the International Classification of Disease, 10th revision (ICD-10) codes, for records dated 1 October 2015 and later, and used the International Classification of Disease, 9th revision (ICD-9) codes for all data prior to that date [14–29].
Study design and statistical analysis
We performed a retrospective analysis of the NIS data, from 1 January 2001, to 31 December 2020. Patients of ages < 18 or > 80 years were excluded from our study. Our sample consisted of hospitalisations with a primary diagnosis of AMI via ICD-9 and ICD-10 codes from past studies. All cases that qualified as “Drug Abuse” based on ICD-9 and ICD-10 codes were excluded from our control group [30]. We studied the prevalence of multiple comorbidities as well as patient and hospital characteristics between cannabis users and non-users. Pearson’s χ2 tests were used for categorical groups, and T-tests were applied for continuous variables for the mean ± standard deviation (SD). The differences in outcomes were analysed via multivariate regression models, where we adjusted for patient characteristics such as sex, insurance, weekend status, race, age groups, as well as comorbidities including hypertension, dyslipidaemia, smoking, diabetes, chronic kidney disease, history of coronary artery bypass grafting (CABG), history of percutaneous coronary intervention (PCI), family history of coronary artery disease (CAD), peripheral vascular disease (PVD), liver cirrhosis, alcohol abuse, history of myocardial infarction, obesity status, Charlson Comorbidity Index (CCI) group, and hospital location/teaching status.
In the second part of our study, patients with and without cannabis use were matched for multiple comorbidities and patient characteristics at a 1 : 1 ratio and a caliper of 0.1. Due to the extensive sample size, potential uneven distribution of data in various variables, and risk of imbalance in matching for some variables, we performed a second set of multivariate regression models to the matched sample to estimate the differences in multiple outcomes between cannabis users and non-users. Primary outcomes consisted of mortality, while secondary outcomes consisted of the use of CABG, PCI, intra-aortic balloon pump (IABP), different cardiac arrhythmias, events of cardiogenic shock, acute kidney injury (AKI), acute ischaemic stroke (AIS), and cardiac arrest.
Our study was performed via SPSS 29.0 (IBM Corp, Armonk, NY, USA), STATA 18.0 (Stata Corporation, College Station, TX, U.S.A.), and R-studio (2023.09.1 Build 494). Packages “haven”, “MatchIt”, and “cobalt” were used for R-studio (https://cran.r-project.org/).
Institutional Board Review or ethics board approval
The NIS is released in de-identified form and is publicly available upon appropriate request from HCUP. Therefore, HCUP waives the need for Institutional Board Review or ethics board approvals for NIS-related studies.
Data provider and use
HCUP, AHRQ, and partners provided the data. As per HCUP criteria, we masked any cell that contained less than 11 cases, to protect the de-identified nature of the database. Additional information regarding the partners associated with AHRQ can be found at https://hcup-us.ahrq.gov/partners.jsp.
Results
In total, 9,930,007 patients with AMI admitted between 2001 and 2020 matched our selection criteria. We found 117,641 (1.2%) patients who reported cannabis use.
Pre-propensity-score-matched analyses
Basic characteristics
Among all AMI cases, patients with cannabis use were younger (mean age: 51.00 vs. 62.74 years, p < 0.01). Both groups consisted of admissions mostly during weekdays, with cannabis users having a higher prevalence of weekend hospitalisations (27.6% vs. 25.8%, p < 0.01). While both groups had a higher prevalence of males (78.8% vs. 65.1%) and Whites (58.6% vs. 74.9%), cannabis users showed a lower percentage of females (21.2% vs. 34.9%, p < 0.01) and a higher percentage of Blacks (29.2% vs. 10.5%, p < 0.01), when compared to the non-user group. Non-users were covered primarily by Medicare (48.7%), while the most common form of insurance was Medicaid (27.1%) among our cannabis-use cohort.
Cannabis users also reported a higher prevalence of alcohol abuse (17.9% vs. 3.0%, p < 0.01), cirrhosis (1.9% vs. 1.1%, p < 0.01), smoking (77.6% vs. 40.9%, p < 0.01), prior myocardial infarction (15.0% vs. 11.3%, p < 0.01), prior PCI (13.5% vs. 12.8%, p < 0.01), family history of coronary artery disease (CAD) (18.1% vs. 10.4%, p < 0.01), and obesity (17.7% vs. 15.4%, p < 0.01) while showing lower prevalence of hypertension (54.2% vs. 60.3%, p < 0.01), dyslipidaemia (55.7% vs. 57.8%, p < 0.01), diabetes (24.7% vs. 36.8%, p < 0.01), CKD (10.2% vs. 12.6%, p < 0.01), PVD (6.2% vs. 8.1%, p < 0.01), and prior CABG (4.2% vs. 7.6%, p < 0.01) than non-users. The proportion of cannabis users with a CCI score of ≥ 3 was lower compared to non-users (29.7% vs. 30.6%, p < 0.01). Both groups were primarily treated in urban teaching centres (Table I).
Table I
Characteristics of patients aged 18–80 years admitted for acute myocardial infarction with and without a history of cannabis use between 2001 and 2020 in the United States
Cardiac arrhythmias and outcomes
Our pre-propensity-score-matched (PSM) sample reported various differences in events of cardiac arrhythmias and outcomes. While cannabis users had a higher incidence of reporting supraventricular tachycardia (1.4% vs. 1.1%, p < 0.01), ventricular tachycardia (7.6% vs. 6.6%, p < 0.01), and ventricular fibrillation (4.1% vs. 3.6%, p < 0.01), atrial fibrillation was more common among the non-users (7.5% vs. 13.7%, p < 0.01). We also found that people using cannabis had higher use of PCI (50.9% vs. 48.4%, p < 0.01) than non-users while having fewer procedures involving CABG (9.2% vs. 10.6%, p < 0.01) and IABP (3.5% vs. 5.1%, p < 0.01). Compared to non-users, cannabis users reported fewer events of cardiogenic shock (3.8% vs. 5.2%, p < 0.01), cardiac arrest (2.9% vs. 3.1%, p < 0.01), acute ischaemic stroke (1.4% vs. 2.4%, p < 0.01), acute kidney injury (12.3% vs. 12.5%, p < 0.01), and in-hospital mortality (1.8% vs. 4.3%, p < 0.01). They also had a shorter hospitalisation (mean length of stay 3.85 vs. 4.72 days, p < 0.01) (Table I).
Multivariate regression analyses
Multivariate regression analyses of our pre-PSM sample found that for patients admitted with AMI, those with cannabis use were less likely to report atrial fibrillation (aOR = 0.933, p < 0.01), use of CABG (aOR = 0.949, p < 0.01), PCI (aOR = 0.858, p < 0.01), events of cardiogenic shock (aOR = 0.785, p < 0.01), IABP (aOR = 0.742, p < 0.01), acute ischaemic stroke (aOR = 0.863, p < 0.01), cardiac arrest (aOR = 0.937, p < 0.01), and all-cause mortality (aOR = 0.647, p < 0.01). However, they had higher odds of supraventricular tachycardia (aOR = 1.307, p < 0.01), ventricular tachycardia (aOR = 1.059, p < 0.01), and events of acute kidney injury (aOR = 1.232, p < 0.01) (Table II).
Table II
Outcomes in our pre-PSM groups among cannabis users vs. non-users for all AMI cases
Propensity-score matched analyses
Our 1:1 matched sample retained 215,743 AMI cases, which included 108,103 (50.1%) with cannabis use and 107,639 (49.9%) without cannabis use. The 2 samples were statistically similar, except for a lower mean age in the cannabis users’ group (mean age: 51.24 vs. 52.92 years, p < 0.01). There were no statistically significant differences in rates of weekend admissions, sex, age groups, dyslipidaemia, smoking, diabetes, prior PCI, prior myocardial infarction, obesity, and CCI grouping. However, we found that our cohorts had slight differences in primary payer form, race, alcohol abuse, cirrhosis, hypertension, CKD, prior CABG, family history of CAD, PVD, and hospital teaching status (Table III).
Table III
Characteristics of patients ages 18–80 years admitted for acute myocardial infarction with and without a history of cannabis use between 2001 and 2020 in the United States after propensity-score matching
Cardiac arrhythmias and outcomes
In the PSM sample, cannabis users reported higher events of supraventricular tachycardia (1.5% vs. 1.3%, p < 0.01) and ventricular tachycardia (7.7% vs. 7.4%, p < 0.01) but fewer events of atrial fibrillation (7.7% vs. 8.6%, p < 0.01) and ventricular fibrillation (4.1% vs. 4.5%, p < 0.01). We noted that, just like in the pre-PSM sample, cannabis users in our PSM sample also had higher events of AKI (12.7% vs. 11.5%, p < 0.01).
However, they had fewer PCI (50.6% vs. 55.6%, p < 0.01), experienced fewer events of IABP use (3.5% vs. 4.2%, p < 0.01), and were less likely to report cardiogenic shock (3.8% vs. 5.1%, p < 0.01). Moreover, fewer events of acute ischaemic stroke (1.4% vs. 1.7%, p < 0.01), cardiac arrest (2.9% vs. 3.1%, p < 0.01), and in-hospital death (1.8% vs. 2.8%, p < 0.01) were reported in cannabis users compared to non-users. No differences were seen between the 2 cohorts for CABG procedures (9.2% vs. 9.1%, p = 0.341). Non-users had longer hospital admissions (3.86 days vs. 4.10 days, p < 0.01) (Table III).
Multivariate regression analyses
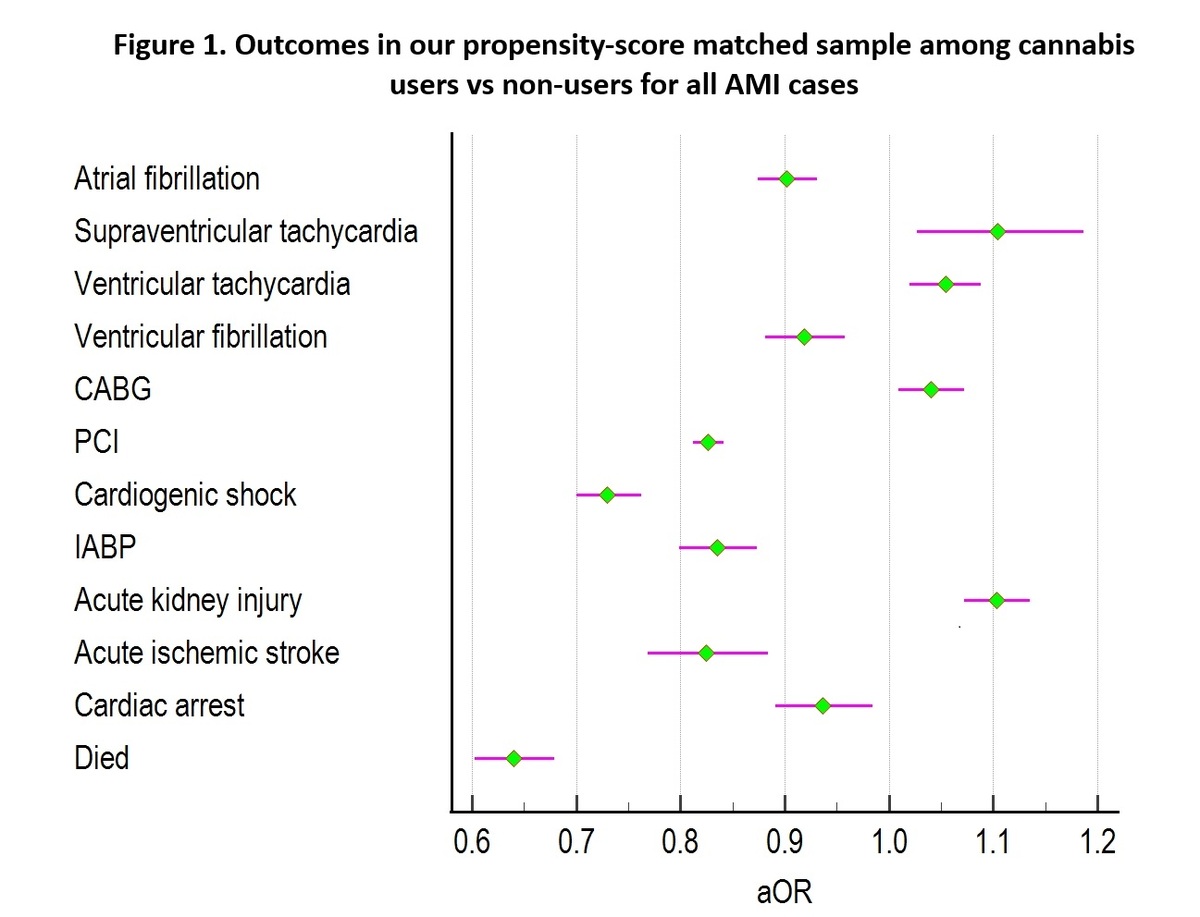
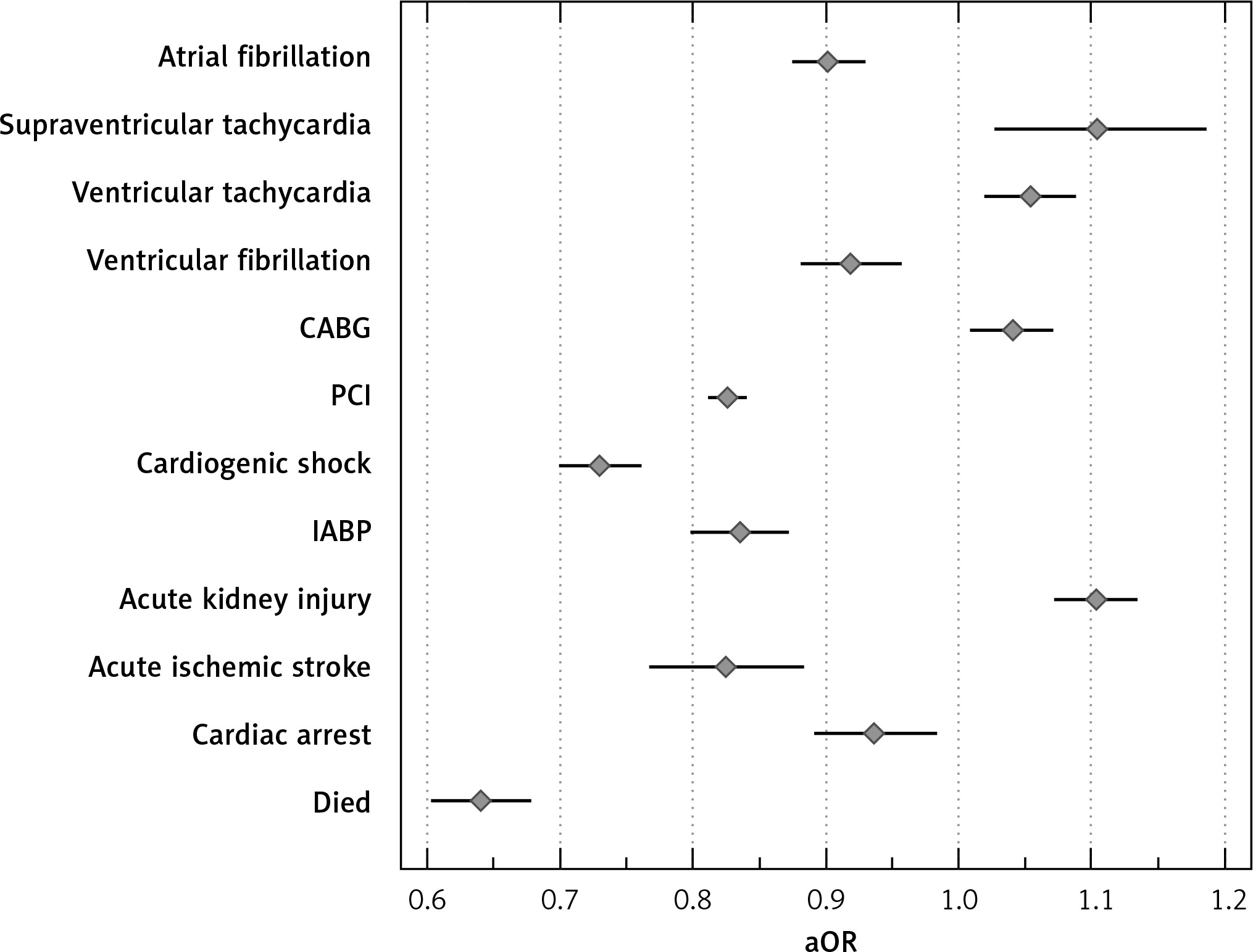
Further adjustment via multivariate regression models of our PSM sample showed that cannabis users were less likely to report atrial fibrillation (aOR = 0.902, p < 0.01), ventricular fibrillation (aOR = 0.919, p < 0.01), cardiogenic shock (aOR = 0.730, p < 0.01), acute ischaemic stroke (aOR = 0.825, p < 0.01), cardiac arrest (aOR = 0.936, p = 0.010), and all-cause mortality (aOR = 0.640, p < 0.01). They were also less likely to undergo PCI (aOR = 0.826, p < 0.01) or need IABP (aOR = 0.835, p < 0.01). However, compared to non-users, they had higher odds of having an episode with supraventricular tachycardia (aOR = 1.104, p < 0.01), ventricular tachycardia (aOR = 1.054, p < 0.01), requiring CABG (aOR = 1.040, p = 0.010), or reporting an event of AKI (aOR = 1.103, p < 0.01) (Table IV, Figure 1).
Table IV
Outcomes in our propensity-score matched sample among cannabis users vs. non-users for all AMI cases
Discussion
To our knowledge, our study is the first to conduct an in-depth assessment of the association between cannabis use and in-hospital outcomes among a representative sample of the US population admitted for AMI over 2 decades.
The primary findings from our study include the following:
Cannabis users were younger than non-users, which partially explains the differences in the prevalence of concurrent comorbidities between these groups.
Cannabis users were more likely to report supraventricular tachycardia and ventricular tachycardia but less likely to report atrial fibrillation and ventricular fibrillation.
In the context of hospitalisation for AMI, the use of cannabis was associated with lower odds of experiencing cardiogenic shock, acute ischaemic stroke, cardiac arrest, PCI use, and IABP use, but higher odds of undergoing CABG or experiencing AKI.
Cannabis users showed lower odds of all-cause in-hospital mortality when admitted for AMI.
The most startling finding of our study is that cannabis use is associated with reduced in-hospital mortality post AMI. This seemingly favourable association was also noted in 2 previous studies by Johnson-Sasso et al. and Desai et al. [31, 32]. However, we investigated the outcomes of cannabis users with AMI over a wider age range (18 to 80 years) and broader contemporary period (2001–2020) compared to the previous studies while incorporating propensity matching and multivariate regression models to adjust for possible confounding factors. The beneficial effect of cannabis use on short-term outcomes post AMI echoes the “smoker’s paradox”, whereby a similar short-term survival benefit was observed in tobacco smokers after treatment for AMI, regardless of whether they had thrombolysis or percutaneous coronary intervention [33, 34]. A few critical factors need to be considered to interpret this finding.
Firstly, cannabis users were generally younger that non-users (mean age: 51.0 vs. 62.7 years). This age difference could underlie the lower prevalence of known cardiovascular risk factors generally associated with advancing age, such as hypertension, dyslipidaemia, diabetes, chronic kidney disease, prior CABG, and peripheral vascular disease [35–38]. Meanwhile, the higher prevalence of smoking [39] and excessive alcohol intake [40] among cannabis users seen in our study mirrors what has previously been documented in the literature. Tobacco smoking has also been linked with cannabis dependence [39, 40]. While prior studies observed a lower obesity rate among cannabis users admitted for ischaemic stroke or myocardial infarction, our sample had a higher proportion of cannabis users classified as obese [30, 41, 42]. Importantly, even after propensity matching and adjusting for these potential confounders, cannabis use continued to be associated with a survival benefit in AMI.
Another factor that may explain the mortality benefit of cannabis use in AMI is the cardioprotection modulated by activation of cannabinoid receptor type 2 (CB2). Ex vivo and in vivo studies involving mice models demonstrated how CB2 agonism can be protective in the setting of myocardial ischaemia by decreasing infiltration of inflammatory cells, restricting the infarct size and limiting adverse remodeling [43, 44]. In the context of coronary reperfusion after AMI, CB2 agonism decreases the incidence of cardiac arrhythmias and reduces the area of necrosis [45]. It is plausible that AMIs in cannabis users may be smaller and have fewer fatal consequences as a result. Given that the complex mechanisms by which cannabis achieves immunomodulation remain to be fully studied and understood, the findings of studies similar to ours will hopefully provide the impetus required to drive research in this field even further.
Finally, the primary mechanism of AMI in cannabis users may differ from the most frequently seen aetiology of atherosclerotic plaque disruption causing acute thrombosis. Studies have shown the effects of cannabis in upregulating the sympathetic element of the autonomic nervous system while inhibiting the parasympathetic component, causing a rise in heart rate, increase in blood pressure, and reduction in coronary blood flow [46]. These changes can also trigger certain arrhythmias, such as supraventricular tachycardia and ventricular tachycardia, seen more commonly in cannabis users in the present study while the higher predisposition to atrial and ventricular fibrillation in our non-cannabis user cohort could be explained by age-related structural and functional remodeling specific to these arrhythmias [47–49]. Oxygen delivery to the myocardium is further compromised by the increase in blood carboxyhaemoglobin levels caused by smoke inhalation associated with cannabis intake [46]. The cumulative effect of these cannabis-induced physiological changes result in higher myocardial workload and worsening oxygen supply vs. demand mismatch, thus creating the substrate for transient myocardial ischaemia or a type 2 AMI [50]. Our observation that cannabis users were less likely to undergo PCI compared to non-users would suggest that they were less likely to have obstructing coronary artery disease as the underlying cause for their AMI.
Limitations: Our research is subject to limitations due to the retrospective nature of the data utilised. The underreporting of cannabis use due to potential stigmatisation may lead to underestimation. As the NIS relies on diagnosis and procedural codes, clinical coding mistakes and documentation errors at the hospital level may also impact the accuracy of our results [15, 16]. Given that we did not have access to data about clinical investigations and pharmacotherapy during hospitalisations, it is plausible that certain confounding factors were not identified and corrected for in the multi-variate analyses. Lastly, we cannot determine the relationship between time or amount of cannabis consumption with the AMI. We cannot adjust for historical rather than regular or recent cannabis use, which, theoretically, is less likely to predispose to AMI or influence outcomes post AMI. We expect that the large sample size analysed in our study, which is a representative sample of the US population, will mitigate some of the effects of these limitations and provide an enlightening insight.
In conclusion, the findings of our study reveal a paradox. Among patients aged 18–80 years admitted to hospital with AMI between 2001 and 2020 in the United States, cannabis use was associated with lower risks of complications, such as, cardiogenic shock, acute ischaemic stroke, cardiac arrest, and PCI use, as well as lower in-hospital mortality despite correcting for several confounding factors. This highlights how cannabis remains a poorly understood substance despite a relentless rise in consumption and social acceptance. Our study underscores the need for further research in the physiology and pharmacology of cannabinoids not only as potential therapeutic agents but also to provide the population with a more informed and nuanced understanding of the possible risks associated with cannabis consumption.