
Introduction
Cardiovascular diseases (CVD) are the biggest contributors to worldwide mortality. Over the last three decades, CVD cases have doubled, affecting over 523 million people globally in 2019 alone [1]. Currently, 6.5 million people in the US suffer from heart failure (HF), projected to rise to 8 million by 2030 [2]. HF patients alone, on account of medications, missed work days, and extensive use of health care services, account for an annual cost of 30.7 billion US dollars [3]. Although HF is extensively researched in older adults, the increase in various risk factors such as obesity, smoking, physical inactivity, and poor diet among younger adults suggests a paradigm shift towards greater mortality even in the younger population in the foreseeable future [4, 5].
Studies have demonstrated that the distribution of HF mortality is not only based on risk factors such as diabetes and hypertension, but has also shown various demographic and geographical differences [3, 6]. Although mortality in older adults has been previously described, evaluating HF-related mortality over larger population groups can enable physicians to observe changes in mortality trends across multiple age groups over the last two decades and to focus on early lifestyle changes to reduce CVD morbidity down the line, thereby decreasing the disease burden [7].
To achieve this aim, this study assessed the distribution of HF-related mortality over a wide population (ages 15 and above), to evaluate changes in mortality from 1999 to 2020 in the United States.
Material and methods
Study setting and data source
Using information from the CDC WONDER (Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research) database covering the years 1999 to 2020, the study observed the mortality records of individuals with heart failure (HF). The information was obtained by utilizing the ICD I50.x code for HF-related mortality (International Statistical Classification of Diseases and Related Health Problems, 10th revision), which includes deaths ascribed to congestive heart failure, left ventricular failure, and unexplained heart failure. Records for underlying causes of death were accessed to study HF-related deaths with a population age group defined as ≥ 15 at the time of their death. This investigation did not require any ethical approval from the Ethical Review Committee or other local institutional board as the data utilized from the CDC WONDER database were completely deidentified and government-issued and were available publicly. The study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting criteria.
Data extraction
Data on population size, year of occurrence, place of death, demographic characteristics, classification of urban and rural areas, allocation to regions, and individual states were all obtained. The cause of mortality was ascertained from death certificates [8]. Among the demographic factors assessed were race/ethnicity, gender, age, and the manner of death (outpatient, emergency room, inpatient, death upon arrival, or status unknown). Non-Hispanic White, non-Hispanic Black or African American, Hispanic or Latino, non-Hispanic American Indian or Alaskan Native, and non-Hispanic Asian or Pacific Islander were among the racial/ethnic groupings. Ten-year increments were used to divide the age groups (i.e., 15–24, 25–35 and so on until over 85). Based on the 2013 U.S. census, the National Center for Health Statistics’ Urban-Rural Classification Scheme was used to divide the population into three groups: urban counties (population ≥ 1 million), medium/small metropolitan areas (population 50,000–999,999), and rural counties (population < 50,000). Regional distribution was broken down into the Northeast, Midwest, South, and West based on U.S. Census Bureau criteria. From 1999 to 2020, age-adjusted mortality rates (AAMRs) per 100,000 and crude mortality rates (CMR) with 95% confidence intervals were obtained. Using the CDC WONDER database, a map of the state-by-state AAMR distribution was produced.
Data analysis
The extracted data were imported into Excel 2019 for additional analysis using the Joinpoint regression tool (National Cancer Institute, joinpoint V 5.0.2). Using log-linear regression models, trends were identified. The average annual percentage change (AAPC), which represents the overall change from 1999 to 2020, was calculated based on the slope of the line, which indicated the annual percentage change (APC). APC values were represented by positive or negative numbers according to the slope gradient, which demonstrated trends in mortality rates that were either rising or falling. A 2-tailed t-test was used to determine whether changes in APCs were significantly different from zero, with a value of p < 0.05 being deemed statistically significant.
Results
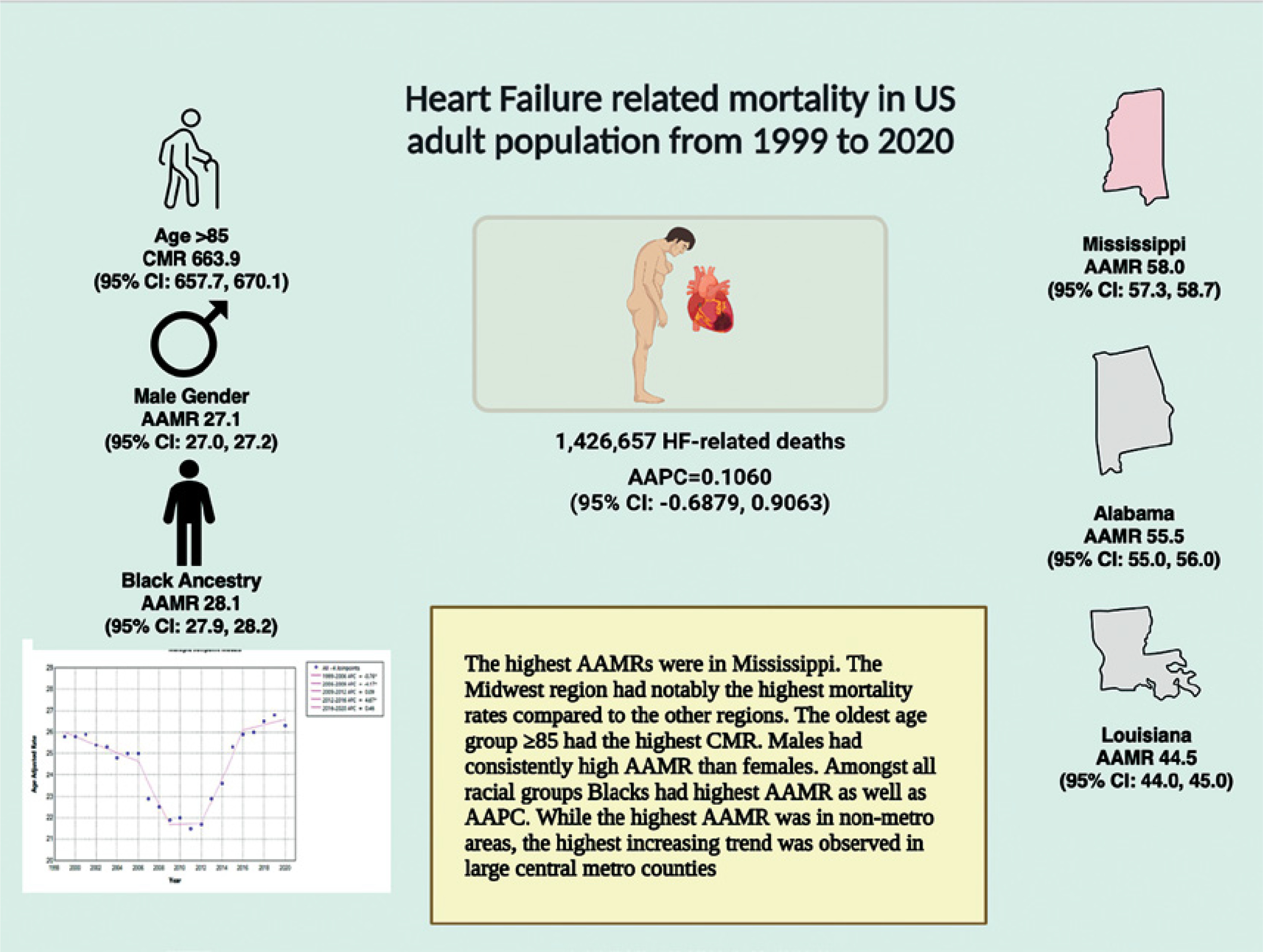
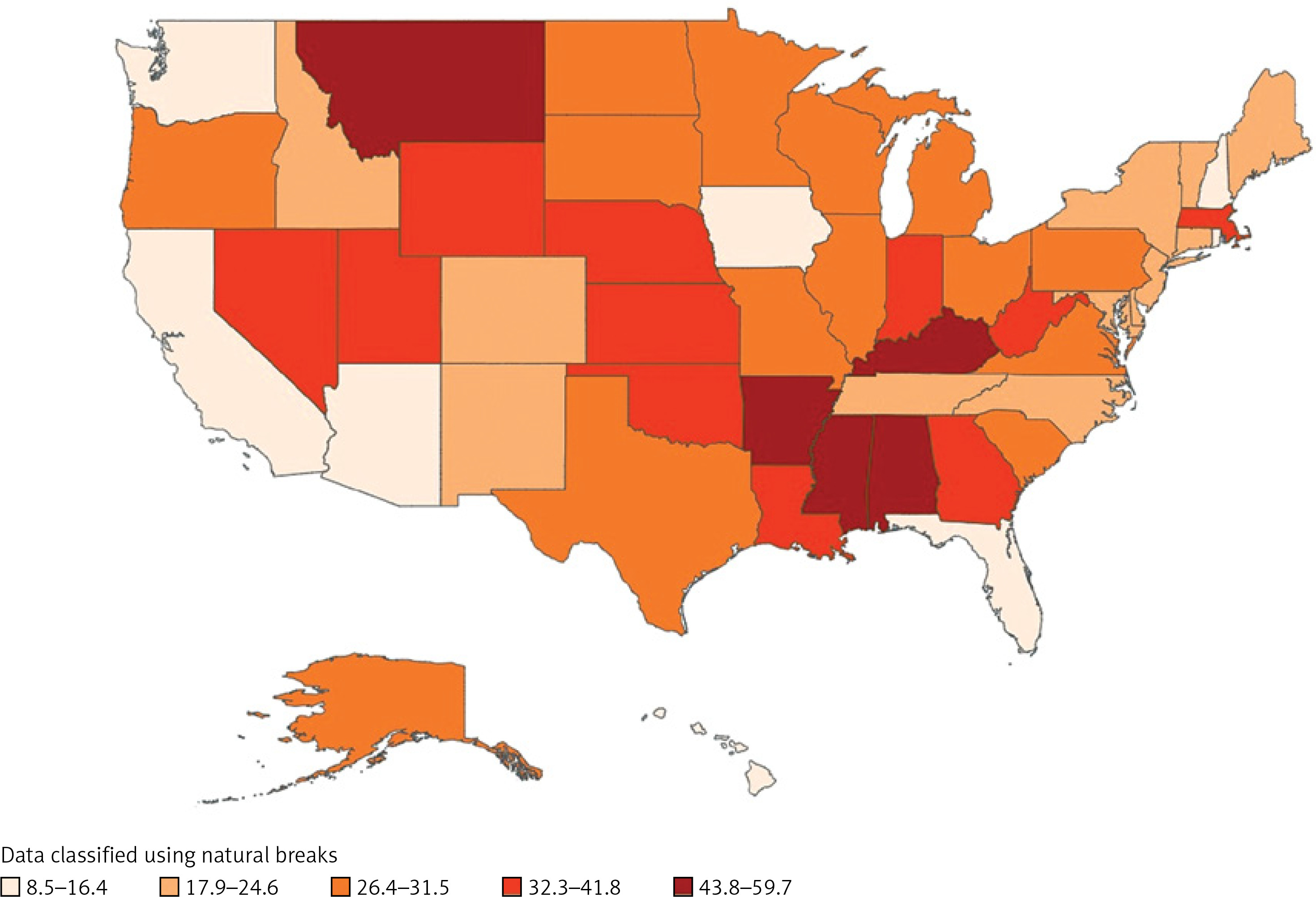
Between 1999 and 2020, there were 1,426,657 documented HF deaths in the United States. Of these deaths, 422,781 (29.6%) occurred in inpatient medical facilities, 423,473 (29.7%) occurred in nursing homes or long-term care facilities, and 26.8% occurred in the deceased’s home. The remaining deaths occurred in other locations. The overall AAMR (95% CI: 24.5, 24.6) was 24.5 per 100,000 (Table I). With an AAMR of 58.0 (95% CI: 57.3, 58.7), Mississippi had the highest mortality rate, followed by AAMRs of 55.5 (95% CI: 55.0, 56.0) in Alabama and 44.5 (95% CI: 44.0, 45.0) in Louisiana. The South’s mortality rate (AAMR = 27.2; 95% CI: 27.2, 27.3) was higher than that of the Northeast, Midwest, and West (Figure 1).
Table I
Demographic characteristics of US population and heart failure-related mortality in US from 1999 to 2020
Figure 1
Central illustration of heart failure-related mortality in US adult population from 1999 to 2020
Overall trends
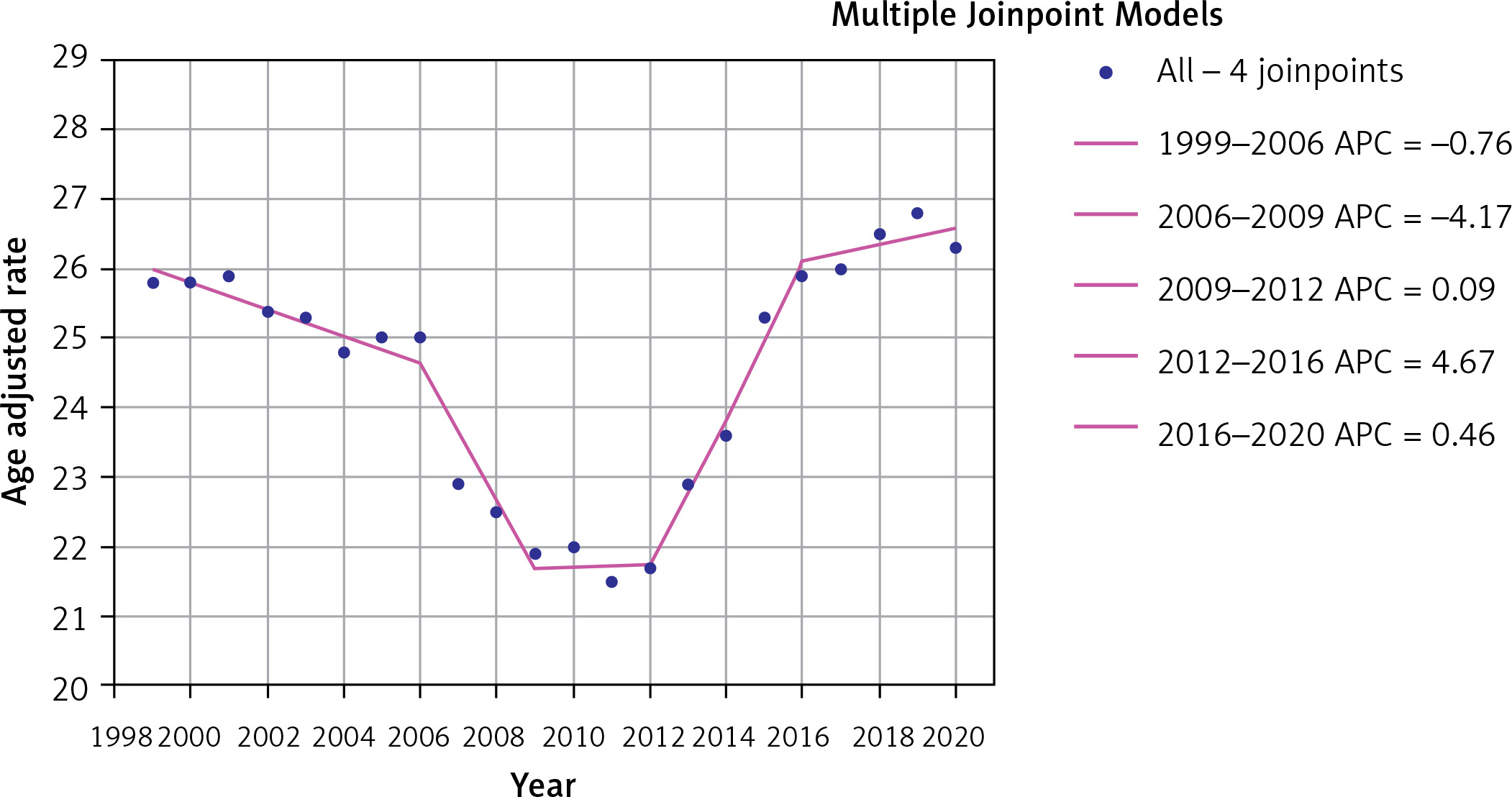
With an overall AAPC = 0.11; 95% CI: –0.69, 0.91, the AAMR was 25.8 (95% CI: 25.6, 26.0) in 1999 and 26.3 (95% CI: 26.1, 26.5) in 2020. Between 1999 and 2006 (APC = –0.76; 95% CI: –1.23, –0.29) and between 2006 and 2009 (APC = –4.1714; 95% CI: –7.92, –0.27), there was a notable, gradual decline. Figure 2 illustrates the near-plateau that followed from 2009 to 2012 (APC = 0.09; 95% CI: –4.00, 4.35), then a notable increase from 2012 to 2016 (APC = 4.67; 95% CI: 2.72, 6.66) and yet another decline from 2016 to 2020 (APC = 0.46; 95% CI: –0.63, 1.57).
Trends by age group
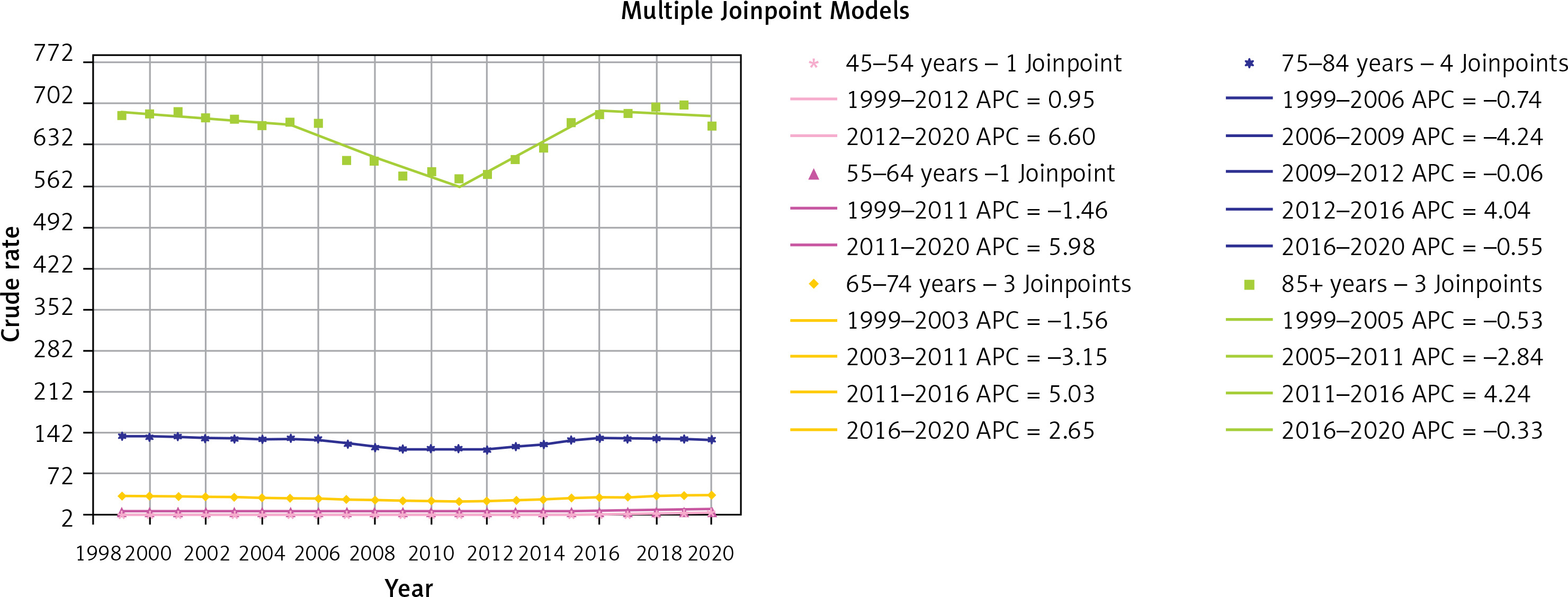
Through the study period, older ages had a higher crude mortality rate (CMR), with the 2020 CMR being 663.9 (95% CI: 657.7, 670.1) in the ≥ 85 age group. Overall crude mortality rates were higher as age increased, with 648.5 (95% CI: 647.0, 649.9) in the ≥ 85 age group, followed by 127.3 (95% CI: 126.9, 127.7) in the 75–84 age group, 31.6 (95% CI: 31.4, 31.7) in 65 to 74 years, 9.5 (95% Cl: 9.4, 9.6) in 55 to 64 years, 2.9 (95% CI: 2.8, 2.9) in 45 to 54 years, 0.8 (95% CI: 0.8, 0.9) in 35 to 44 years, 0.3 (95% CI: 0.3, 0.3) in 25 to 34 years and 0.1 (95% CI: 0.1, 0.1) in 15 to 24 years. On the other hand, the age groups with the highest AAPC were the 45 to 54 years group (AAPC = 3.06; 95% CI: 2.22, 3.92), followed by 55 to 64 years (AAPC = 1.66; 95% CI: 1.32, 2.00), 65 to 74 years (AAPC = 0.15; 95 CI: –0.32, 0.62), 75 to 84 years (AAPC = –0.22; 95% CI: –0.97, 0.53), and 85 and above years (AAPC =–-0.05; 95% CI: –0.79, 0.70), as demonstrated in Figure 3.
Trends by gender
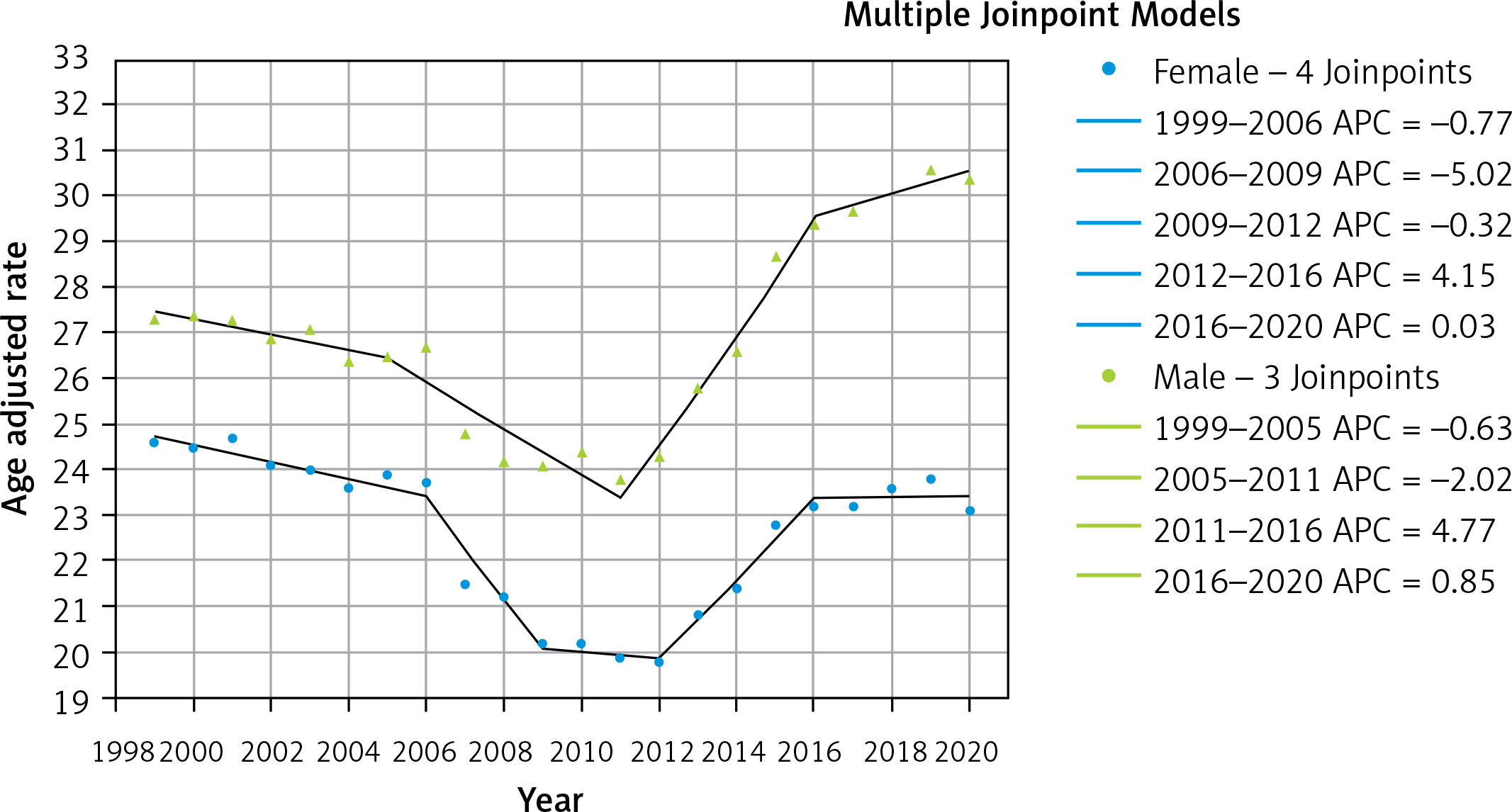
Following the trend of population as a whole, men and women had an initial drop in AAMR, which was followed by an increase from 2013 to 2020. Males had a consistently higher annual AAMR than females, with an overall AAMR of 27.1 (95% CI: 27.0, 27.2) versus 22.6 (95% CI: 22.5, 22.6). In addition, between 1999 and 2020, males had higher AAPC (AAPC = 0.51; 95% CI: –0.09, 1.11) versus females, AAPC (AAPC = –0.26; 95% CI: –1.15, 0.64), as demonstrated in Figure 4. Overall, the death rate was 42.4% for men and 57.6% for women.
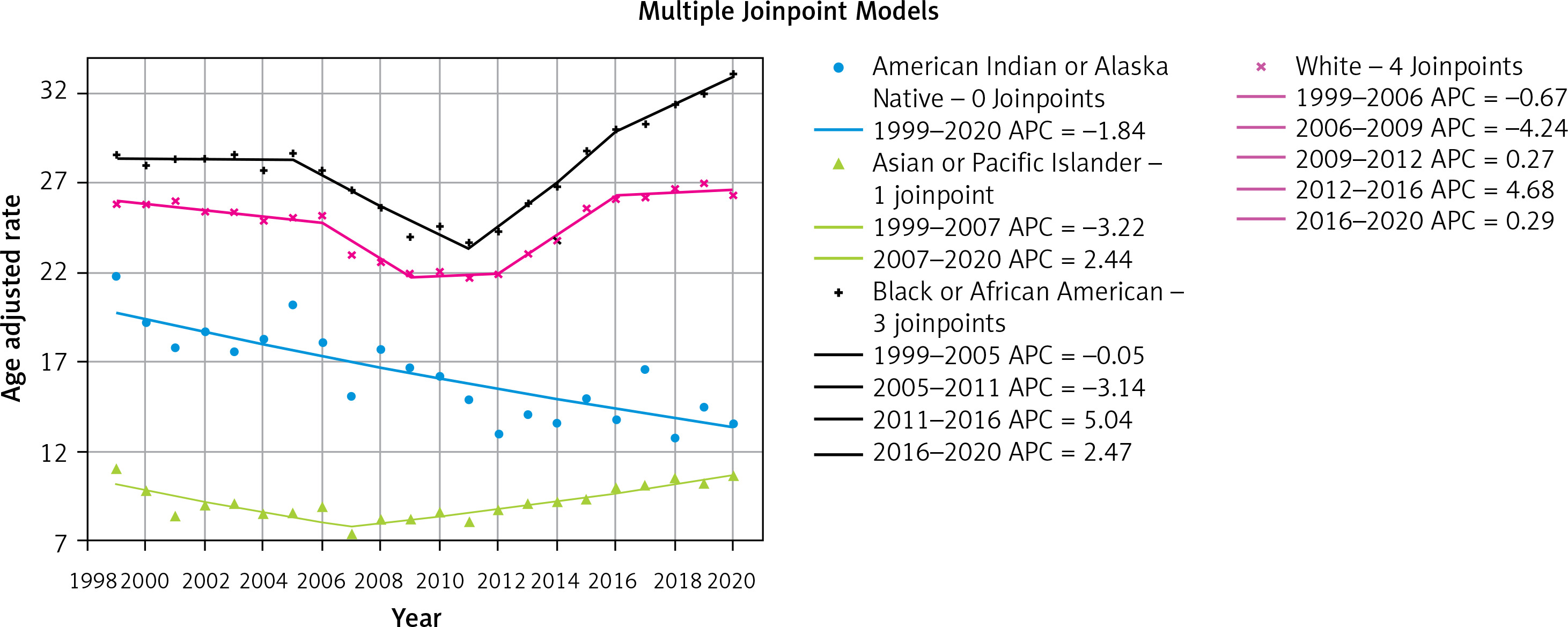
Trends stratified by race/ethnicity
Black ancestry people had the highest AAMR (AAMR = 28.1; 95% CI: 27.9, 28.2) and the highest AAPC (AAPC = 0.71; 95% CI: 0.18, 1.25). The AAMR for Hispanic or Latino ancestry individuals was 14.1 (95% CI: 14.0, 14.2). The AAPC for Asian or Pacific islands ancestry individuals was 0.25 (95% CI: –0.43, 0.93). The AAPC for the White ancestry cohort was 0.12 (95% CI: –0.78, 1.04). Finally, the lowest AAPC (AAPC = –1.84; 95% CI: –2.42, –1.25) was observed among American Indians or the Alaska Natives ancestry group (Figure 5).
Trends stratified by geographical region and county
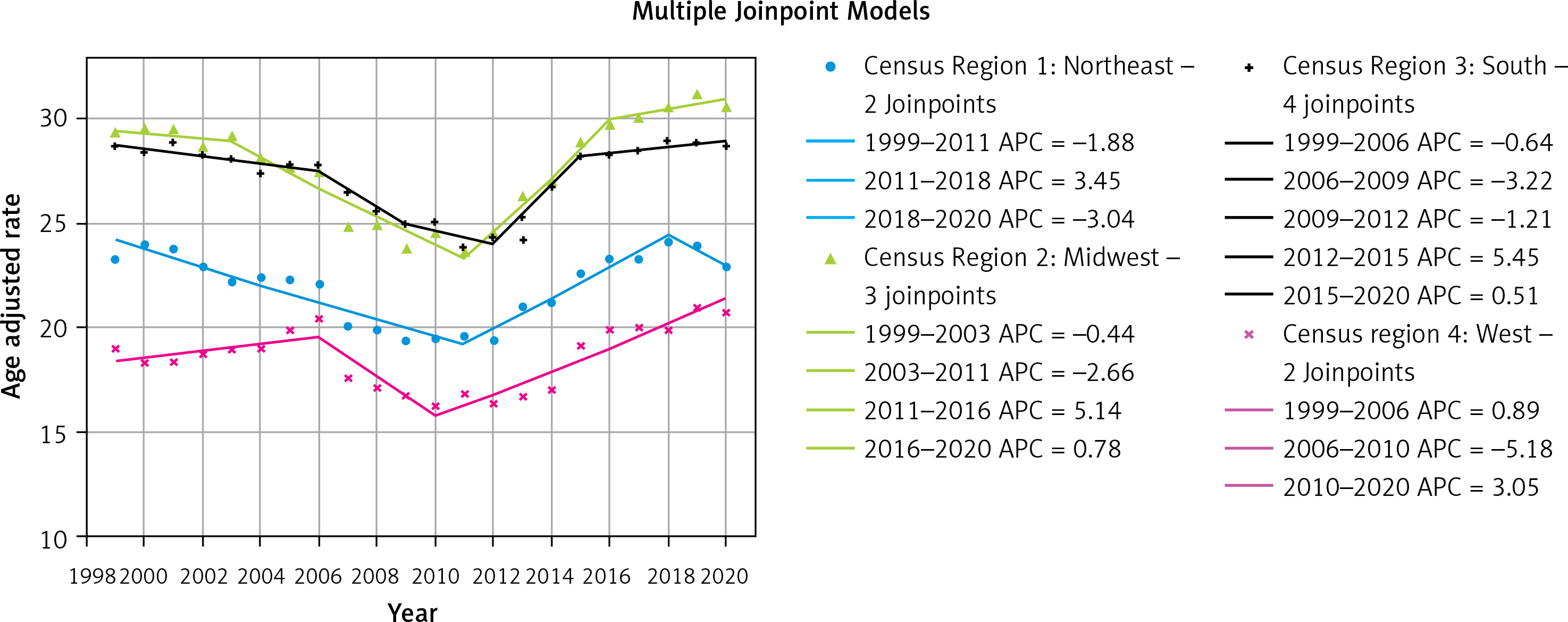
The South region had an AAMR of 27.2 (95% CI: 27.2, 27.3), while the Midwest had the highest AAMR of 27.8 (95% CI: 27.7, 27.9). The Midwest (AAPC = 0.23, 95% CI: –0.51, 0.98), South (AAPC = 0.03, 95% CI: –0.79, 0.85) and Northeast (AAPC = –0.25, 95% CI: –1.06, 0.57) had the lowest AAPC overall, with the West having the highest AAPC (AAPC = 0.72; 95% CI: –0.29, 1.73), as demonstrated in Figure 6.
Figure 6
Trends of heart failure-related, age-adjusted mortality rate (per 100,000) stratified by census region in US, 1999 to 2020
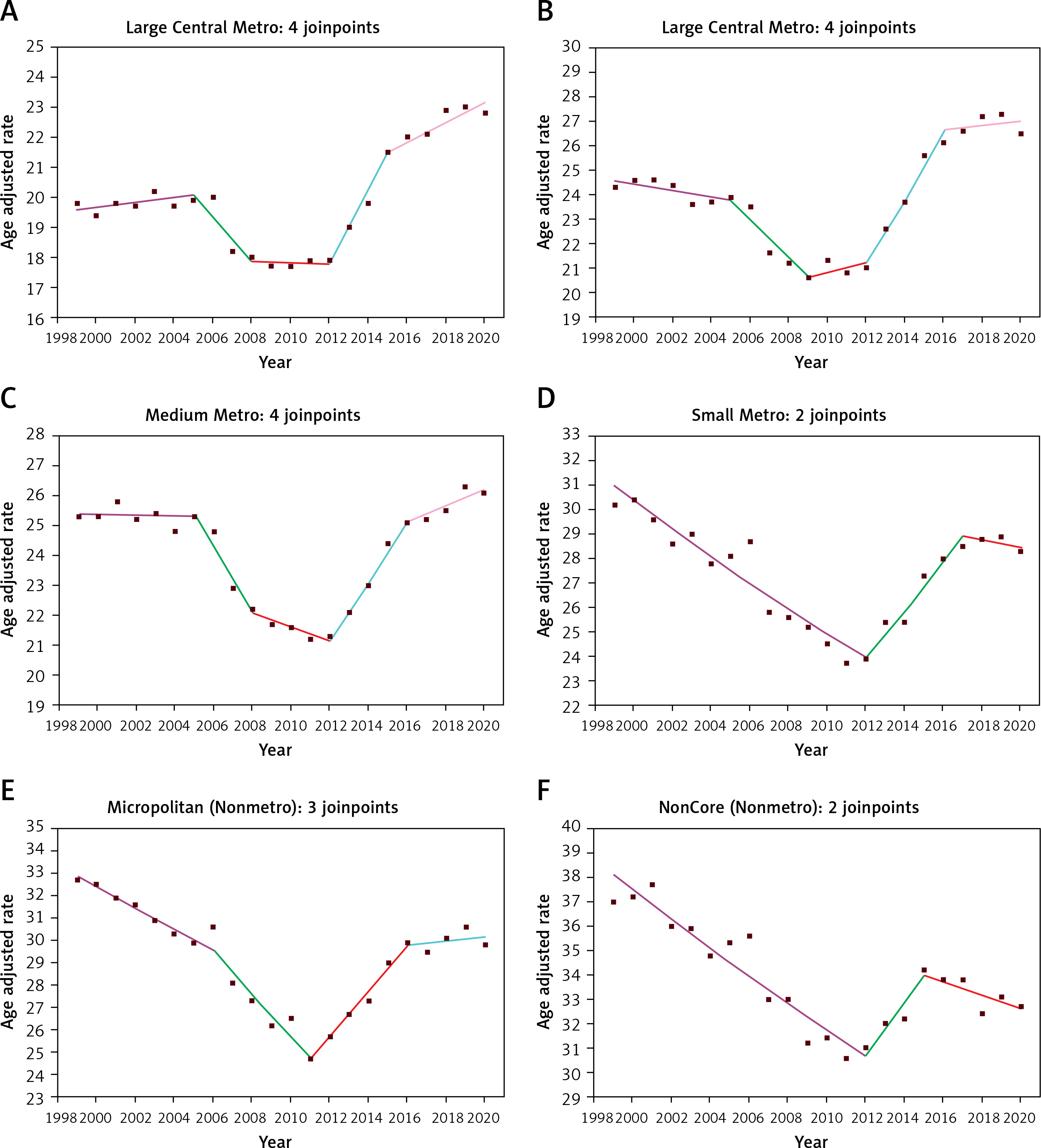
The non-metropolitan NonCore (AAMR = 33.7; 95% CI: 33.5, 33.9) had the highest AAMR, followed by the non-metropolitan Micropolitan (AAMR = 29.1; 95% CI: 28.9, 29.2). The largest AAPC was found in large Central Metro counties (AAPC = 0.80; 95% CI: –0.11, 1.72). With an AAPC of –0.74 (95% CI: –1.76, 0.29), NonCore (Nonmetro) had the lowest AAPC; the difference was not statistically significant. Based on the data presented in Figure 7, the AAPC values for the Large Fringe Metro were 0.45 (95% CI: –0.63, 1.54), Medium Metro was 0.15 (95% CI: –0.55, 0.87), Small Metro was –0.40 (95% CI: –1.12, 0.33), and Micropolitan (Nonmetro) was –0.40 (95% CI: –0.85, 0.05). With an AAMR of 58.0 (95% CI: 57.3, 58.7), Mississippi had the highest mortality rate, followed by AAMRs of 55.5 (95% CI: 55.0, 56.0) in Alabama and 44.5 (95% CI: 44.0, 45.0) in Louisiana (Figure 8).
Figure 7
Trends of heart failure-related, age-adjusted mortality rate (per 100,000) stratified by Urban-Rural 2013 Classification Scheme in US, 1999 to 2020. Joinpoint regression model for urban–rural trends (2–4 segments). A – Large Central Metro – 1999 to 2005 (APC = 0.42; 95% CI: –0.32, 1.17), 2005 to 2008 (APC = –3.84; 95% CI: –8.12, 0.65), 2008 to 2012 (APC = –0.13; 95% CI: –2.53, 2.33), 2012 to 2015 (APC = 6.62; 95% CI:1.96, 11.50), and 2015 to 2020 (APC = 1.47; 95% CI: 0.60, 2.35). B – Large Fringe Metro – 1999 to 2005 (APC = –0.53; 95% CI: –1.47, 0.41), 2005 to 2009 (APC = –3.52; 95% CI: –6.39, –0.57), 2009 to 2012 (APC = 0.98; 95% CI: –5.26, 7.63), 2012 to 2016 (APC = 5.84; 95% CI: 2.92, 8.84), and 2016 to 2020 (APC = 0.33; 95% CI: –1.26, 1.94). C – Medium Metro – 1999 to 2005 (APC = –0.05; 95% CI: –0.67, 0.57), 2005 to 2008 (APC = –4.42; 95% CI: –8.05, –0.65), 2008 to 2012 (APC = –1.08; 95% CI: –3.18, 1.07), 2012 to 2016 (APC = 4.40; 95% CI: 2.35, 6.49), and 2016 to 2020 (APC = 1.06; 95% CI: –0.08, 2.2120). D – Small Metro – 1999 to 2012 (APC = –1.96; 95% CI: –2.40, –1.53), 2012 to 2017 (APC = 3.87; 95% CI: 1.44, 6.35), 2017 to 2020 (APC = –0.52; 95% CI: –3.93, 3.01). E – Micropolitan – 1999 to 2006 (APC = –1.48; 95% CI: –2.07, –0.89), 2006 to 2011 (APC = –3.47; 95% CI: –4.65, –2.28), 2011 to 2016 (APC = 3.75; 95% CI: 2.48, 5.02), and 2016 to 2020 (APC = 0.31; 95% CI: –0.81, 1.44). F – NonCore – 1999 to 2012 (APC = –1.65; 95% CI: –2.00, –1.29), 2012 to 2015 (APC = 3.42; 95% CI: –3.84, 11.23), and 2015 to 2020 (APC = –0.80; 95% CI: –2.35, 0.77)
Discussion
Incidence
The statistical data collected during this study demonstrate an irregular pattern in AAMR over two decades in the US population. A gradual decline was observed until 2009, followed by a plateau to 2012, followed more concerningly by a sharp rise in AAMR thereafter. The overall change in incidence of HF in the US has been estimated by several studies, and generally shows a declining overall incidence of heart failure between 1990 and 2016, with however some increase in Black populations and an increasing overall incidence of heart failure with preserved ejection fraction (HFpEF) [9].
The reasons for the gradual decline in AAMR until 2009 can only be speculated and could be artefactual due to HF being entered less frequently on death certificates for unknown reasons. It could however be argued to be linked to the steady advancement in therapies and implementation of newer guidance, such as the addition of the mineralocorticoid receptor antagonist spironolactone in the 2005 American Heart Association (AHA) guideline on heart failure [10]. Significantly, this would be the last major addition to standard pharmacological management of HF until the PARADIGM HF trial led to the inclusion of angiotensin receptor-neprilysin inhibitors (sacubitril-valsartan) in guidelines over a decade later [11]. Disparities involving gender, age, geographical distribution [12], genetic predispositions, and access to health care however also have a pivotal role in driving these statistics.
Following 2012, a drastic increase in mortality rates in heart failure patients can be observed, returning to around 25–26 in 100,000, which was similar to the level observed between 1999 and 2006. One contributing factor to this could be an increase in the elderly population in the USA, with the census held in 1999 reporting the percentage of adults more than 65 years of age to be 12.7% [13] and increasing to 16.8% by 2020 [14]. This will invariably lead to higher mortality as a result of increased frailty, with patients having less physiological reserve to overcome acute illnesses and consequently more complications from illness.
With advancing age, additionally comes a higher comorbidity burden in the older population [7]. However, data additionally show that comorbidity has increased in younger age groups [15]. The estimated age-standardized prevalence of diabetes increased significantly from 9.8% in 1999 to 14.3% in 2018 [16]. All the while, prevalence of hypertension in the USA in 2018 was 49.64% [17]. Similarly, other factors such as obesity, smoking, and sedentary lifestyles have a role in increasing AAMR in heart failure patients. It is possible, however, that the return to an AAMR similar to that seen before 2006 may suggest that despite the introduction of advancing therapies, HF mortality has actually been affected very minimally.
Our findings are consistent with other data collected in heart failure patients in demonstrating the pattern of mortality and AAMR [18]. Reducing mortality in heart failure patients requires a multifaceted approach that encompasses both preventive and therapeutic strategies. Timely and appropriate interventions can help change the trends of mortality due to heart failure.
Age
The data collected during the study show a rising trend in HF-associated mortality among older individuals as compared to younger adults. According to 2020 statistics, AAMR is highest for ages > 85 years. The observed phenomenon can be ascribed to various factors, including physiological alterations associated with aging and the presence of comorbidities. Elderly patients experiencing heart failure exhibit a combination of structural and functional changes, such as an increase in sympathetic nervous activity, left ventricular wall hypertrophy, myocardial fibrosis, apoptosis, micro- and macrovascular coronary sclerosis, and aortic stiffness [19]. AAPC for ages 65 years and above years have shown an increasing trajectory over the last two decades. The causes of this are complex and may include recent budget cuts in the healthcare sector as well as an increase in comorbid conditions such as diabetes, obesity, and chronic kidney disease, all of which are linked to an increased risk of heart failure in the country’s aging population [7]. Improving the mortality rate of the elderly population can be achieved by the introduction of screening programs and routine medical examinations by healthcare professionals. To reduce mortality, the healthcare system would need to use a multimodal strategy, avoiding polypharmacy and implementing evidence-based treatment plans.
Gender
The study illustrates that men consistently had higher heart failure AAMRs than women throughout the study period despite females having higher overall mortality secondary to HF. Other studies with similar parameters have reflected similar outcomes [20–22]. Women live longer than men in general but also with advanced heart failure after adjusting for baseline clinical factors, which may explain the higher crude mortality in females; men display higher likelihood of death during follow-ups [22]. Notably, women exhibit approximately 20% lower risk of mortality or hospitalization for both cardiovascular and non-cardiovascular events. These survival differences are primarily influenced by a collection of biological, behavioral, and socio-economic factors. Men are predisposed to HF with reduced ejection fraction, while women primarily present with HF with preserved ejection fraction [21]. Ongoing molecular studies are investigating the role of gender-based variations in cardiac physiology and hypertrophy that may contribute to the survival advantage for women with heart failure [20, 22]. Paradoxically, females diagnosed with HF experience a more compromised quality of life that persists even after accounting for age and other confounding factors [8]. Further research is needed to understand the differences in HF between sexes and the implications they have for management and outcomes.
Race
This study also demonstrated noteworthy differences between the diverse racial groups, emphasizing that Black ancestry individuals have a disproportionately higher HF AAMR, a disparity that has widened over time, followed by the white ancestry cohort, whose AAMR has stabilized over the past couple of years. The American Indians and Alaskan natives had a consistently declining trend over the study period, whilst Asian/Pacific Islanders had the lowest AAMRs. Higher incidences in the Black demographic have also been observed in other studies [2, 23–25]. A recent report by CDC WONDER revealed a 2.97-fold higher age-adjusted cardiovascular death rate related to heart failure for African-American women and a 2.60-fold elevation for African-American men aged 35 to 64 compared to their White counterparts [2]. The divergent health outcomes may be explained by differences in access to advanced healthcare therapies and effective heart failure treatments. Despite the hydralazine and isosorbide nitrates (H/I) combination being data-proven as more advantageous for black patients, only 11% were utilizing this treatment for HF [25]. The burden of cardiovascular diseases, particularly the occurrence of heart failure at an earlier age, left ventricular hypertrophy, and a higher incidence of hypertension, is also understood to be more pronounced in the Black demographic compared to the others [24]. Even after adjusting for factors such as age, comorbidities, medical compliance, and the causes and severity of heart failure, individuals from the Black ancestry population consistently demonstrate higher risks of mortality from all causes [22, 23]. Further research and a comprehensive analysis of health-related factors, including lifestyle, genetics, socioeconomic status, and healthcare infrastructure, are needed to fully comprehend these racial differences, which could help mitigate the disparities observed in heart failure-related mortality that have been noted among the different demographic groups in the USA.
Geographical region/county and urban vs. rural
Examining individual risk variables is critical for determining the likelihood of development of HF. However, a geographical perspective helps to better understand the impact of health policy actions. The large regional diversity in HF mortality may, to some degree, be understood by differences in outpatient cardiology practices, the influence of state legislators (such as Medicaid expansion), and the load of comorbidities. Our results revealed the highest AAMR in the Midwest region throughout the 21 years of death certificate data, closely followed by the South region. These findings are consistent with these being the most persistently poverty-stricken areas [26]. Ahmad et al. also found a correlation between regional poverty and high HF and CHD-related mortality [27].
Furthermore, these geographic variations are also influenced by the prevalence of leading risk factors for HF, such as diabetes, obesity, hypertension, and individual physical inactivity in the population [3]. These differences are well noted in urban vs. rural environments where large-medium metropolitan areas were found to have an increasing trend of AAMR over the two decades compared to small non-metropolitan areas, which had an overall decrease. The greater prevalence of obesity in more urban settings is perhaps a consequence of busy lifestyles and less focus on physical activity [28].
Limitations
This study has various limitations that need to be carefully considered. Initially, there is a risk of misrepresenting or omitting HF as a cause of death due to dependence on ICD codes and death certificates, where documentation and recording of data can be inaccurate. Furthermore, the dataset lacks critical clinical factors such as vital signs, laboratory results, echocardiographic data, and genetic analysis, which might improve the overall characterization of HF. Thirdly, there is a lack of information on medical therapy and the therapeutic methods used for HF, as well as a lack of data on the etiologies of heart failure and the duration of therapy due to the limitations of clinical coding. Finally, the existing statistics do not sufficiently address the socioeconomic determinants of health, which are critical for understanding access to care.
In conclusion, while mortality rates fluctuated, trends show a significant increase since 2012, particularly in those over the age of 85, whilst younger age groups exhibited few to no changes. Gender discrepancies show that males had higher AAMR despite women having greater total mortality due to HF. Racial differences observed greater mortality rates among Blacks, while the geographical differences underscore the relevance of regional policies and healthcare infrastructure in reducing AAMR, underlining the necessity for tailored interventions to reduce HF mortality and enhance outcomes across varied demographic groups and geographic locations and pointing to increased depravation as a driver of mortality in HF. The increasing AAMR over past decades highlights a need for lifestyle changes and more focus on preventative measures from an early age.