Coronary artery disease (CAD) remains a major contributor to cardiovascular disease (CVD) burden among older adults in the United States (U.S.), with an estimated 8.9 million cases in 2019, despite a recent decline in prevalence [1]. Alongside CAD, dementia affects approximately 1 in 10 older adults in the U.S., imposing significant healthcare costs projected to reach $511 billion by 2040 [2, 3]. Given the anticipated growth of the U.S. population aged 65 and older to 88.5 million by 2050 [4], the increasing burden of CAD and dementia represents a substantial public health challenge, with implications for morbidity, mortality, and healthcare costs. Emerging evidence suggests a significant link between CAD and dementia, attributed to shared risk factors and overlapping pathophysiological mechanisms. Furthermore, a high prevalence of undiagnosed cognitive impairment among older adults hospitalized with acute myocardial infarction (AMI) highlights opportunities for improved diagnosis and management strategies that may benefit patients with both CAD and dementia [5]. However, mortality trends associated with the intersection of CAD and dementia, particularly across demographic groups such as sex and race/ethnicity, remain underexplored in the U.S. This study aims to address this gap by analysing CAD- and dementia-related mortality trends in older adults from 2000 to 2020, stratified by demographic factors, using data from the Centers for Disease Control and Prevention’s (CDC) Wide-Ranging Online Data for Epidemiologic Research (WONDER) database.
We used death certificate data from the CDC WONDER Multiple Cause of Death database to analyse CAD- and dementia-related deaths among individuals aged 65 years and older in the U.S. from 2000 to 2020. Deaths were identified using the International Classification of Diseases, Tenth Revision (ICD-10) codes I20–I25 for CAD and F01, F03, and G30 for dementia; deaths in which both CAD and dementia were recorded as either underlying or contributing causes were included [6–8]. These diagnoses are based on ICD-10 coding by the certifying physician and reflect conditions documented at or near the time of death. To investigate national trends in CAD and dementia-related mortality, we calculated both crude mortality rates and age-adjusted mortality rates (AAMRs) per 100,000 individuals over the study period. Crude mortality rates were obtained by dividing the annual number of deaths by the respective U.S. population for each year, while AAMRs were standardized to the 2000 U.S. population for consistency across years [9]. We reported 95% confidence intervals (CIs) for all mortality rates. Trend analyses were conducted using the Joinpoint Regression Program (Version 5.2.0, National Cancer Institute), which calculates annual percent change (APC) and average annual percent change (AAPC) along with corresponding 95% CIs. A trend was classified as increasing or decreasing if its slope significantly differed from zero, with statistical significance assessed using two-tailed t-tests. A p-value ≤ 0.05 was considered statistically significant. A parallelism test was conducted to assess whether the trends between groups were statistically similar or divergent. A significant p-value in this interaction test indicated that the trends, based on AAPC, significantly differed between the two groups.
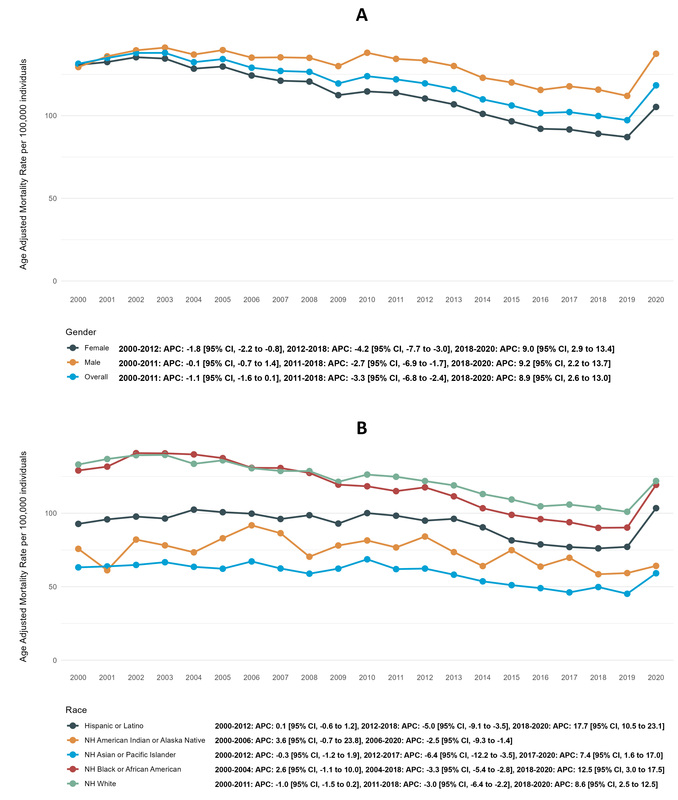
A total of 1,066,176 CAD and dementia-related deaths occurred among older adults from 2000 to 2020. Overall AAMR was 131.4 (130.2 to 132.6) in 2000 and 118.3 (117.4 to 119.3) in 2020 with an AAPC of –0.9% per year. AAMR first decreased from 2000 to 2011 (APC: –1.1%, –1.6 to 0.1), followed by a steeper decline until 2018 (APC: –3.3%, –6.8 to –2.4). A sharp rise was seen from 2018 to 2020 (APC: +8.9%, 2.6 to 13.0) (Figure 1 A).
Figure 1
Coronary artery disease and dementia-related AAMRs per 100,000 in older adults in the United States from 2000 to 2020, stratified by (A) overall and sex, and (B) race
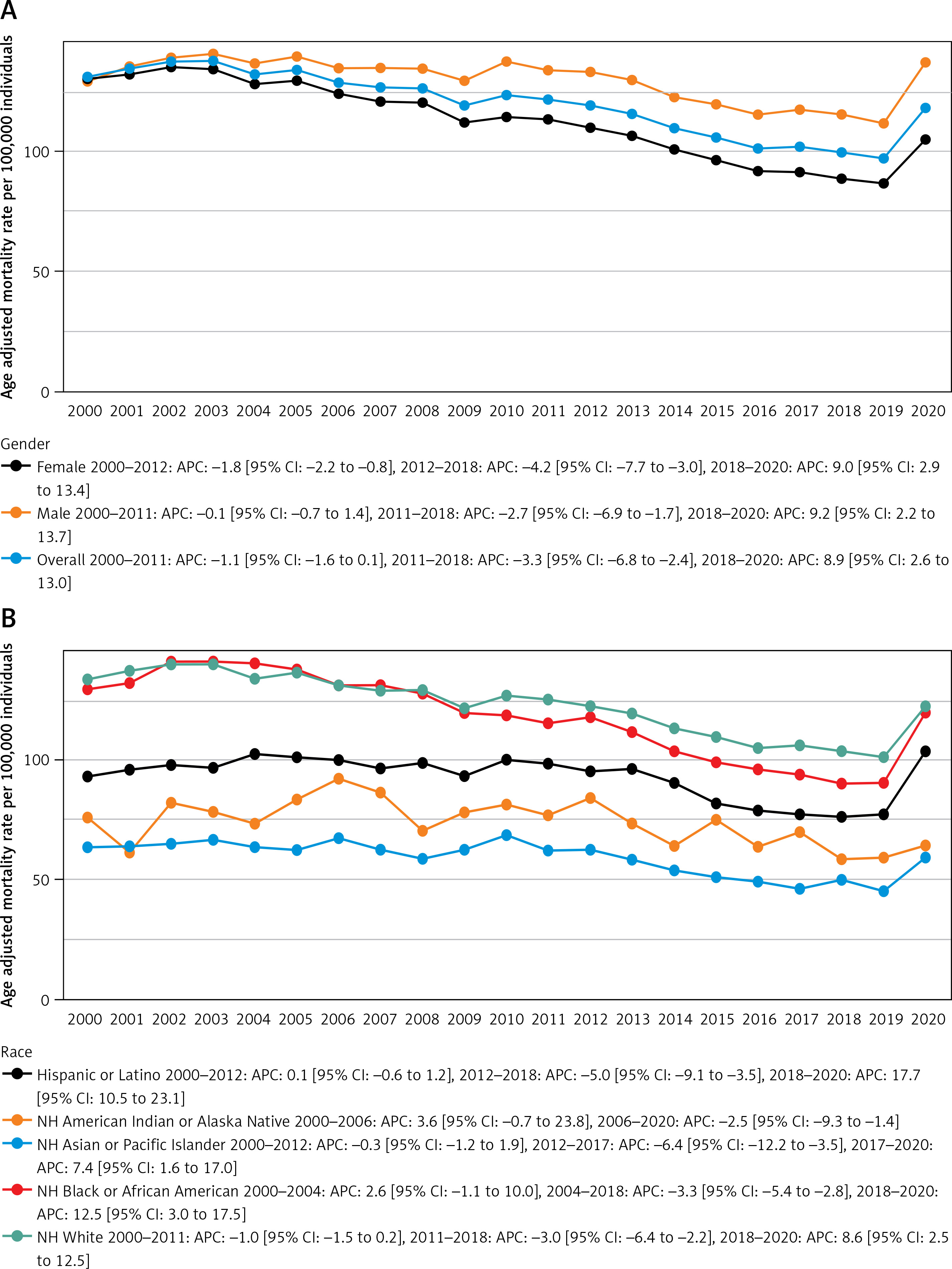
Older males consistently showed higher overall AAMRs than older females throughout the study period, with older males at 118.8 (118.6 to 119.1) and older females at 111.8 (111.5 to 112.0). The decline in AAMR was significantly larger in older females (AAPC: –1.4%, –1.8 to –1.2) compared to older males (AAPC: –0.1%, –0.6 to 0.3) (p < 0.001; Table I, Figure 1 A).
Table I
Results
Non-Hispanic (NH) White populations had the highest AAMR (121.6, 121.4 to 121.9), followed by NH Black (115.5, 114.7 to 116.3), Hispanic (90.6, 89.8 to 91.4), NH American Indian (71.8, 69.3 to 74.3) and NH Asian (56.7, 55.8 to 57.5) populations. NH Whites experienced a significant decline in AAMR (AAPC: –0.8%, –1.2 to –0.5), while AAMRs for NH Asians (AAPC: –0.7%, –1.3 to 0.0), NH American Indians (AAPC: –0.7%, –2.2 to 1.3), NH Blacks (AAPC: –0.6%, –1.3 to 0.0) and Hispanics (AAPC: +0.1%, –0.3 to 0.6) remained consistent (Figure 1 B).
In this study of CAD- and dementia-related mortality among older adults, we found that males and NH Whites, followed by NH Black populations were disproportionately affected. Prior studies have confirmed links between CAD and dementia, with CAD-related mortality generally declining over time. However, temporal trends in the co-occurrence of these conditions among the elderly remain unexplored. Our findings show an upward trend in CAD- and dementia-related mortality after 2018, accompanied by persistent demographic disparities that warrant further investigation.
The combined burden of CAD and dementia in older adults significantly worsens clinical outcomes, underscoring the need for integrated management strategies. CAD-associated vascular dysregulation has been shown to double the risk of dementia through multiple pathophysiological mechanisms, including platelet activation, which promotes amyloid-beta protein deposition – a key feature of Alzheimer’s disease [5]. Additionally, the primary underlying pathology of CAD is atherosclerosis, which also contributes to neurovascular microinfarcts that accumulate over time. This can lead to cognitive impairment and vascular dementia. Following an AMI, hypotension can lead to cerebral hypoperfusion, exacerbating neurovascular dysfunction and further contributing to dementia risk [5, 10]. CAD and dementia also share common risk factors: such as smoking, diabetes, and hypertension. The prevalence and impact of these increase with advancing age [11]. In clinical practice, elderly patients with dementia often receive less intensive treatment for CAD. This include fewer invasive procedures and reduced access to cardiac rehabilitation, resulting in poorer outcomes [12]. Cognitive impairment also complicates adherence to essential CAD medications and lifestyle modifications, impeding effective disease management [5].
Elevated AAMRs among males align with prior research showing a higher risk of mortality from both isolated and coexisting dementia and CAD. This increased risk is likely driven by a higher prevalence of shared risk factors, such as hyperlipidaemia, smoking, and a history of stroke [5, 13]. NH Whites had the highest AAMRs among racial groups, despite higher CAD prevalence in NH Black populations. This may reflect survival bias, where earlier CAD-related deaths among Blacks reduce dementia onset rates, while a larger elderly demographic in Whites increases co-occurring CAD and dementia risk. However, NH Blacks, still showed disproportionately high AAMRs compared to other non-white groups. This is likely due to increased hypertension, metabolic conditions, and nutritional factors linked to dementia, in addition to, longstanding socioeconomic and healthcare disparities [11, 14]. The sharp rise in mortality rates between 2019 and 2020 likely reflects the impact of the COVID-19 pandemic, which introduced additional mortality risks for older adults. These risks include prolonged inflammatory responses, cerebrovascular complications, and significant disruptions in cardiovascular care, all of which exacerbated health vulnerabilities in this population during the pandemic [15, 16].
The combined burden of CAD and dementia is not only driving recent increases in mortality but also highlighting opportunities to improve care strategies. Early lifestyle interventions and cognitive screening among at-risk AMI patients may help mitigate rising dementia-related healthcare demands and costs. More aggressive CAD therapies could also reduce dementia risk, though further research is necessary to identify optimal approaches for older adults with cognitive impairment [5]. Advances in neuroimaging and biomarkers are improving risk prediction, facilitating earlier intervention, and better prognosis [11].
This study has several limitations. The use of ICD-10 codes and death certificate data carries a risk of misclassification. CAD or dementia may be miscoded or omitted, particularly when other acute events are present, and certain diagnoses may be recorded based on clinical suspicion rather than confirmatory testing. This may lead to under- or overestimation of the true burden, consistent with prior mortality studies using death certificate data. Lack of data on cardiovascular risks, comorbidities, management, and socioeconomic factors also limits insights. Furthermore, as this is an observational analysis of death certificate data, no direct causal inferences can be made from the reported associations.
Despite overall declines in CAD- and dementia-related mortality, demographic disparities persist, with males and NH Whites facing worse outcomes. Furthermore, all cohorts showed increasing mortality trends from 2018 onward, raising significant concerns. Our identification of potentially vulnerable groups in the U.S. highlights areas for further research and the potential for developing risk assessment strategies, while suggesting that tailored management may help improve mortality outcomes in older adults.