Introduction
The use of bare metal and drug-eluting stents to recanalize narrowed coronary arteries and endovascular vessels revolutionized revascularization. However, the demonstrated efficacy of bare-metal stent (BMS) and drug-eluting stent (DES) is balanced by the risk of stent thrombosis, thought to be due to delayed vascular healing resulting from either the initial antiproliferative effect (and associated late acquired incomplete stent apposition) or a hypersensitivity reaction to the drug, polymer coating, or their combination [1, 2]. In-stent restenosis (ISR) occurs in up to one-half of patients treated with BMS [3]. Although it was initially considered to be a benign process, later on the evidence showed that it presented with acute myocardial infarction or unstable angina in more than one-third of cases [4]. Several treatment modalities have been proposed and used for bare-metal in-stent restenosis: plain/cutting balloon angioplasty (BA), repeat stenting, vascular brachytherapy, rotational directional atherectomy, pullback atherectomy, and excimer laser-based angioplasty [5]. Previously plain BA with or without brachytherapy had been the most frequently used treatment for patients with in-stent restenosis, but now a number of studies have shown superiority of DES over conventional treatment modalities for restenosis in BMS in terms of a larger post-procedural lumen volume as well as a significant reduction in the volume of neointimal proliferation with DES than with plain BA at follow-up angiography [6–11]. The DES limitations including uneven distribution of drug, delayed endothelialization, and polymer-induced inflammation or thrombosis prompted innovation for improved solutions, such as the local delivery of drugs. Reliable clinical experience, however, is still limited. The Treatment of In-Stent Restenosis by Paclitaxel-Coated Balloon Catheters (PACCOCATH) ISR I trial was a controlled, randomized, blinded first-in-human study that investigated the use of paclitaxel-coated balloon catheters for treatment of coronary in-stent restenosis. Patients who were treated with the coated PACCOCATH balloon had significantly superior angiographic results associated with improved 12-month clinical outcomes compared with patients treated with an uncoated balloon [12]. The results of this trial were confirmed by longer follow-up and the subsequent PACCOCATH ISR II trial [13]. From a technical point of view, the ease of use and high deliverability of balloon-based drug delivery systems create an opportunity for their use in coronary territories in which DES can be problematic or have not proved to be particularly effective such as small vessels, bifurcations, long lesions, ostial lesions, and saphenous vein grafts. In this study we compared the efficacy of drug-eluting balloons versus drug-eluting stents in the treatment of in-stent restenosis.
The aim of the study was to compare the efficacy of drug-eluting balloons versus drug-eluting stents in the treatment of ISR in terms of binary restenosis, target lesion revascularization (TLR) and late lumen loss (LLL) by coronary angiography at 6 months.
Material and methods
The study was conducted at a tertiary care hospital from April 2016 to May 2017. Patients were selected from those having undergone angioplasty and attending the cardiac outpatient department for recurrence of angina equivalent symptoms. Patients aged > 18 years, with clinical evidence of stable or unstable angina or abnormal functional study and restenosis in a single stent were included in the study. The patients were screened after assessment of ISR through qualitative coronary angiography (QCA).
All patients with acute myocardial infarction within the previous 48 h, severe renal insufficiency (GFR < 30 ml/min), known hypersensitivity or contraindication to the required medication, or malignancies causing life expectancy of < 2 years were excluded. Also, on the basis of angiographic findings, patients with stented segments > 34 mm in length, vessel diameters of < 2.5 mm, unprotected left main stenosis, and stents covering a major side branch (> 2 mm) were excluded from the study.
A total of 41 patients, who attended the cardiology department, fulfilled the inclusion and exclusion criteria and were enrolled in the study. The patients were then randomized to the two arms of the study wherein the control group was treated with the implantation of a second-generation DES and the study group was treated with a paclitaxel-eluting DEB. The study was designed as a prospective randomized single-blind study, and the patients were blinded to the treatment assignment during the study. Procedural success was assessed by the performance characteristics in terms of tracking ability, deliverability and acute luminal gain on QCA. Late lumen loss and any ISR (the difference between the in-segment minimal lumen diameter (MLD) after the procedure and at 6 months, as evaluated by quantitative coronary angiography) was the primary end point. Secondary end points included the rate of restenosis and the rate of the combined clinical events up to 6 months, including stent thrombosis, target-lesion revascularization, myocardial infarction, and death (Tables I–III).
Table I
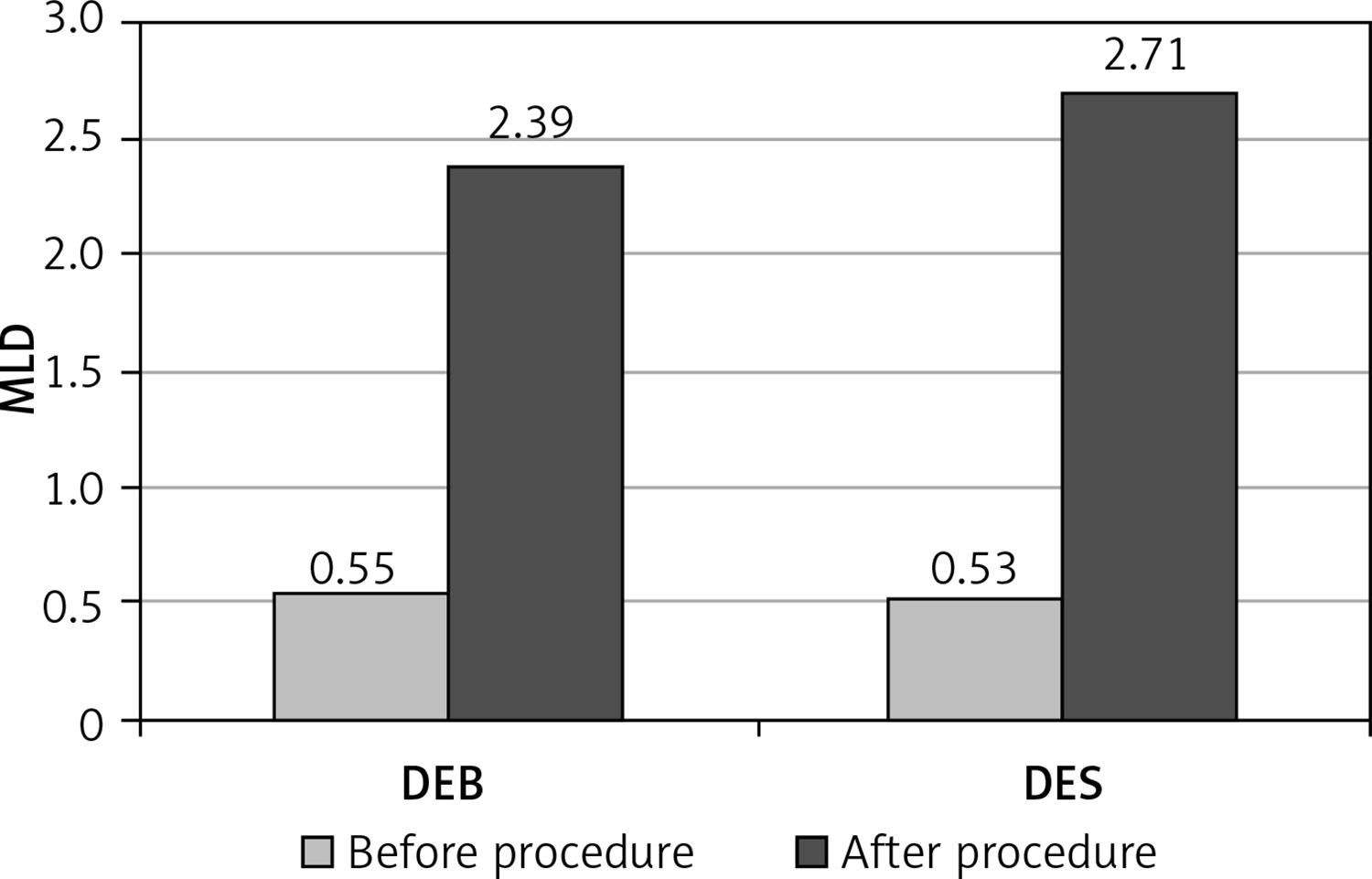
Angiographic data before and after procedure (mean ± SD)
Table II
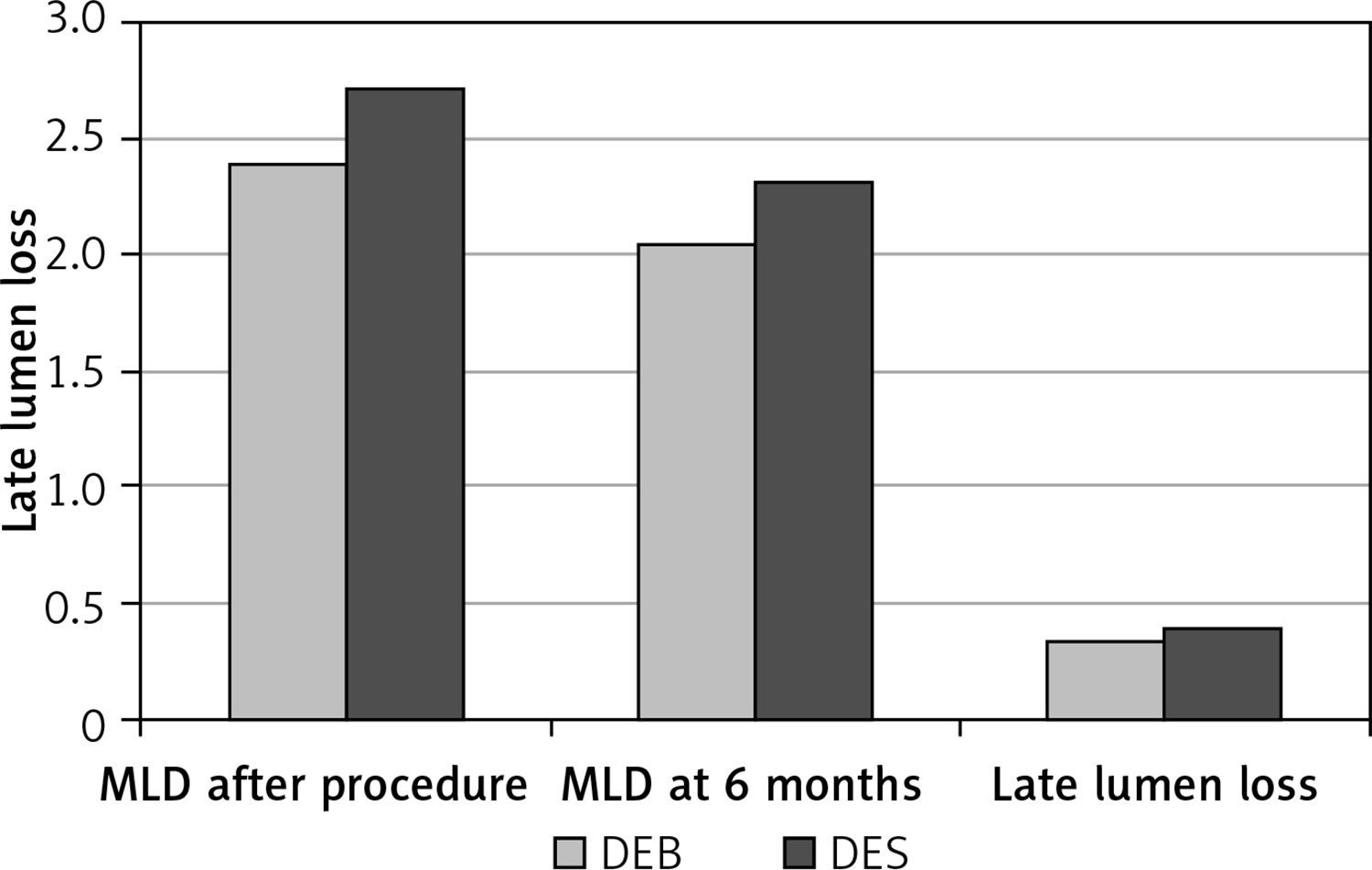
Coronary angiography follow-up results at 6 months in 2 study groups (mean ± SD)
| Parameter | DEB | DES | P-value |
|---|---|---|---|
| MLD after procedure | 2.39 ±0.42 | 2.71 ±0.31 | < 0.009* |
| MLD at 6 months | 2.05 ±0.56 | 2.31 ±0.54 | 0.132 |
| Late lumen loss | 0.35 ±0.52 | 0.40 ±0.36 | 0.719 |
Table III
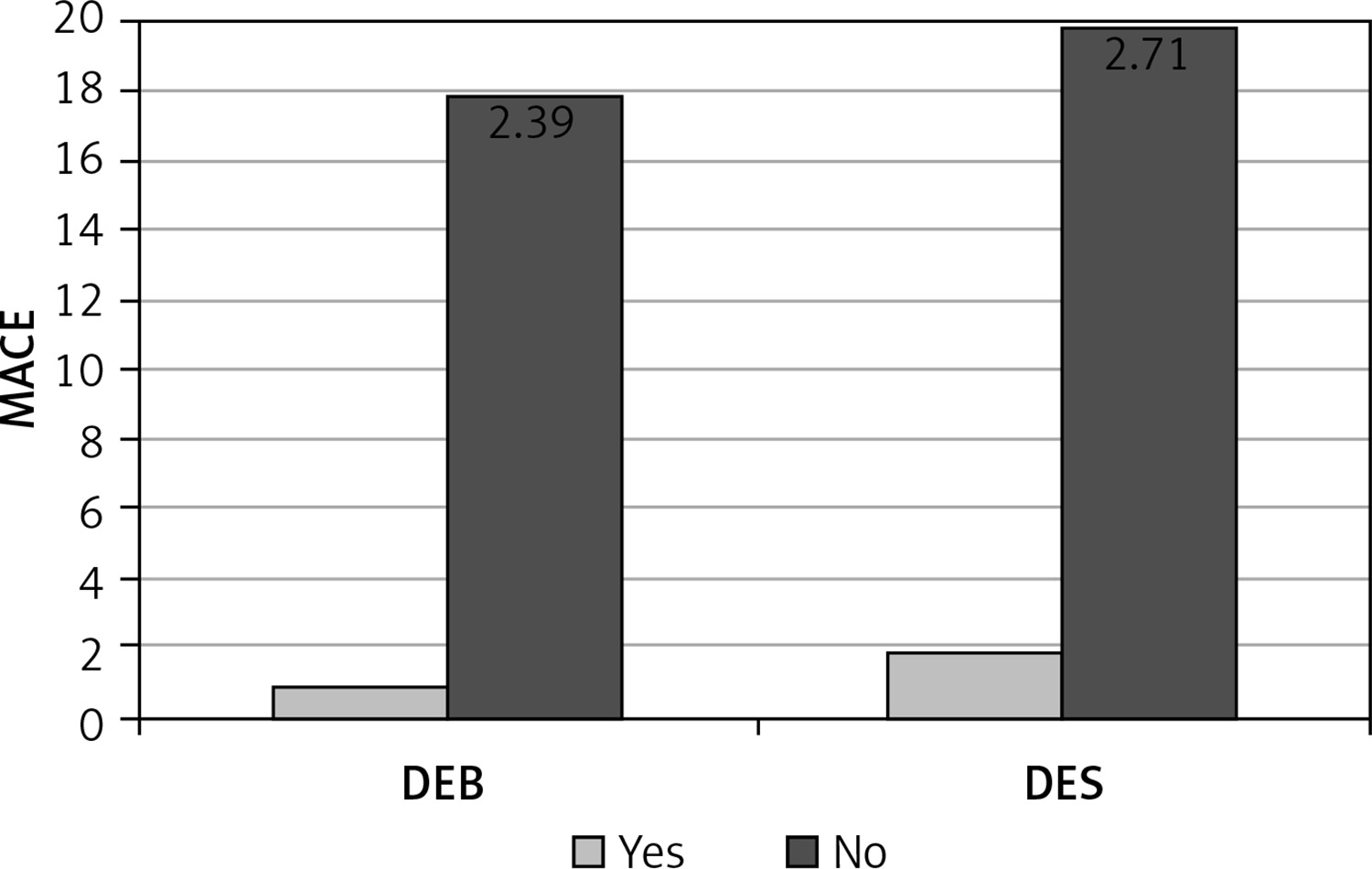
Incidence of major adverse cardiovascular events (MACE) in 2 groups
| MACE | Treatment of in-stent restenosis (ISR) | Total | Pearson χ2 | P-value | |
|---|---|---|---|---|---|
| DEB | DES | ||||
| Yes | 1 | 2 | 3 | 0.54 | 0.46 |
| No | 18 | 20 | 38 | ||
| Total | 19 | 22 | 41 | ||
Written informed consent was obtained from all patients before randomization. Ethical clearance was taken from the hospital ethics committee.
Statistical analysis
Continuous variables were expressed as mean ± SD. Values were reported as numbers with relative percentage or SD. For continuous data, groups were compared with the parametric Student’s t test or the nonparametric Mann-Whitney U test according to the distribution of the data. Categorical variables were compared with the χ2 test. A p-value of < 0.05 was considered statistically significant. The SPSS statistical software (version 17.0, SPSS, Inc., Chicago, Illinois) was used for all statistical calculations.
Results
Observation
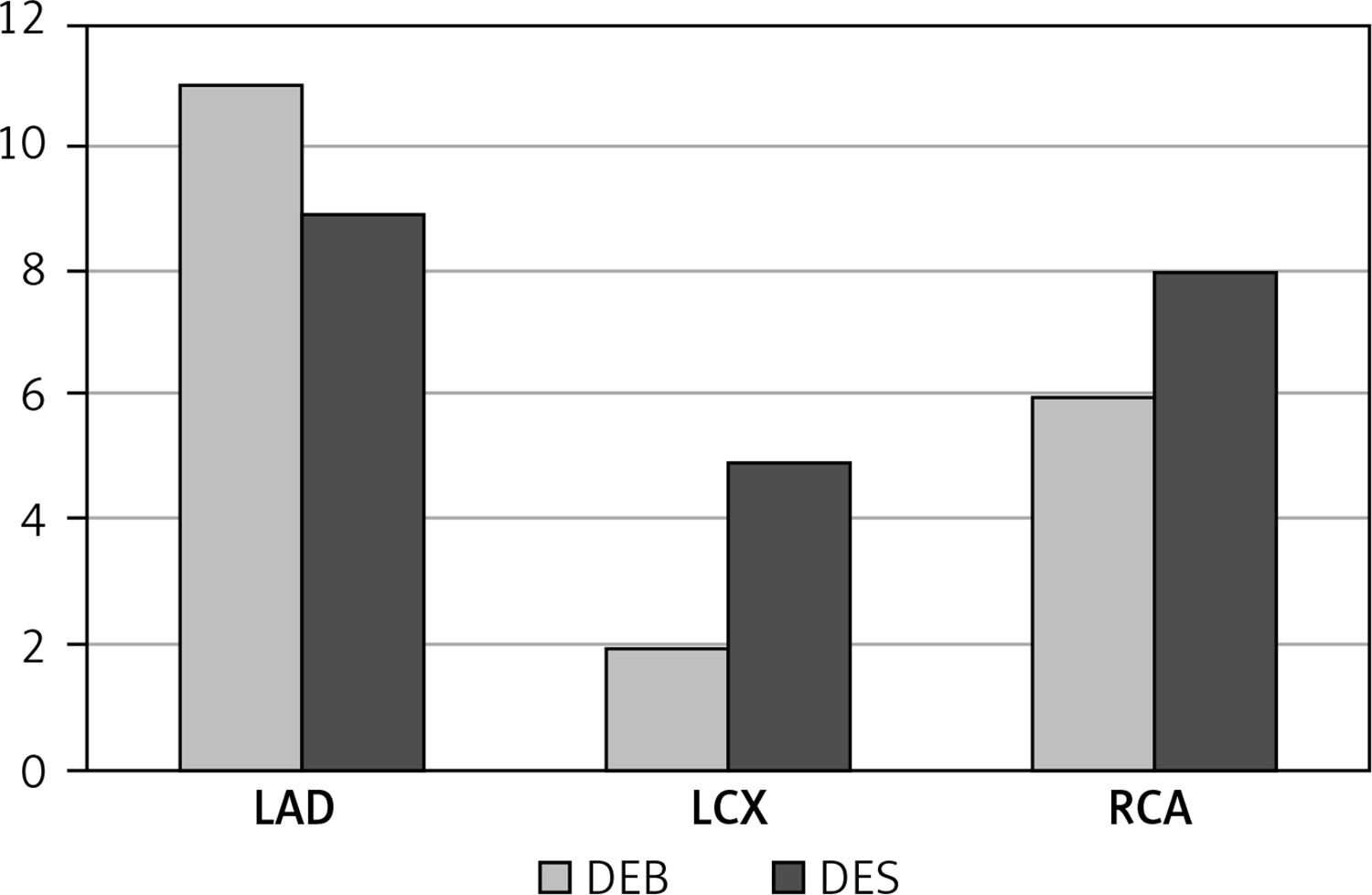
Out of 41 patients, 29 (60.9%) patients were between the ages of 50 and 70 years; 33 were male and 8 were female. Nineteen patients were assigned revascularization with a DEB and 22 with a DES (Figure 1). The mean age of patients in the DEB group was 57.16 ±11.16 years while that in the DES group was 60.95 ±8.33 years. Thirteen patients were male and 6 were female in the DEB group and 20 were male and 2 were female in the DES group. The mean body mass index (BMI) in the DEB group was 27.05 ±3.62 kg/m² while in the DES group it was 25.29 ±3.11 kg/m². Three patients in the DEB group and 4 in the DES group had type2 diabetes mellitus. The left anterior descending artery (LAD) was previously stented in 20 patients, out of whom 11 were treated with DEB and 9 with DES. Out of 7 patients with left circumflex artery (LCX) ISR, 2 were treated with DEB and 5 with DES. In 14 patients, the right coronary artery (RCA) was affected; of these, 6 received a DEB and 8 a DES (Figure 2).
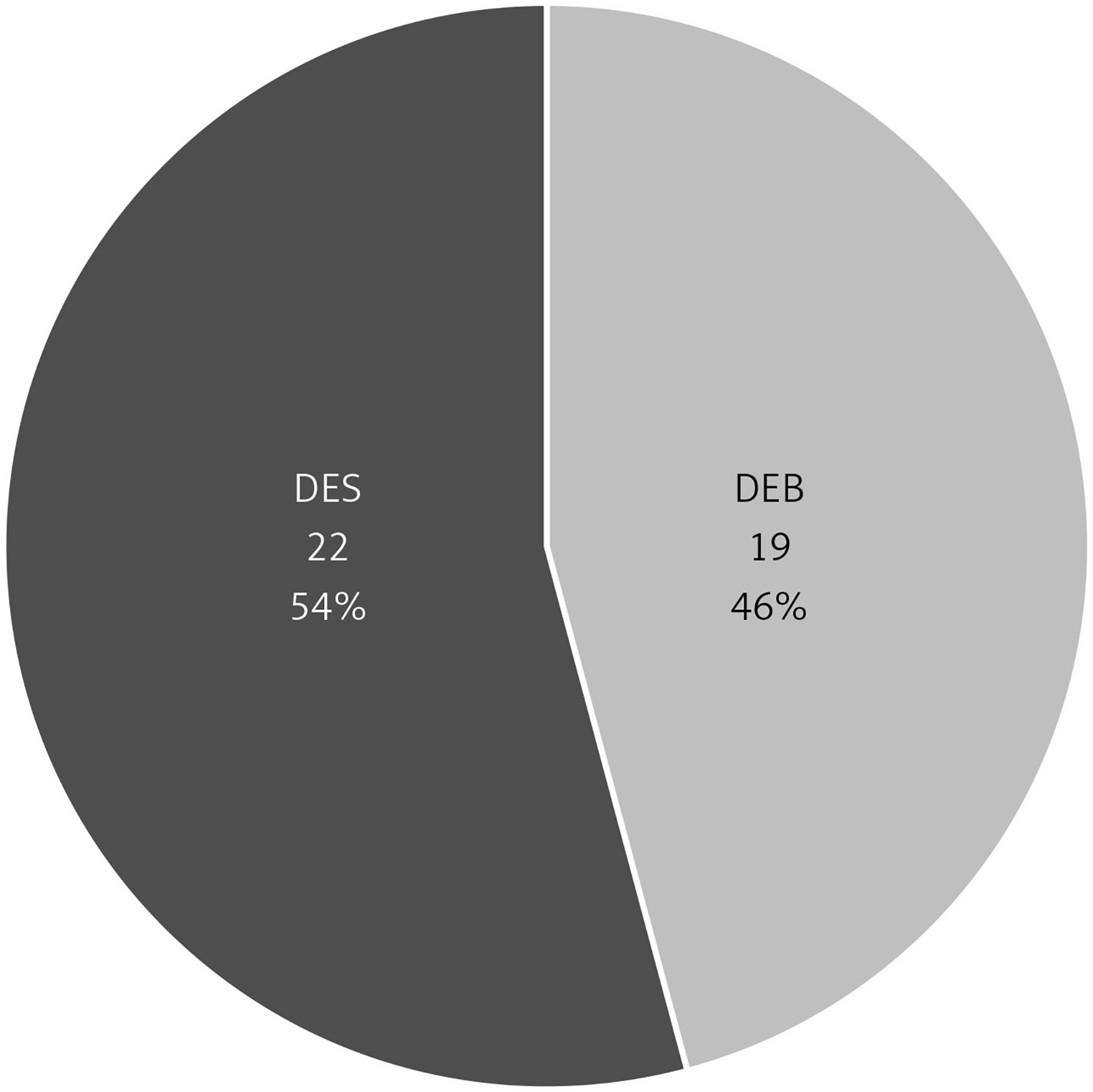
Figure 2
In-stent restenosis (ISR)-affected coronary artery
LAD – left anterior descending artery, LCX – left circumflex artery, RCA – right coronary artery.
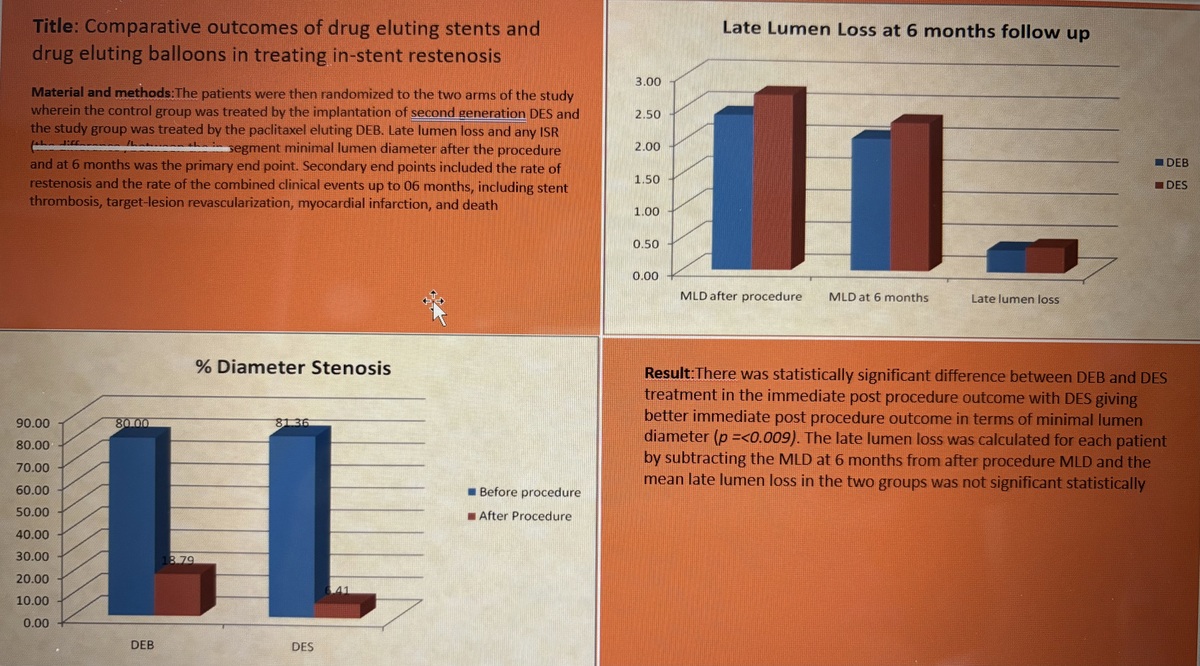
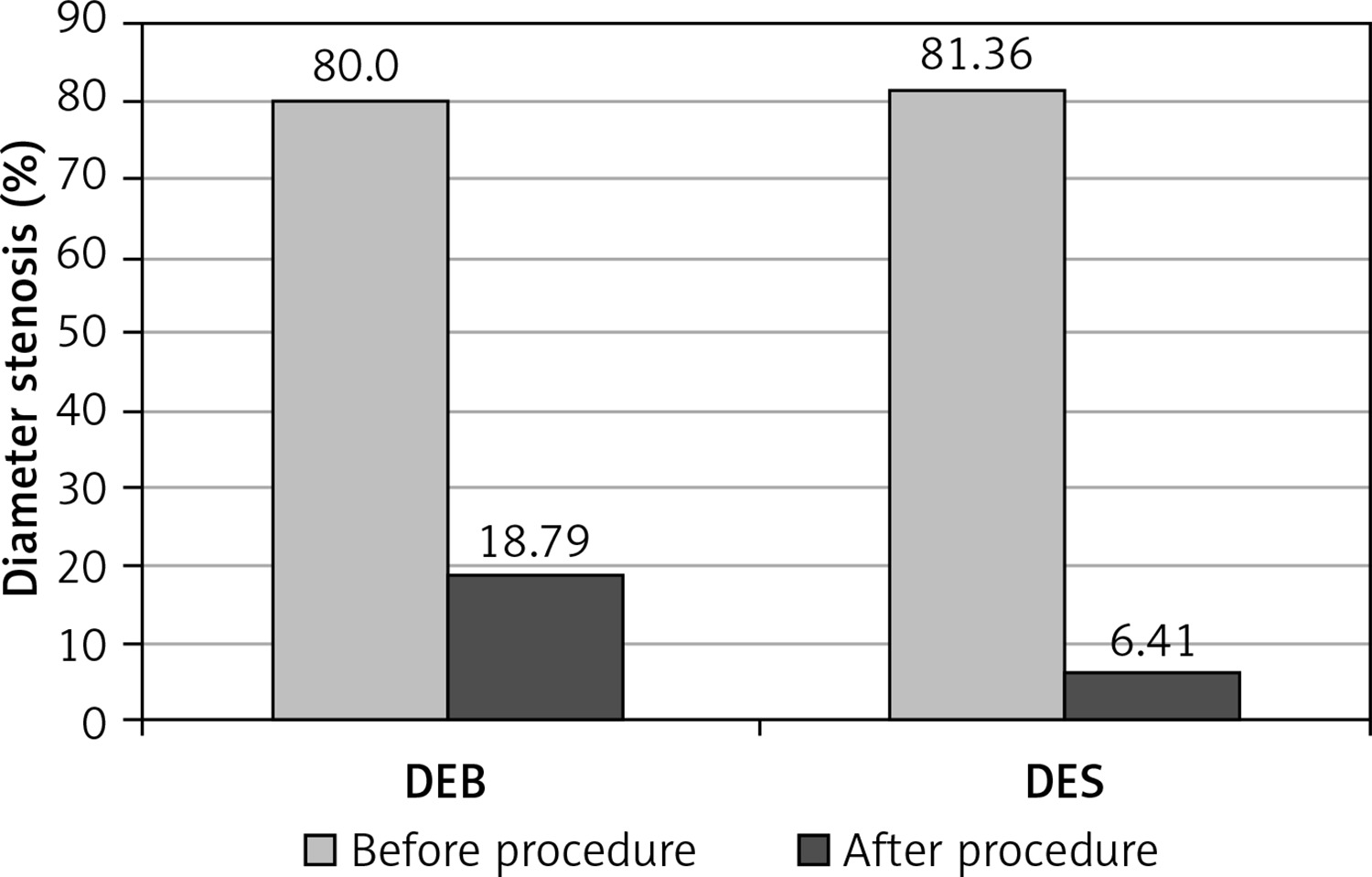
The mean stenosis diameter in the ISR coronaries treated with DEB was 80.00 ±13.33% with an MLD of 0.55 ±0.38 mm before the procedure (Figure 3). The maximum ISR of 100% was observed in 4 patients. After treatment with DEB, the % diameter stenosis decreased to 18.79 ±5.30 and MLD increased to 2.39 ±0.42 mm. The mean stenosis diameter in the ISR coronaries treated with DES was 81.36 ±10.82% with an MLD of 0.53 ±0.27 mm before the procedure (Figure 4). The maximum ISR of 100% was observed in 2 patients. After treatment with DES, the % diameter decreased to 6.41 ±2.09 and MLD increased to 2.71 ±0.31 mm. There was a statistically significant difference between DEB and DES treatment in the immediate post-procedure outcome, with DES giving a better immediate post-procedure outcome. The late lumen loss was calculated by subtracting the MLD at 6 months follow-up from that after the procedure. No significant difference in late lumen loss was observed between patients treated with either DEB or DES (Figure 5). Two patients who were treated with a DEB developed significant ISR (> 50%), and they had to be undergo revascularization, whereas among the patients who were treated with a DES, only 1 developed significant restenosis requiring revascularization (Figure 6).
Discussion
There was a statistically significant difference between DEB and DES treatment in the immediate post-procedure outcome, with DES giving a better immediate post-procedure outcome in terms of MLD (p ≤ 0.009). The late lumen loss was calculated for each patient by subtracting the MLD at 6 months from the post-procedure MLD, and the mean late lumen loss in the two groups was not significantly different.
This study demonstrated that treatment of ISR using DEB is a feasible and effective approach and provides excellent results, with only 5.3% TLR at 6 months. The drug-eluting balloon has the added advantage of simplifying the treatment of ISR while at the same time avoiding the addition of a second layer of metal and reducing costs.
However, our study sample size is small, and the follow-up was only 06 months; hence studies with a larger sample size and longer follow-up are recommended.
Since DEB are found to be effective or at least non-inferior at 6 months in our small study, we also propose further research on using DEB for smaller vessels, longer length restenotic segments and in ISR in stents placed across major side branches to avoid placing another layer of metal, which may compromise flow to the major side branch.