Introduction
Patients with acute coronary syndrome (ACS) represent a heterogeneous population. Sex and racial differences in patient presentation may affect treatment decisions and outcomes among patients presenting with ACS. Current literature suggests that women are at higher risk of long-term adverse events than their male counterparts after undergoing percutaneous coronary intervention (PCI) for ACS, which is not completely explained by more advanced age and a higher burden of comorbidity [1]. On the other hand, racial differences in patients undergoing PCI for ACS have largely focused on controlling for treatment quality and socioeconomic differences to explain the divergence in outcomes between groups [2]. However, disparities in medical risk factors, pathophysiologic adaptation, and biologic response to injury may also play a role in various sex and racial groups. For example, it is known that a significantly higher percentage of age-adjusted prevalence of hypertension exists in adult non-Hispanic blacks in the United States, compared to other races [3]. Hypertension is a risk factor for left ventricular hypertrophy (LVH), which is a major independent risk factor for cardiovascular mortality [4]. Nevertheless, the association of LVH and mortality has not been borne out in most studies of ACS patients undergoing PCI [5–8]. However, LVH is a heterogeneous classification and can be subdivided into concentric (CH) and eccentric hypertrophy (EH). Based on new literature, we hypothesized that LVH may be a clinical over-simplification and the true effect of various cardiac geometry on outcomes may be subdued [9]. Indeed, our group has reported that EH and not CH is a prognostic variable, independent of sex, in ACS patients undergoing PCI [10]. The long-term consequence of differences in baseline cardiac geometry (as a result of hypertension) in patients undergoing PCI for ACS is ill-defined.
The primary purpose of this study was to clarify whether there were differences among sexual and racial groups in echocardiographic findings reflecting cardiac geometry and adaptation in patients undergoing PCI for ACS and whether this could explain the difference in outcomes seen between these groups.
Material and methods
We performed an observational study of patients presenting to an urban, community hospital with ACS who underwent PCI and were discharged alive between September 23, 2011 and July 31, 2017. The follow-up period of the primary study was 1 year. Qualified patients were identified from an institutional registry that enrolled all patients undergoing PCI for mandatory reporting to the New York State Department of Health (NYSDOH) and is exempt from the need for patient consent if de-identification of data for reporting is maintained. We excluded PCI patients who did not have ACS, based on clinical presentation, elevation in cardiac enzymes (troponin I and/or CK-MB) or ST-segment changes prior to the procedure. Peak troponin I (ng/ml) obtained during the hospital stay was abstracted from medical records. A transthoracic echocardiogram was performed during the index hospitalization utilizing a protocol in line with the American Society of Echocardiography/Intersocietal Accreditation Commission, and it was interpreted by a board-certified cardiologist. The 2D measurements of left ventricular end diastolic diameter (LVEDd), intraventricular septal diameter (IVS), and posterior wall diameter (PWD) were taken from parasternal long axis views. LV mass index (LVMI) was calculated according to the Devereux equation normalized to body surface area [11]: LVMI (g/m2) = (0.8 × (1.04 × ((LVEDD + IVSd + PWd)3 – LVEDD3)) + 0.6)/body surface area.
Relative wall thickness (RWT) was calculated as: RWT = (2 × PWd)/LVEDd.
In accordance with American Society of Echocardiography (ASE) guidelines, an LVMI ≥ 95 for females and ≥ 115 g/m2 for males was suggestive of LVH, whereas a RWT ≥ 0.42 was suggestive of concentric adaptations [12]. Four phenotypes of cardiac geometry were identified: normal, concentric remodeling (grouped together as normal geometry), concentric hypertrophy (defined as LVMI ≥ 95 and RWT ≥ 0.42) and eccentric hypertrophy (defined as LVMI ≥ 95 and RWT ≥ 0.42). Left ventricular ejection fraction (LVEF) was measured using the 2D, bi-plane or single plane method of disks at the discretion of the interpreting cardiologist. The primary endpoint was all-cause mortality within 1 year after hospital discharge, which was verified by reviewing medical records or by contacting primary care physicians or the patients’ families, when necessary. The secondary endpoint was major adverse cardiac events (MACE-B) after discharge, which was defined as a composite of all-cause mortality, non-fatal myocardial infarction, non-fatal stroke, or hospitalization for bleeding, adjudicated based on the primary discharge diagnosis and verified in a similar fashion.
Statistical analysis
Continuous and categorical variables are presented as the mean with one standard deviation or median with interquartile range, as appropriate, and were compared with Student’s t-test for means, the Mann-Whitney test for medians, and the two-sided z-test or χ2 test for proportions. Event rates were estimated using the Kaplan-Meier time-to-event methodology and compared using log-rank tests. Multivariable Cox proportional hazard regression was used to determine the independent predictors of the primary and secondary outcomes. The following demographical covariates were simultaneously included in the model for the primary and secondary outcomes: age, sex, race (white vs. non-white), hypertension, diabetes, prior MI, pre-PCI creatinine, LVEF < 50%, normal geometry, concentric and eccentric hypertrophy. Two dummy variables were used to include the three groups of cardiac geometries simultaneously with reported hazard ratios (HR) of CH and EH in reference to a HR of 1 for normal geometry. The significance level was set at p < 0.05 (two-sided). All analyses were performed with IBM SPSS Statistics for Mac, version 24 (IBM Corp., Armonk, N.Y., USA). Figures were generated with Microsoft Excel for Mac, version 16.45 (Microsoft Corp., Redmond, WA, USA).
Results
Between September 2011 and July 2017, 1,610 ACS patients were identified in the institutional registry who underwent PCI. Vital status could not be established in 165 patients. A complete echocardiographic report was not available for 292 patients. A total of 1,153 patients were enrolled in the study. Baseline characteristics, by sex and race, are displayed in Table I. In summary, males tended to be younger, have fewer comorbidities, larger cardiac LV chamber diameter/thickness, more hypertrophic changes, lower LVEF, higher peak troponin values, and were more likely to present with ST-elevation myocardial infarction (STEMI). Whites tended to have fewer comorbidities, smaller cardiac LV chamber diameter/thickness, less hypertrophic changes, higher LVEF, and higher peak troponin values.
Table I
Comparative table of baseline demographics by sex and race
[i] CABG – coronary artery bypass graft, CVD – cerebral vascular disease, FamHx of CAD – family history of coronary artery disease HF – heart failure, IVS – intraventricular septal diameter, MI – myocardial infarction, LVIDd – left ventricular inner diameter at end diastole, LVEF – left ventricular ejection fraction, LVMI – left ventricular mass index, PAD – peripheral artery disease, PCI – percutaneous coronary intervention, PWD – posterior wall diameter, RWT – relative wall thickness, STEMI – ST-segment elevation myocardial infarction, sx – surgery.
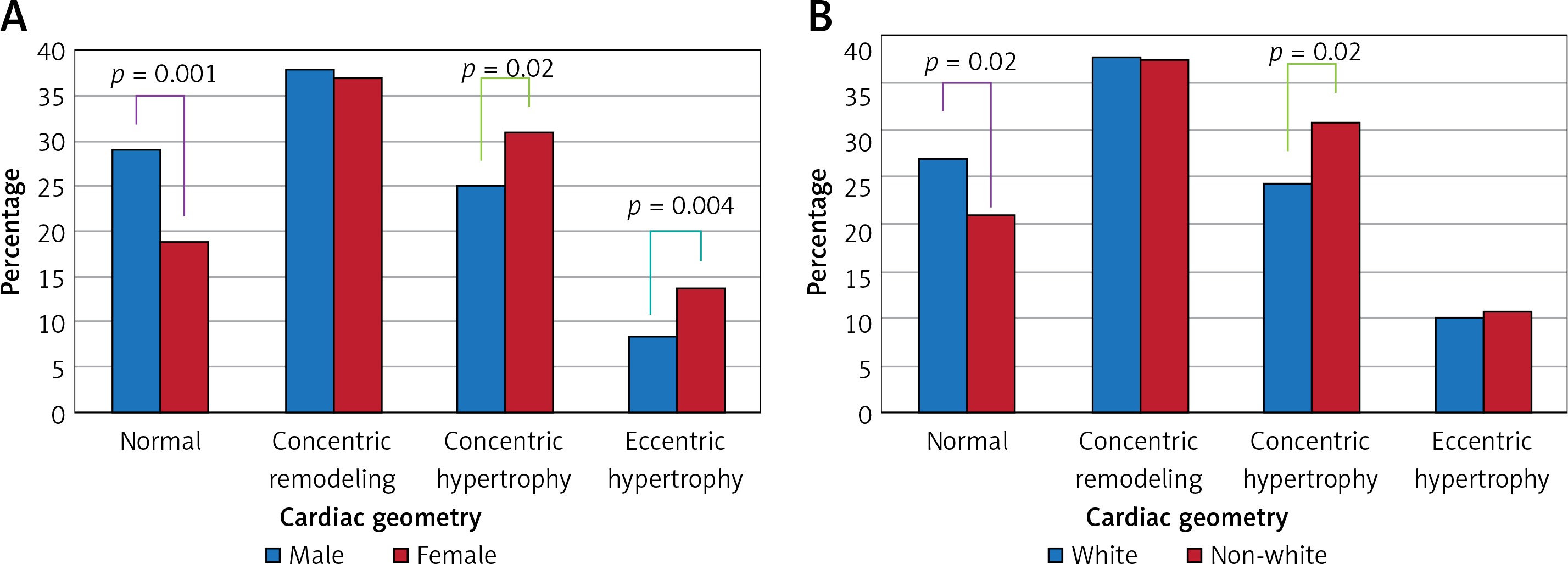
Analysis comparing cardiac geometric patterns between males and females revealed a statistically significant difference in the distribution of three phenotypes: normal, concentric hypertrophy, and eccentric hypertrophy: 29% vs. 19% (p = 0.001), 25% vs. 31% (p = 0.02), and 8% vs. 14% (p = 0.004), respectively. The prevalence of concentric remodeling was similar (38% vs. 37%, p = 0.64) (Figure 1 A). Analysis by race revealed that whites were more likely to present with normal cardiac geometry (27% vs. 21%, p = 0.02) and less likely to present with concentric hypertrophy (24% vs. 31%, p = 0.02) than non-whites. Again, the rates of concentric remodeling were similar among the racial groups (38% vs. 38%, respectively, p = 0.93) (Figure 1 B).
Females were at increased risk of one-year mortality and MACE-B compared to males. There were no differences in outcomes among the different race groups (Table II). Incidence of various MACE-B endpoints are displayed in Table III.
Table II
Univariate analysis of 1-year mortality and MACE-B according to sex and race
Table III
Incidence of various major adverse cardiac events and bleeding endpoints by sex
| Parameter | Male (n = 694) | Female (n = 459) | P-value |
|---|---|---|---|
| All-cause death | 42 (6) | 48 (10) | 0.01 |
| Non-fatal MI | 31 (4) | 34 (7) | 0.02 |
| Non-fatal stroke | 2 (0.2) | 6 (1) | 0.06 |
| Hospitalization for bleeding | 28 (4) | 21 (5) | 0.41 |
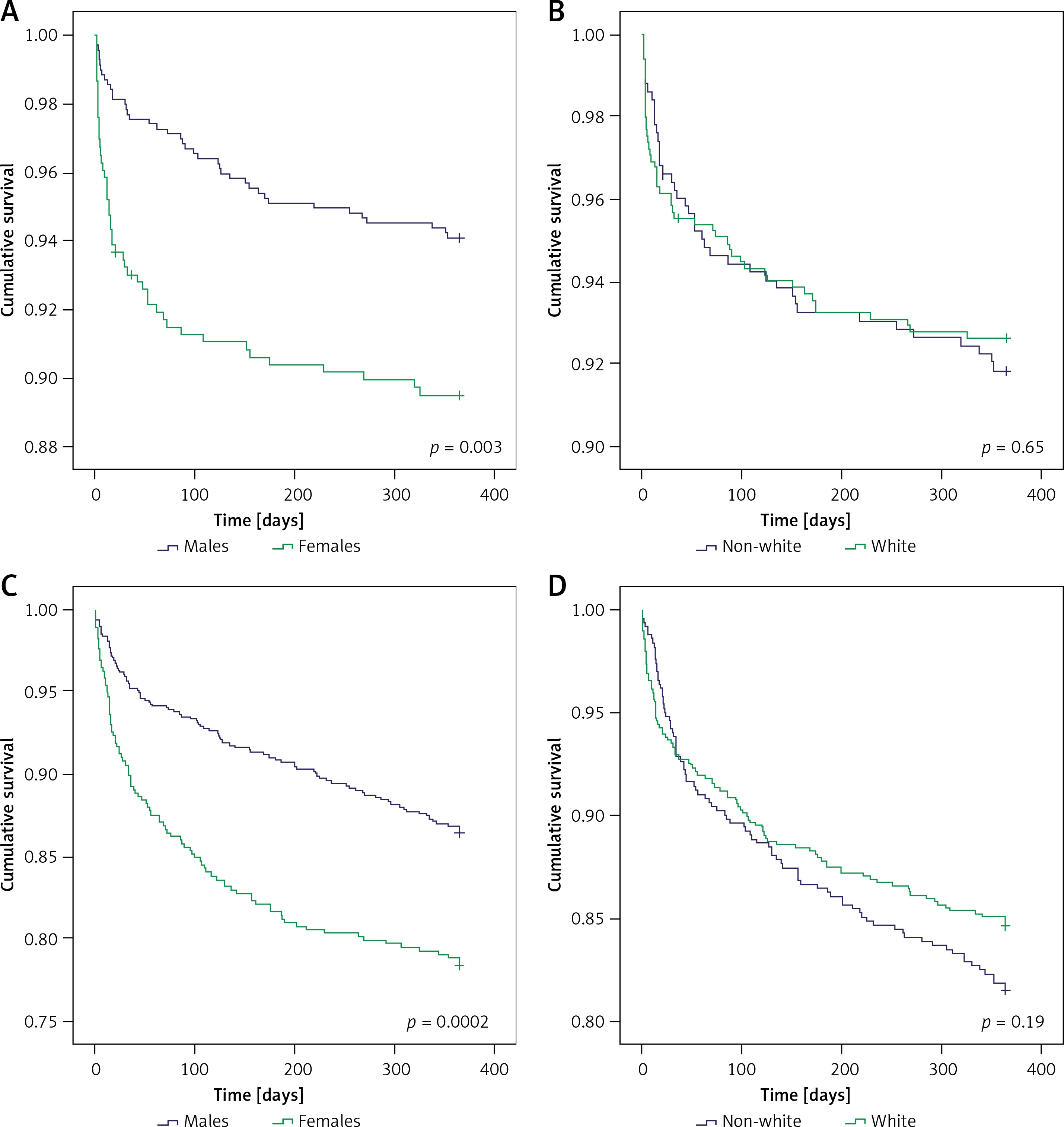
The primary endpoint of all-cause death (n = 89, 7.7%) occurred in 48 (10.5%) females and in 41 (6.0%) males and 48 (7.4%) whites and 41 (8.2%) non-whites, p = 0.003 and 0.65, respectively (Figures 2 A, B).
Figure 2
A – All-cause mortality by sex. B – All-cause mortality by race. C – Major adverse cardiac events by sex. D – Major adverse cardiac events by race
In a multivariable analysis, age (hazard ratio (HR (per year) = 1.07 (1.05–1.09), p < 0.001), pre-PCI creatinine (HR (per 1 mg/dl) = 1.11 (1.01–1.22), p = 0.023), and LVEF < 50% (HR = 2.69 (1.68–4.30), p < 0.001) were significant predictors of survival, whereas race, sex, hypertension, diabetes, prior MI, and cardiac geometry were not (Table IV).
Table IV
Independent predictors of 1-year all-cause mortality and major adverse clinical events
[i] LVEF – left ventricular ejection fraction, LVH – left ventricular hypertrophy; defined as LVMI > 115 in males, and ≥ 95 in females, MACE – major adverse cardiac events; defined as cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, and hospitalization for bleeding, MI – myocardial infarction.
Males with EH had similar MACE-B outcomes as females with EH 1 year after PCI (29% vs. 32%, respectively, p = 0.77) (Table V).
Table V
Univariate comparison of 1-year mortality and MACE-B in EH group between sexes
| Parameter | Mortality at 1 year | P-value | MACE-B at 1 year | P-value |
|---|---|---|---|---|
| Sex: | 0.41 | 0.77 | ||
| Males with EH (n = 58) | 7 (12) | 17 (29) | ||
| Females with EH (n = 63) | 11 (17) | 20 (32) |
Age (HR (per year = 1.04 (1.02–1.05), p < 0.001), female sex (HR = 1.38 (1.01–1.87), p = 0.04), diabetes (HR = 1.43 (1.05–1.95), p = 0.02), pre-PCI creatinine (HR per 1 mg/dl) = 1.10 (1.03–1.17), p = 0.003), LVEF < 50% (HR = 1.74 (1.28–2.36), p < 0.001), and eccentric hypertrophy (HR = 1.54 (1.02–2.33), p = 0.04) were significant predictors of MACE-B, whereas race, hypertension, prior MI, and concentric cardiac geometry were not (Table IV).
Discussion
The major findings from this single-institution, observational study, in which 2D echocardiographic data from 1,153 patients with an index ACS treated with PCI were compared by sex and race are as follows: 1) sexual differences in the distribution of EH place females in a higher risk category, whereas racial differences differ only in CH; 2) females and males exhibit similar outcome rates once EH develops; 3) CH is a benign adaptation in one-year outcomes in ACS patients undergoing PCI and as such racial outcomes did not differ between groups; 4) differences in cardiac geometry did not account for the difference in outcomes seen between sexes.
The premise that sex affects outcome in patients undergoing PCI for symptomatic CAD has been extensively studied and debated, with mixed results [7–20]. However, the conflicting findings can largely be attributed to differences in study design and group selection. The studies that found no difference in long-term mortality between men and women enrolled a sizeable proportion of patients treated for stable angina or atypical chest pain [20–26]. In contrast, an increase in long-term mortality or MACE-B risk was found in those studies that included only patients treated for ACS [13–19]. Yet, a fair degree of heterogeneity exists even in those studies focusing on ACS patients. For example, sub-group analyses by Raphael et al. revealed that the higher mortality seen in women is due to death from non-cardiac causes, explained by higher baseline age and comorbidities [13]. More recently, Kosmidou et al. reported only a statistically significant increased risk of MACE-B at 5 years in females, while the increased risk for all-cause mortality disappeared upon adjustment for baseline and procedural characteristics [17]. We report findings in agreement of females being at increased risk of adverse outcomes following hospital discharge after PCI for ACS.
Our findings are novel because we recently integrated a new clinical variable – cardiac geometry – that may be useful in risk stratifying patients with respect to death or MACE-B [10]. We now investigate the interaction between it and race and sex to assess whether differing cardiac geometry may be more prevalent among certain race or sex groups. As hypertension is more common in females and in non-Hispanic blacks, they are more likely to exhibit hypertrophic cardiac geometries, both concentric and eccentric [27]. Although racial differences in 1-year mortality or MACE-B were not observed, such divergence in time-to-event curves may occur beyond 1 year given the increased prevalence of hypertrophic changes in non-white populations in our cohort and the fact that LVH is an independent predictor of mortality [28]. In our study, CH was not independently associated with worse outcomes in 1 year; thus the lack of racial differences in outcomes is not surprising. It was found that females tend to have higher frequencies of EH than males, which highlights novel sex differences in cardiac geometry portending higher risk. In agreement with prior studies, sex differences in MACE-B were observed in our analysis even after controlling for age and baseline co-morbidities. However, our analysis did not reveal EH to interact with sex in observed MACE-B events 1 year after PCI, indicating cardiac geometry independent mechanisms in sex and MACE-B.
It is currently not known whether disparities in medical risk factors, pathophysiologic adaptation, and/or biologic response to injury are responsible for the sexual differences in worse outcomes seen in ACS patients undergoing PCI. Our analysis and others have demonstrated that sex is predictive of worse outcomes independent of medical risk factors. Based on the results of this study, it seems unlikely that sex differences in biologic response to LVH and acute MI in those with EH contribute to worse outcomes. Moreover, the results from this study do not support the notion that the increased prevalence of EH in females presenting with ACS may account for the differences in outcomes reported in the literature, since the difference in MACE-B between sexes persisted in subgroup analysis without EH (unpublished data). An important question for future studies may be to explain why females presenting with ACS have a higher prevalence of EH and whether this may be a predictive variable.
We recognize important limitations to our study design, observations and conclusions. The first is the relatively small cohort of patients included in this single-center study when compared to multi-centered randomized clinical trials, which may not be generalizable to the US population as a whole. Second, data were collected retrospectively from the electronic medical records, and were not recorded in a standardized and systematic manner, thus obscuring confounders that cannot be optimally controlled for. A strength of our study is the relatively high percentage of females and minority groups enrolled in our institutional registry.
In conclusion, despite these limitations, we conclude that in patients with recent acute coronary syndrome revascularized with percutaneous coronary intervention, 2D echocardiography identifies females at higher risk for worse outcomes partly because they are more likely to express the eccentric hypertrophy phenotype, which is an independent predictor of worse outcomes. However, our analysis did not reveal EH to interact with sex in observed adverse events 1 year after PCI, indicating mechanisms independent of cardiac geometry in sex and adverse outcomes. Further studies are needed to explore the variables responsible for the increased prevalence of EH in female ACS patients.