Introduction
Disseminated intravascular coagulation (DIC) is a serious condition with a high mortality rate and a major challenge to clinicians. In the United States, a study analyzing hospital admissions in 2016 found that there were approximately 8,704 cases of DIC, with a mortality rate of 47.7% [1, 2]. The main etiology behind DIC, which is associated with the highest mortality rates, is sepsis, with an incidences rate of 55.5% of all causes of DIC cases from 2002 to 2014 [1, 3]. It is associated with mortality ranging from 45% to 78% during hospitalizations [4]. Elderly populations are particularly at risk for DIC due to the low-grade, systemic, pro-inflammatory state associated with aging [5]. The incidence of DIC in men has decreased significantly over the past decade, although the mortality rate remains the same [6]. Disseminated intravascular coagulation may result as a complication of infection, solid cancers, hematological malignancies, obstetric diseases, trauma, aneurysms, and liver diseases, etc., each of which presents characteristic features related to the underlying disorder [7]. It is a strong predictor of death and multiple organ failure in patients with septic shock. Mortality risks have been demonstrated to double in critically ill patients if DIC occurs [8–10].
Identifying the demographic distribution of DIC-related mortality can help identify populations at the highest risk so that timely targeted interventions can be provided. Therefore, we sought to evaluate demographic differences in DIC-related mortality from 1999 to 2020 among adults > 65 years of age within the United States.
Material and methods
Population and study setting
This was a retrospective, population-based study using publicly available mortality data from the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research (CDC WONDER) database. The study used codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10).
The study population includes individuals 65 years and older, identified through death certificates that listed DIC (ICD-10 code: D65) and the underlying cause of death i.e., circulatory (ICD-10 code: I00-I99), poisoning (ICD-10 code: T36-T88), and cancer (ICD-10 code: C00-C97). The study was exempt from institutional review board approval because the CDC WONDER database contains anonymized, publicly available data. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed in this study [11].
Data abstraction
Data were extracted for all 50 states in the United States and the District of Columbia, from the years 1999 to 2020. The data were collected on demographic factors including age, sex, and race/ethnicity, as well as the place of death, categorized as medical facilities, nursing or long-term care facilities, hospices, the decedent’s home, or other unspecified locations. Ethnicity was categorized as non-Hispanic (NH) White, NH Black or African American, NH American Indian or Alaskan Native, NH Asian or Pacific Islander, and Hispanic or Latino [12]. The geographical data were classified into metropolitan areas, comprising large metropolitan regions (populations over 1 million) and small to medium metropolitan regions (50,000 to 1 million), and nonmetropolitan areas with populations below 50,000, based on the NCHS Urban-Rural Classification Scheme for Counties. Furthermore, the United States was divided into four regions – Northeast, Midwest, South, and West – following the classification established by the U.S. Census Bureau’s classification [13].
Statistical analysis
Age-adjusted mortality rates (AAMRs) and crude mortality rates per 100,000 individuals, along with 95% confidence intervals (CI), were calculated. These rates were stratified based on year, gender, race/ethnicity, and region. Crude mortality rates were computed by dividing the number of deaths attributed to DIC by the corresponding U.S. population for each respective year. AAMRs were standardized to the 2000 US population [14]. The Joinpoint Regression Program (Joinpoint V 5·2·0·0, National Cancer Institute) was used to determine the annual percent change (APC) with a 95% CI in AAMR [15]. It uses log-linear regression models for the mortality data, allowing the calculation of annual percent change (APC) with 95 % confidence intervals (CI). An empirical quantile method was used to determine whether the APC and AAPCs indicated an increase or decrease in mortality over the time interval. Statistical significance was evaluated at p ≤ 0.05.
Results
A total of 36,853 deaths related to DIC were reported in older adults (aged ≥ 65 years) from 1999 to 2020. Of these, 93.1% occurred in medical facilities, 2.4% in nursing homes/long-term care facilities, 2.3% at home, and 1.2% in hospice care. The results were further stratified by overall trends, sex, race or ethnicity, and geographical regions. (Supplementary Table SI).
Overall annual trends for DIC-related AAMR
The overall age-adjusted mortality rate (AAMR) for DIC declined from 6.4 per 100,000 (95% CI: 6.1 to 6.7) in 1999 to 4.0 (95% CI: 3.8 to 4.1) in 2020, with an average annual percentage change (AAPC) of –2.4 (95% CI: –2.9 to –2.0). AAMR decreased from 1999 to 2004, with an annual percentage change (APC) value of –4.9 (95% CI: –7.9 to –3.3), and continued decreasing at a steady rate until 2015 (APC = –3.1; 95% CI: –5.7 to 0.2), followed by an increase from 2015 to 2020 (APC = 1.7; 95% CI: –1.4 to 7.9) (Figure 1, Supplemental Table SII).
DIC-related AAMR stratified by sex
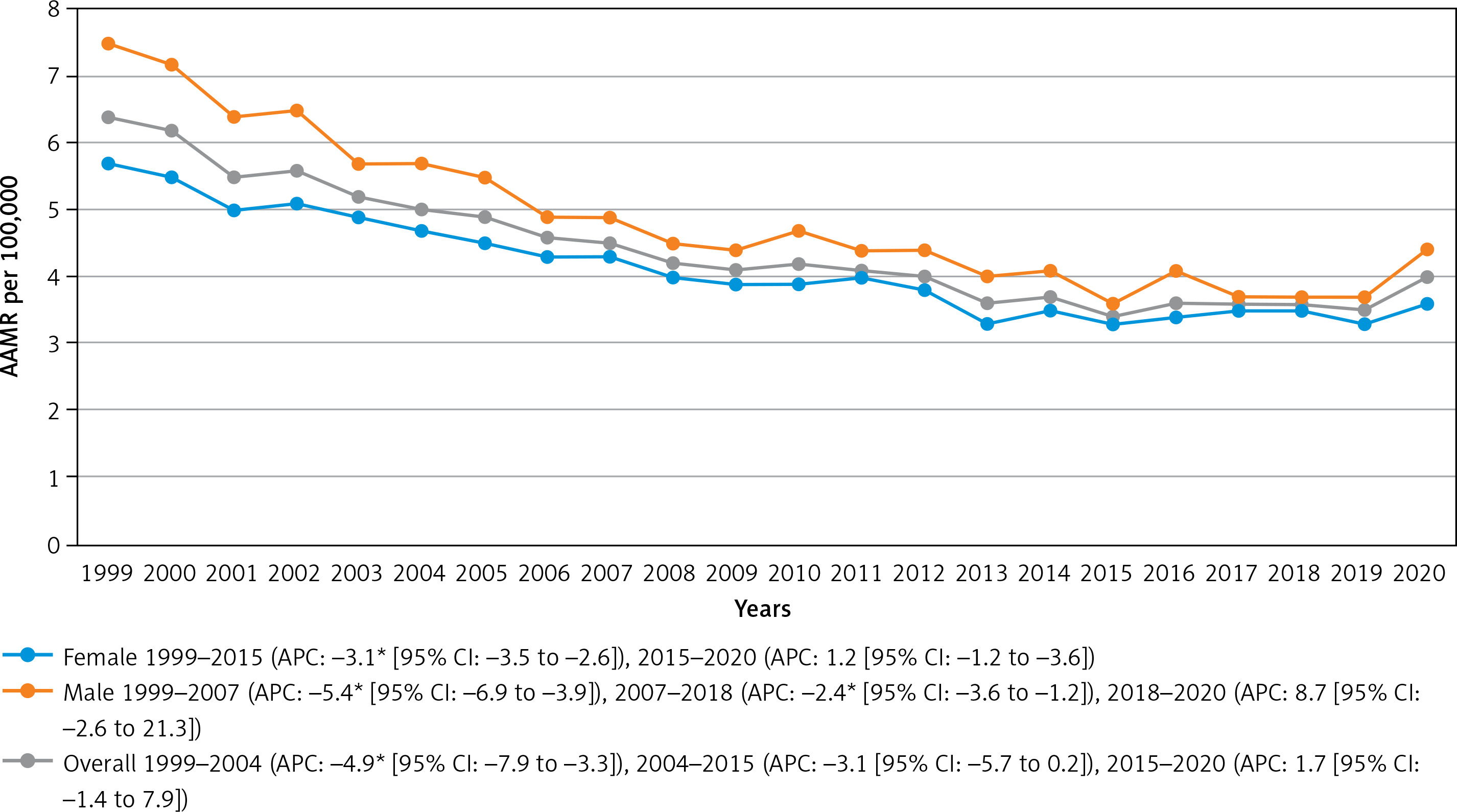
Among DIC-related deaths, 21,647 (54.3%) occurred in women (AAMR = 4.1; 95% CI: 4 to 4.1), and 18,206 (45.7%) occurred in men (AAMR = 4.8; 95% CI: 4.7 to 4.8). In men, overall, there was a decreasing trend from 1999 to 2020 (AAPC = –2.6; 95% CI: –3.8 to –1.3). AAMR in men decreased from 7.5 in 1999 to 4.9 in 2007 (APC = –5.4; 95% CI: –6.9 to –3.9) and continued decreasing to 3.7 until 2018 (APC = –2.4; 95% CI: –3.6 to –1.2), followed by an increase to 4.4 in 2020 (APC = 8.7; 95% CI: –2.6 to 21.3). Similarly, in females, AAMR declined from 1999 to 2020 (AAPC = –2.1; 95% CI: –2.7 to –1.5). AAMR declined from 5.7 in 1999 to 3.3 in 2015 (APC = –3.1; 95% CI: –3.5 to –2.6), followed by a slight increase to an AAMR of 3.6 by 2020 (APC = 1.2; 95% CI: –1.2 to –3.6) (Figure 1, Supplementary Table SII).
DIC-related AAMR stratified by race
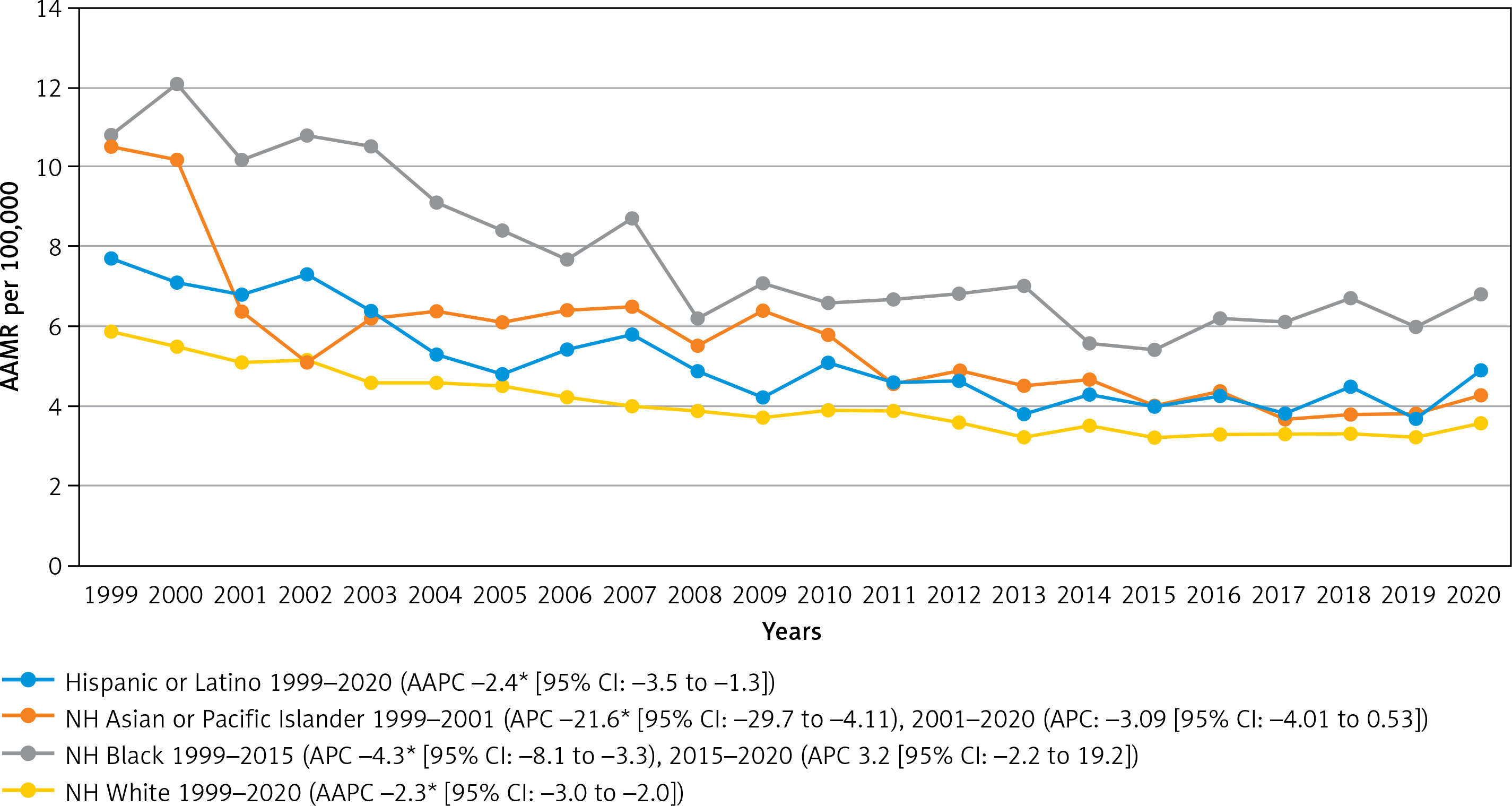
In terms of racial/ethnic distribution, the highest mortality rate during the study period was observed in NH African American or Black patients, with an AAMR of 7.6 (95% CI: 7.4 to 7.8), and the lowest in NH White patients, with an AAMR of 4.0 (95% CI: 3.9 to 4.0) (Supplementary Table SIII). In NH African Americans, the AAMR was 10.8 in 1999 and declined to 5.4 by 2015 (APC = –4.3; 95% CI: –8.1 to –3.3), followed by a rise to 6.8 until 2020 (APC = 3.2; 95% CI: –2.2 to 19.2). The AAMR in Asians or Pacific Islanders decreased sharply from 10.5 in 1999 to 6.4 in 2001 (APC = –21.6; 95% CI: –29.7 to –4.1) and then continued decreasing steadily until the end of the study period, reaching 4.3 (APC = –3.1; 95% CI: –4.01 to 0.53). The AAMR in NH Whites and Hispanics showed a steady decline during the study period, with an average APC of –2.3 (95% CI: –3.0 to –2.0) in NH Whites and –2.4 (95% CI: –3.5 to –1.3) in Hispanics, respectively (Figure 2, Supplementary Table SIII).
DIC-related AAMR stratified by age
The AAMR was highest for the age group of 85+ years, followed by 75–84 years, and lowest for 65–74 years. The people in the age group 85+ years showed a steady decrease from 1999 to 2020 (AAPC = –4.2; 95% CI: –4.6 to –3.7). The population aged 75–84 years showed a steep decline from 1999 to 2008 (APC = –4.3; 95% CI: –5.4 to –3.3) followed by a gradual decline until 2020 (APC = –1.6; 95% CI: –2.8 to –0.6). The patients in the group aged 65–74 years had a sharp declining trend from 1999 to 2006 (APC = –4.8; 95% CI: –6.1 to –3.5) followed by a gradual decline until 2016 (APC = –1.9; 95% CI: –2.8 to –1.1) and then a rise until 2020 (APC = 4.9; 95% CI: 1.9 to 8) (Supplementary Figure S1, Supplementary Table SIV).
DIC-related AAMR stratified by geographic region
A slight variation in AAMR was noted in different regions, with the AAMR being highest in the Southern region (AAMR = 4.6; 95% CI: 4.5 to 4.6), followed by the Northeastern (AAMR = 4.5; 95% CI: 4.4 to 4.6), Western (AAMR = 4.2; 95% CI: 4.1 to 4.3), and Midwestern regions (AAMR = 4.0; 95% CI: 4.0 to 4.1). All regions showed a declining trend in AAMR from 1999 to 2020 (Supplementary Figure S2, Supplementary Table SV).
The AAMR in metropolitan areas was 7.6 in 1999, which decreased to 3.9 in 2020 (AAPC = –2.3; 95% CI: –3.04 to –1.54), and the AAMR in nonmetropolitan areas decreased from 6.2 to 4.5 (AAPC = –1.94; 95% CI: –2.98 to –0.89). The AAMR decreased in metropolitan areas from 1999 to 2015 (APC = –3.56; 95% CI: –3.99 to –3.11), followed by a slight increase from 2015 to 2020. Similarly, the AAMR in nonmetropolitan areas decreased from 1999 to 2013 (APC = –3.76; 95% CI: –4.71 to –2.80), followed by a gradual increase from 2013 to 2020 (Supplementary Figure S3, Supplementary Table SVI).
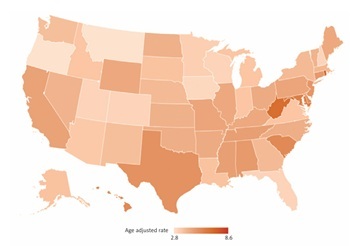
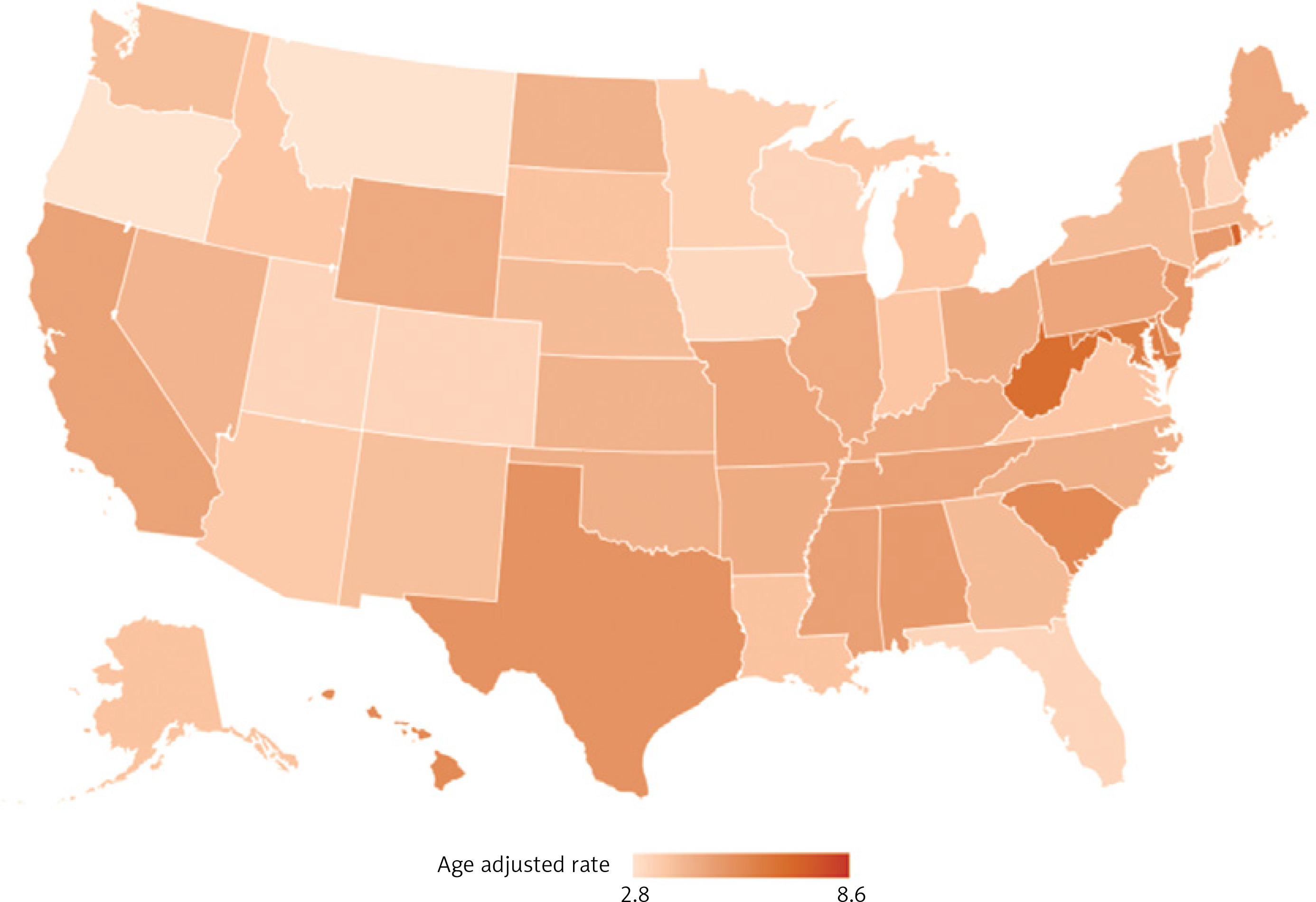
States exhibited significant differences in AAMR, with values ranging from 8.6 in the District of Columbia to 2.8 in Montana. States in the upper 90th percentile of AAMRs included the District of Columbia, Rhode Island, West Virginia, Maryland, and Hawaii. These states had AAMRs that were nearly three times higher than those in the lower 10th percentile, which included New Hampshire, Colorado, Iowa, Oregon, and Montana (Supplementary Table SVII, Figure 3).
Underlying causes of death in DIC-related mortalities
Among older adults with DIC-related deaths, the most commonly reported underlying causes were circulatory system diseases, malignancies, and poisoning. Circulatory conditions were the leading contributors, with AAMR decreasing from 3.51 in 1999 to 2.22 in 2020 (AAPC = –2.19; 95% CI: –2.95 to –1.42). The AAMR for circulatory causes declined from 1999 to 2015 (APC = –3.75; 95% CI: –4.29 to –3.20), followed by an increase from 2015 to 2020 (APC = 2.99; 95% CI: –0.10 to 6.17). Cancer–related deaths ranked second and also showed a declining trend, with AAMR declining from 1.76 to 0.99 during the study period (AAPC = –2.60, 95% CI: –3.48 to –1.70). Poisoning-related deaths also declined with AAMR decreasing from 0.42 in 1999 to 0.16 in 2020 (AAPC = –3.63; 95% CI: –8.22 to –1.19) (Supplementary Table SVIII, Figure 4).

Discussion
This analysis of mortality data for the period 1999-2020 from the Centers of Disease Control and Prevention database shows a few key insights. Our findings indicate an overall decline in DIC-related mortality, with AAMR decreasing from 6.4 per 100,000 in 1999 to 4.0 per 100,000 in 2020. Almost all subgroups revealed a decrease in AAMR until 2015, followed by a steep rise at the end of the study period. The older men experienced higher mortality as compared to the women. The NH Blacks had the highest DIC-related AAMR compared with other racial groups in this age stratum > 65 years. Specific geographical locations, such as the District of Columbia, Rhode Island, West Virginia, Maryland, and Hawaii, consistently exhibited high morbidity rates for DIC throughout the study period. Moreover, metropolitan areas demonstrated consistently higher mortality rates compared with nonmetropolitan areas.
According to some studies, the incidence of DIC has decreased over the past decade, whereas the case fatality rate has not changed significantly [1]. However, in our study, a notable increase in AAMR was observed in the latter part of the study period (2015–2020), indicating a potential shift in underlying risk factors, healthcare interventions, or diagnostic practices. The initial steep decline until 2015 aligns with advancements in critical care and anticoagulation therapies. However, the subsequent increase from 2015 to 2020 warrants further investigation, as it could reflect an increase in underlying conditions predisposing older adults to DIC, the onset of the COVID-19 pandemic, or an ageing population with more comorbidities. These findings highlight the urgent need to improve rural healthcare access, especially for older individuals disproportionately affected by worsening DIC outcomes [2].
The common causes of DIC in the elderly population include sepsis and cancer, especially acute myeloid leukemia (AML) [5]. The increase in the burden of cardiovascular diseases, heat illness, vascular disorders, and blood and immune disorders in the aged population has also led to more critical care admissions and life-threatening conditions [16, 17]. Some studies claim that sepsis in the geriatric population leads to an almost 38 times increased mortality rate [18]. The contributing factors may include lower treatment uptake for DIC, risk factors such as infections, injuries, sedentary lifestyle leading to obesity, substance abuse, smoking, poor nutrition, delayed treatment, and ignoring cancer screening among older individuals. A few studies have shown that advancing age is linked to lower physiological stress tolerance, impaired endothelial function, and decreased organ reserves, all of which increase susceptibility to critical illness in older individuals [19–21].
However, the DIC-related mortality was higher in men than women, though both groups experienced an overall decline for one decade, followed by a sudden rise in the last few years [22]. The incidence of DIC in men showed a significant decrease over the past decade, whereas in women, the change was unremarkable [6]. The increased mortality in men is likely linked to a higher prevalence of serious conditions such as lung cancer and colorectal cancer [23, 24]. Moreover, cases of DIC have been observed in prostate cancer patients following fibrinolysis [25]. Higher cardiovascular disease burden, increased incidence of sepsis, chronic infections (e.g., pneumonia, urinary tract infections progressing to urosepsis), delayed healthcare-seeking behavior, cancer-related DIC, trauma, surgery, and poorer adherence to chronic disease management (e.g., hypertension, stroke, diabetes mellitus) may have led to more DIC-related AAMR in men [26].
This study further analyses racial disparities, with NH African Americans experiencing the highest mortality rates, followed by NH Asian or Pacific islanders, Hispanics, and the lowest in the White population. These disparities suggest ongoing inequities in healthcare access and quality, which were further exacerbated by the COVID-19 pandemic. The sharp early decline among Asians/Pacific Islanders could be due to improved access to care or genetic predispositions that influenced survival rates. Studies have shown that African American and Native American patients with DIC have a higher risk of in-hospital mortality compared to Caucasian patients. Additionally, research indicates that Hispanic patients may experience a higher incidence of thromboembolic events, which are related to DIC, compared to non-Hispanic White patients. These disparities may be influenced by genetic factors, access to healthcare, underlying health conditions, and socioeconomic determinants [1, 27].
Geographic variations in AAMR highlight potential differences in healthcare access, socioeconomic status, and regional disease burden. The highest AAMR in the Southern region may be linked to higher rates of chronic conditions predisposing individuals to DIC. This was followed by the Northeastern, Western, and Midwestern regions. Investigating factors such as healthcare disparities, comorbid conditions, and regional healthcare policies will be crucial. Future research should focus on the underlying causes of the increase after 2015 and explore targeted interventions to reduce racial and geographic disparities.
Metropolitan areas had higher DIC-related mortality rates compared to non-metropolitan regions, though both showed a decline in AAMR over the study. Urban hospitals, particularly major tertiary care centers, treat more critically ill patients, increasing exposure to sepsis. In urban areas, hospitals provide advanced cancer treatments and manage serious trauma cases resulting from accidents and violence. This may be reflected in a greater number of chemotherapy-related and significant tissue injury-related DIC cases. Persistent exposure to pollution may cause chronic endothelial dysfunction, slightly increasing coagulation risks. During the COVID-19 pandemic, higher patient volumes and ICU admissions in urban centers might have contributed to more cases of DIC-like coagulopathy. Additionally, crowded city environments may lead to higher rates of respiratory and bacterial infections. These combined factors may elevate the risk of developing DIC in metropolitan settings, while in rural areas, limited specialized care could lead to higher cancer-related DIC. Chronic conditions such as diabetes and hypertension, being more prevalent in rural areas, may elevate inflammation and endothelial dysfunction, raising DIC risk. Delayed transport to advanced care centers worsens outcomes due to late critical interventions.
Among the different states, California had the maximum number of deaths, estimated to be as high as 4,632, followed by Texas and Florida. The lowest rates were seen in Alaska, Wyoming, and Vermont.
These findings underscore the critical need for heightened clinical awareness and tailored interventions to address the elevated mortality risks associated with DIC, particularly among specific demographic groups. Early detection and improved cancer and chemotherapy treatment and monitoring, use of novel biomarkers, staging systems, newer anticoagulants, and targeted therapies are needed. DIC is a complex condition that may require individualized treatment guided by advanced coagulation tests such as thromboelastography or thrombin generation tests [28]. Further research is needed to explore targeted therapies and better identify specific clotting abnormalities.
Despite providing valuable insights into DIC-related mortality trends among older adults, this study has several limitations that should be considered when interpreting the findings. The study is based on mortality data derived from death certificates, which may be subject to misclassification and reporting biases. The analysis does not include individual patient records, limiting the ability to assess underlying conditions, treatment interventions, or severity of illness. Factors such as comorbidities, access to healthcare, and quality of treatment could significantly impact mortality trends but were not taken into account in this study. The vast majority (93.1%) of DIC-related deaths occurred in medical facilities, with only a small percentage reported in nursing homes, hospice care, or at home. This suggests potential underreporting in non-hospital settings, where DIC may not have been formally diagnosed or documented as a cause of death. While the study highlights differences in mortality rates by race/ethnicity and geographic region, it does not account for disparities in healthcare access or socioeconomic status, or differences in medical practices across populations. To address these limitations, future studies should incorporate detailed patient-level clinical data, investigate socioeconomic and healthcare access factors, and examine the impact of risk factors and treatment outcomes for older adults affected by DIC.
In conclusion, according to this study, DIC-related age-adjusted mortality rates in older individuals showed a significant decrease between 1999 and 2020, despite a slight upward trend in recent years. While a decrease in AAMR was observed across sex, racial groups, and geographic regions, disparities still exist, with NH African Americans exhibiting the highest mortality burden. The southern region recorded the highest AAMR, and the fall was more pronounced in metropolitan areas than in non-metropolitan areas. The results highlight the necessity of focused interventions and surveillance to prevent a further rise in DIC-related mortality.