Introduction
Acute myocardial infarction (AMI) is characterized by the lack of oxygen and necrosis of the myocardium due to low or interrupted blood supply to one or more coronary arteries [1]. This disease negatively affects the psychological health of the patients due to the high morbidity and mortality rates, the severity of clinical symptoms, the possibility of economic and social problems, disabilities due to the disease, and lifestyle change requirements. The prevalence of anxiety and depression increase in patients with myocardial infarction history [2]. Individuals may experience intense stress after MI diagnosis. This stress could lead to anxiety due to the uncertainty of the treatment process, concerns about another MI especially while alone, and fear of death [3]. However, not all patients with MI history exhibit similar psychological responses. Patients’ past experiences, traumatic experiences, social support systems, economic and environmental factors, personality traits, and coping and defence mechanisms play an important role in the differentiation of psychological and behavioural responses that may be observed after the disease [4]. The literature review revealed that certain studies reported increased anxiety and depression symptoms immediately after MI or later [5, 6]. However, there was no study on the correlation between these stress-induced psychological symptoms and the defence mechanisms adopted by myocardial infarction patients.
Thus, the present study aimed to investigate the correlations between anxiety, depression symptoms, defence mechanisms, and other clinical and socio-demographic data in patients with MI history.
Material and methods
Local Ethics Committee approval was obtained for the present study, and the study was conducted according to the Helsinki Declaration. Sixty patients, who were admitted to the cardiology outpatient clinic with chest pain, diagnosed with myocardial infarction, hospitalized in the cardiology department, and were organically stable, were included in the study. Patient sociodemographic information was recorded. The Beck Depression Scale, Beck Anxiety Scale, and Defence Styles Questionnaire were applied. The inclusion criteria included age 40–70 years, literacy, and acceptance of the informed consent form. During the application of the scales, patients with neurological or other physical diseases and psychiatric diseases that would prevent patient cooperation and communication were excluded from the study. The study was carried out between February 2019 and April 2019.
Method
Patients who applied to Firat University Cardiology Outpatient Clinic with complaints of chest pain and diagnosed with MI were interviewed after they were stable (on average, one week after admission). The patients were informed about the study, and they signed the informed consent form, then a psychiatrist applied the Defence Styles Questionnaire, Beck Depression Inventory, and Beck Anxiety Inventory. Patient sociodemographic information such as age, marital status, education level, occupation, gender, place of residence, and income level was recorded in a sociodemographic data form.
Data collection instruments
Sociodemographic and clinical data form
A sociodemographic and clinical data form developed by the authors based on the clinical experience and the information obtained in the literature review and the aims of the study was employed to collect personal data. The form was a semi-structured form that aimed to determine patient sociodemographic information such as age, gender, marital status, education level, occupation, place of residence, income level, and family structure.
Beck Depression Scale
The 21-item, 3-point, Likert-type self-report scale was developed by Beck in 1961 and measures the physical, emotional, cognitive, and motivational depression symptoms [7]. A scale score of 17 or above is considered depression that requires clinical intervention. The Turkish validity and reliability of the scale were determined in 1989 by Hisli [8].
Defence Styles Questionnaire (DSQ)
The Defence Styles Questionnaire, developed by Andrews et al., is an 88-item self-report test that analyses 26 defence styles [9]. The construct validity analysis demonstrated that the defence styles in DSQ included 4 factors: immature defence styles, image perversion defence styles, self-hiding defence styles, and mature defence styles. Later, the total number of items was reduced to 40, which included immature, mature, and neurotic styles. Immature (primitive) defences include reflection, passive aggression, expression, isolation, devaluation, autistic fantasy, negation, displacement, dissociation, division, rationalization, and somatization sub-factors. Neurotic defences include undoing, pseudo-altruism, idealization, and reaction formation subscales. Mature defences include sublimation, humour, suppression, and anticipation subscales. The immature defence scores vary between 24 and 216, the neurotic defence score varies between 8 and 72, and the mature defence score varies between 8 and 72.
Beck Anxiety Inventory
The inventory measures the frequency of anxiety symptoms experienced by an individual. It is a 3-point Likert-type self-report scale that includes 21 items. A high total score indicates high anxiety. The inventory was developed by Beck et al. [10].
Statistical analysis
SPSS for Windows v. 22.0 software was employed for the data analysis. The t-test was used for unpaired comparisons, and the χ2 test was used for categorical comparisons. In data analysis, frequencies, percentages, and the arithmetic mean and standard deviation were calculated. The correlations between the scale scores were determined with Pearson correlation analysis.
Results
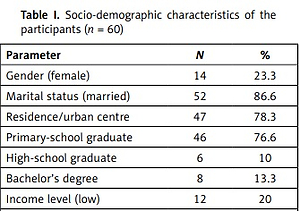
It was determined that the mean age of the participants was 61.07 ±11.02 years. Twenty-three percent of the patients were female (14) and 77% were male (46). Thirty-eight participants had MI once, 7 had it twice, and 15 had it more than twice. The number of patients who underwent diagnostic angiography was 31. Stents had been placed in 22 patients previously. The families of 36 patients had a history of heart disease. First-degree relatives of 26 patients died of heart disease, while relatives of 30 patients died of heart disease. Other socio-demographic patient characteristics are summarized in Table I.
Table I
Socio-demographic characteristics of the participants (n = 60)
The mean BDI score of the participants was 15.9 ±11.2, the mean DSQ score was 15.98 ±10.9, the mean immature defence mechanism score was 102.6 ±31.02, the mean neurotic defence mechanism score was 47.28 ±10.12, and the mean mature defence mechanism score was 44.63 ±11.62. There was a positive correlation between depression and immature defence mechanism scores of the participants, and a negative correlation between depression and mature defence mechanism scores. A negative correlation was determined between anxiety and mature defence mechanism scores (Table II).
Table II
Evaluation of scale scores with correlation analysis
| Age | BDI | BAI | DSQ immature total | DSQ neurotic total | DSQ mature total | ||
|---|---|---|---|---|---|---|---|
| Age | r | 1 | 0.233 | 0.121 | 0.069 | 0.062 | –0.001 |
| p | 0.074 | 0.356 | 0.599 | 0.640 | 0.993 | ||
| BDI | r | 0.233 | 1 | 0.624** | 0.412** | 0.095 | –0.359** |
| p | 0.074 | 0.000 | 0.001 | 0.468 | 0.005 | ||
| BAI | r | 0.121 | 0.624** | 1 | 0.238 | –0.116 | –0.397** |
| p | 0.356 | 0.000 | 0.067 | 0.376 | 0.002 | ||
| DSQ immature total | r | 0.069 | 0.412** | 0.238 | 1 | 0.432** | 0.162 |
| p | 0.599 | 0.001 | 0.067 | 0.001 | 0.215 | ||
| DSQ neurotic total | r | 0.062 | 0.095 | –0.116 | 0.432** | 1 | 0.566** |
| p | 0.640 | 0.468 | 0.376 | 0.001 | 0.000 | ||
| DSQ mature total | r | –0.001 | –0.359** | –0.397** | 0.162 | 0.566** | 1 |
| p | 0.993 | 0.005 | 0.002 | 0.215 | 0.000 | ||
The classification based on the anxiety scale revealed mild anxiety in 18 (30%) participants, moderate anxiety in 19 (32%) participants, and severe anxiety in 8 (13%) participants.
The inter-scale comparisons based on gender revealed no difference between male and female defence mechanism scores. However, the mean BDI scale score and the mean BAI score of females were statistically significantly higher when compared to those of males (p = 0.012, p = 0.015, respectively). The BDI and BAI scores of 44 patients with a comorbid disease were significantly higher when compared to those without a comorbid disease (p = 0.009, p = 0.024, respectively).
Participants with BDI scores of 17 and above were divided into 2 groups with depression (26 patients) and without depression (34 patients), and their defence mechanism sub-scale and total scores were compared (Table III). The total immature defence mechanism score of the group with depression was statistically significantly higher when compared to the group without depression. The immature defence mechanism subscale scores, except dissociation, were higher in the group with depression when compared to the group without depression.
Table III
Comparison of scale scores of the patients with and without depression
| Scale | Depression (+) N = 26 | Depression (–) N = 34 | P-value | t |
|---|---|---|---|---|
| BDI | 26.6 ±7.9 | 7.64 ±4.44 | 0.000* | –11.792 |
| BAI | 23.9 ±10.03 | 9.94 ±7.09 | 0.000* | –6.306 |
| DSQ immature total | 112.2 ±27.9 | 95.2 ±31.7 | 0.034* | –2.168 |
| DSQ neurotic total | 47.2 ±10.8 | 47.4 ±9.73 | 0.952 | 0.060 |
| DSQ mature total | 40.0 ±11.5 | 48.18 ±10.5 | 0.006* | 2.862 |
However, only the differences between passive aggression and somatization subscale scores were statistically significant (p = 0.033, p = 0.008) (Table IV).
Table IV
Comparison of immature defence mechanism subscale scores of patients with and without depression
| Variable | Depression (+) N = 26 | Depression (–) N = 34 | P-value | t |
|---|---|---|---|---|
| Reflection | 9.85 ±3.46 | 8.24 ±4.33 | 0.126 | –1.553 |
| Passive aggression | 7.85 ±4.06 | 5.62 ±3.82 | 0.033* | –2.179 |
| Acting out | 9.0 ±5.61 | 7.0 ±4.99 | 0.151 | –1.456 |
| Isolation | 9.08 ±4.69 | 8.62 ±4.91 | 0.716 | –0.366 |
| Devaluation | 8.73 ±4.54 | 6.85 ±4.14 | 0.1 | –1.671 |
| Autistic fantasy | 9.42 ±5.80 | 8.5 ±5.14 | 0.517 | –0.652 |
| Denial | 10.7 ±4.69 | 9.82 ±4.98 | 0.514 | –0.656 |
| Displacement | 8.89 ±5.38 | 7.71 ±4.69 | 0.370 | –0.904 |
| Dissociation | 6.77 ±4.68 | 8.71 ±4.62 | 0.115 | 1.601 |
| Splitting | 9.69 ±3.5 | 8.18 ±4.36 | 0.152 | –1.451 |
| Rationalization | 7.65 ±4.81 | 6.85 ±4.57 | 0.513 | –0.657 |
| Somatization | 12.6 ±4.15 | 9.47 ±4.49 | 0.008* | –2.744 |
| Immature total | 112.2 ±27.9 | 95.2 ±31.7 | 0.034* | –2.168 |
The total mature defence mechanism score of the group with depression was significantly lower when compared to the group without depression. All mature defence mechanism subscale scores were lower in the group with depression when compared to the group without depression. However, only the difference in low sublimation subscale scores was statistically significant (p = 0.008) (Table V).
Table V
Comparison of the mature defence mechanism subscale scores of the patients with and without depression
| Variable | Depression (+) N = 26 | Depression (–) N = 34 | P-value | t |
|---|---|---|---|---|
| Sublimation | 10.8 ±4.25 | 14.0 ±4.64 | 0.008* | 2.764 |
| Humour | 7.54 ±4.4 | 9.15 ±4.22 | 0.156 | 1.437 |
| Suppression | 10.9 ±5.81 | 13.3 ±4.87 | 0.09 | 1.726 |
| Anticipation | 10.6 ±4.14 | 11.5 ±4.0 | 0.407 | 0.836 |
| Mature total | 40.0 ±11.5 | 48.2 ±10.5 | 0.006* | 2.862 |
Discussion
The present study findings revealed that anxiety and depression scores were higher in patients with MI history, and there was a significant correlation between the adopted defence mechanisms and the anxiety and depression scores. It was also determined that there was a positive correlation between the depression scores of all participants and immature defence mechanism scores. The group with clinically significant depression scores had higher total immature defence mechanism scores and lower mature defence mechanism scores when compared to the group without depression. Furthermore, as the anxiety scores of all participating patients increased, their mature defence mechanism scores decreased, and there was a negative correlation between these 2 variables.
It is always possible for the individual to face a stress factor that affects the quality of life and disrupts her or his balance in daily life. For example, a diagnosis of a disease with severe clinical symptoms or a high mortality rate could occur suddenly and disrupt the balance of most individuals. To protect the psychological balance in the face of a disease, the individual could develop certain psychosocial responses such as cognitive, emotional, and behavioural responses [11]. MI may also lead to certain psychosocial reactions because it is a life-threatening disease that requires intensive care treatment, restriction of mobility leads to severe pain, insomnia, and concerns and anxiety about the future. However, people can have a variety of psychosocial reactions to severe disease. The type of psychosocial response to disease can vary based on the patient’s perception of the disease, personality traits, and defence and coping mechanisms [12].
It is known that anxiety is the earliest psychological response to acute myocardial infarction. There is evidence that MI increases the risk of anxiety and depression disorder during the first 2 years after MI, and post-MI anxiety disorders are associated with recurrent MI risk [13]. In a study conducted in 2018, anxiety symptoms were evaluated 2 and 12 months after hospitalization of the MI patients, and anxiety symptoms were observed in 38% and 33% of these patients, respectively. It was found that depression/anxiety history, female gender, young age, smoking, and heart disease history were strongly associated with post-MI anxiety [14]. In the present study, the anxiety levels of MI patients were higher, which is consistent with the literature, and 45% of the patients exhibited moderate or severe anxiety symptoms.
It was determined that 43% of the patients exhibited clinical depression symptoms. Deveci et al. applied BDI to patients who had MI for the first time, were treated in the intensive care unit, and were then transferred to the cardiology service. In the study, the depression score (17 and higher) of 31.0% of patients was consistent with clinically significant depression. In the same study, it was found that the rate of clinical depression was significantly higher among women when compared to men [15]. In another study, it was reported that post-MI anxiety symptoms were not an independent prognostic risk factor for new cardiovascular events or death, while depression symptoms were associated with increased mortality [16]. In a study conducted in 2017, 250 post-MI patients were interviewed 72 h after their admission to the hospital, and the Hospital Anxiety and Depression Scale was applied. In the study, it was reported that female patients were more anxious and exhibited higher complication levels when compared to male patients [17]. In the present study, both anxiety and depression scores of females were higher when compared to males, which is consistent with the literature.
One of the important results of the present study was that the immature defence mechanism scores of depressive patients were higher and their mature defence mechanism scores were lower when compared to the patients without depression. The psychological processes called defence mechanisms are specific, unconscious, intrapsychic adjustments that resolve conflicts and reduce anxiety. They play a key role in the development of personality and the adaptation of the individual to the environment, and they protect the individual from internal conflicts and emotional distress. Thus, defence mechanisms play an active role in ego development and the determination of behavioural patterns, as well as controlling anxiety and other affective states [18].
Defence mechanisms are scrutinized based on 3 groups: immature, neurotic, and mature mechanisms. Immature defence mechanisms are the most primitive defence styles and are generally observed during the initial years of life; they are inadequate for harmony between impulses and environmental realities [19]. Immature (primitive) defences are classified as reflection, passive aggression, expression, isolation, devaluation, autistic fantasy, negation, displacement, dissociation, division, rationalization, and somatization. Immature defences and neurotic defences are mostly adopted by individuals with various psychopathological conditions [20].
Mature defence mechanisms, on the other hand, allow the individual to establish a harmonious and beneficial balance between impulses and environmental realities and reduce psychological stress and anxiety [21]. These defence mechanisms, which mostly originate from immature defences, are adopted by healthy individuals [22]. When the defence mechanisms are adopted properly and when required, they can protect the individual, allow the individual to cope with stress, and reduce anxiety. However, the use of inadequate defence mechanisms by patients, like those with a history of MI, may increase their psychological burden, which could be considered natural in the beginning and could lead to psychological disorders and difficulties in the follow-up and treatment of the disease [23, 24].
Carvalho conducted a large-scale study with 9937 subjects. The results of the study that investigated the correlation between defence mechanisms and depression disorder revealed that high-level immature defence mechanism and low-level mature defence mechanism use were independently associated with depression symptoms [25]. In the present study, there was a positive correlation between depression and immature defence mechanisms in MI patients and a negative correlation between depression and mature defence mechanisms.
Furthermore, a negative correlation was determined between anxiety and mature defence mechanism scores in the present study. Because mature defences are adopted to alleviate or eliminate the effects of undesired events or situations, the inability to utilize these defences could lead to increased anxiety levels. In previous studies, positive correlations between anxiety levels and primitive defence mechanisms such as reflection, denial, displacement, and passive aggression were reported [26]. This was a predictable result because, in individuals with depression, high anxiety symptoms accompany the disease. Thus, individuals with high anxiety are expected to have lower maturity defence scores and higher immature defence mechanism scores. However, in the present study, no correlation was determined between immature defence mechanisms and anxiety scores. In our study, because the patient evaluations were conducted early in the post-MI period, similar findings could be observed when the defence mechanisms adopted by the same patients are re-evaluated in the future.
In clinical applications, it is important to determine the post-physical disease psychological symptoms and the defence mechanisms adopted by the individual to develop an adequate treatment plan. It is well known that stress-reducing interventions in post-MI patients may reduce the risk of the development of a new coronary event [27]. Thus, interventions such as the determination of immature defences adopted by MI patients with anxiety or depression symptoms, elimination of cognitive problems, and guidance of the patients to use mature defences such as humour, anticipation, and exaltation should be included in the treatment plan. However, for this, it is necessary to raise the awareness of health professionals with in-service training about the timing, development, and functionality of the defence mechanisms, when they are pathological, and when they could be protective. It was also observed that psychiatrists should cooperate with healthcare professionals in the cardiology department for the diagnosis and treatment of psychological problems that may develop in MI patients.
The present study has certain limitations. Because defence styles are unconscious processes, the analysis of these processes with a self-reporting scale may have led to certain errors. Also, although the number of patients included in the study was adequate for analysis, further studies conducted with a larger sample would report more comprehensive findings.