
Introduction
The skin, encompassing the epidermis, dermis, and subcutaneous tissue, serves vital functions in protection, thermoregulation, and sensory perception [1, 2]. Burn injuries, caused by heat, chemicals, electricity, or radiation, exhibit histological zones of coagulative necrosis, stasis, and hyperemia [3, 4]. The depth determines burn classification (1st to 4th degree), impacting healing and scarring [5, 6]. Although burns have a higher degree of systemic inflammatory response and show higher generalized capillary permeability than other wounds [7], their healing follows the traditional wound healing model [7, 8]. This particular model is characterized by three phases: inflammation, multiplication, and maturation [9]. The inflammatory phase involves tumor necrosis factor α (TNF-α), cytokines, and growth factors, triggering hemostasis and inflammation stages. Platelet activation, coagulation cascade, and subsequent angiogenesis characterize this phase [10]. The multiplication phase includes epithelium formation, capillary growth, granulomatous tissue development, and wound shrinkage, influenced by VEGF, PDGF, and bFGF [11, 12]. The remodeling phase, lasting weeks to years, sees collagen type III replaced by type I, forming scars. Burn depth influences healing speed and esthetic recovery, with deeper burns resulting in longer healing periods and potential hypertrophic scarring [13]. Understanding the role of TNF-α, cytokines, and growth factors is crucial for effective burn care, as they play pivotal roles in inflammation, tissue repair, and scar formation [9, 14, 15].
Statins are widely used for the treatment of hyperlipidemia, and their main pharmacological action is served by the inhibition of 3-hydroxy-3-menthyl glutamate coenzyme A (HMG-CoA) reductase, a key enzyme in cholesterol biosynthesis, which converts HMG-CoA to mevalonic acid [16]. However, apart from their lipid-lowering action, recent studies have proved that statins, thanks to their pleiotropic effects, present anti-inflammatory and anti-oxidant activity, thereby amplifying the processes of angiogenesis, re-epithelization, and fibroblast proliferation [17]. Rosuvastatin, a synthetic hydrophilic statin, effectively lowers low-density lipoprotein and triglyceride levels while increasing high-density lipoprotein levels [18]. Notably, research has revealed that rosuvastatin specifically targets reactive oxygen species-induced oxidative stress and inflammation, making it a potent intervention for managing wound and burn healing [19].
The purpose of this experimental study was to evaluate the action of rosuvastatin on the pathophysiological disorders of burn injury. The evaluation was done by reproducing partial-thickness burns in rats. The experiment then attempted to study the processes observed in the body as a whole, using inflammatory markers, and on the skin locally, by histopathological examination of the affected tissues. In addition, the action of rosuvastatin in the above processes was also examined.
The current evidence endorsing the potential positive impact of rosuvastatin on wound healing is predominantly derived from animal studies characterized by limited sample sizes and short-term observation periods. Furthermore, the specific role of rosuvastatin in the context of burn wounds remains relatively unexplored.
Material and methods
A randomized prospective experimental study was carried out in male Wistar Albino rats with intervention and control groups. The study was a clinical trial, that is, a prospective randomized open-label study in which a comparison was made with a negative control group (placebo).
This was an experimental study of the anti-inflammatory action of rosuvastatin on burns of partial thickness. The application of this type of statin concerning the healing of a burn injury has not been studied previously.
Experimentation should therefore be carried out in groups of animals and not in groups of patients, with all the limitations and variations expected to occur. However, it may be a starting point for subsequent studies, once the hypotheses to be tested are confirmed. The experimental part of the study was conducted at the Laboratory of Scientific Research and Experimental Surgery of the Second Propedeutical Department of Surgery of the Aristotle University of Thessaloniki (Hippocrates Hospital).
Animals
Thirty-six male Wistar rats were used as animal models. The classification of the animal model is: Class: Mammalia, Order: Rodentia, Suborder: Sciurognathi, Family: Muridae, Genus: Rattus, Species: norvegicus, Stem: Wistar.
The rats were 12 to 16 weeks old with a body weight of approximately 300 g. Hosting of all animal models during the study took place in plexiglass cages, at a temperature between 20°C and 22°C, with a relative humidity between 55 and 65%, and a light cycle of 12 h of light and 12 h of darkness. Animal models had free access to water and food (ad libitum), which is specific to rats (blight no. 510, ELVIZ). Regarding the genetic standardization of animal models, there was a randomized series of experimental animals, while in the case of microbiological standardization there were standard (conventional) experimental animals.
Preparation of animals
All procedures were approved by the Committee for Bioethics and Ethics of Aristotle University of Thessaloniki and were conducted in accordance with its established guidelines. Animals were obtained from the laboratory of experimental surgery of the 2nd Propedeutical Department of Surgery of Aristotle University.
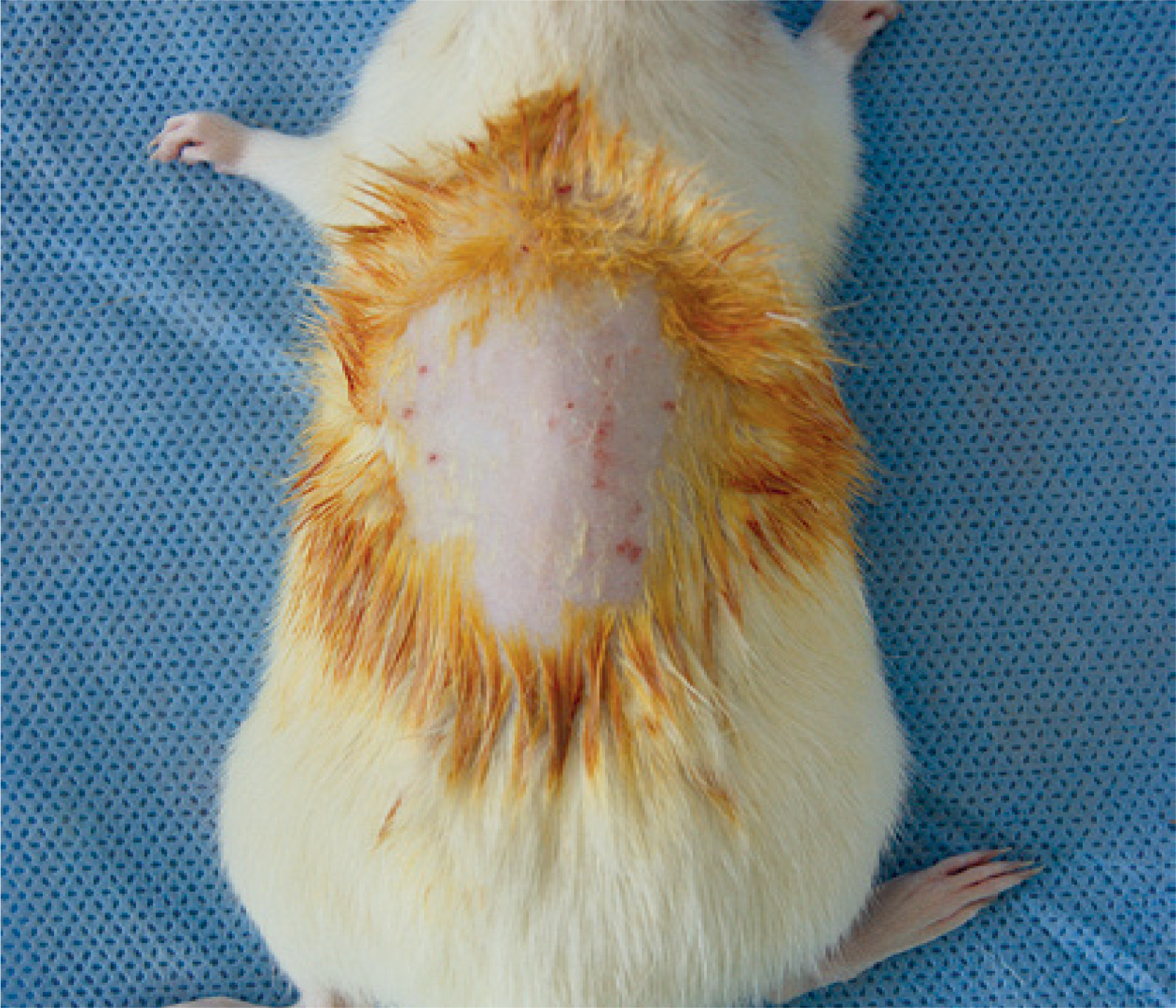
The operation began with the induction of anesthesia after immobilization of the animal with a special glove and intraperitoneal administration of ketamine hydrochloride (Ketalar amp, 50 mg/ml, Parke-Davis) at a dose of 70 mg/kg BA and xylazine (20 amp, mg/ml, Bayer), at a dose of 10 mg/kg BA. The dorsum of the rat was shaved. The shaver was held at a 45-degree angle to the skin and a maximum of two crosses was allowed, in order to minimize skin trauma. Subsequently, the rat was immobilized on the surgical table and preparation of the surgical field was conducted. After anesthesia and under aseptic conditions, the animal’s hair was removed in the area of the back, on a surface of at least 5 cm2 (Figure 1).
Preparation of rosuvastatin and placebo cream
For the preparation of the mixture for the study group, 20 g of Eucerin cream base and 20 rosuvastatin 20 mg tablets were used, mixed, and homogenized. For the preparation of the mixture that was used in the placebo group, 20 g of Eucerin cream base was used.
Wound infection model
To cause the burn of the partial thickness of skin, a special metal iron cylindrical bar 2 cm in diameter, 2.5 mm thick, and weighing 500 g was used. These dimensions ensured efficient heat transfer [20]. The seal is composed of stainless steel and features a wooden handle. Thermal burns were performed on the back of 36 white Wistar rats. The metal seal was heated to 85°C. The thermal burn per rat was caused by placing the metal seal on the skin of the back for 10 s. This method induced a deep burn of the partial thickness of the skin [20]. After removing the seal, the wound was washed with saline, a photograph of the burn wounds was taken, and a record of the burnt surface of each animal was made. The animals were then placed in their cages and monitored until anesthesia had elapsed. The eschar was removed on the first post-burn day with surgical scissors. Subsequently, Eucerin cream or a mixture of Eucerin with rosuvastatin was applied daily, depending on the group of each rat. The day of burn removal is defined as day 0 and the first application of Eucerin cream and Eucerin cream mixed with rosuvastatin took place on that day. Wounds were covered with Tegaderm dressing (Figures 2, 3).


Animal grouping
Thirty-six male rats were randomly divided into two main groups, the study group, and the placebo group, depending on whether the rosuvastatin cream excipient was used or not. These groups were in turn divided into 3 subgroups of 6 rats depending on the day that the animal was sacrificed. The investigation of the healing effect of the solution was assessed on the 3rd, 6th, and 9th burn days. Once the burn was induced, the animals were divided according to the days their burn wound was going to be studied.
Study group (SG)
1. The rats in this group were burned to a partial thickness using a metal signet ring and rosuvastatin cream excipient was applied to the burnt surface.
1 a) Study group 1a – sacrifice on the 3rd post-burn day
This group consisted of 6 rats that were sacrificed on the 3rd post-traumatic day.
1 b) Study group 1b – sacrifice on the 6th post-traumatic day
This group consisted of 6 rats that were sacrificed on the 6th post-traumatic day.
1 c) Study group 1c – sacrifice on the 9th post-traumatic day
This group consisted of 6 rats that were sacrificed on the 9th post-traumatic day.
Placebo group (PG)
2. For rats of this group, once partial skin burn had been caused using a metal signet ring, Eucerin cream was applied to the burnt surface.
2 a) Placebo group – sacrifice on the 3rd post-traumatic day
This group consisted of 6 rats that were sacrificed on the 3rd post-traumatic day.
2 b) Placebo group – sacrifice on the 6th post-traumatic day
This group consisted of 6 rats that were sacrificed on the 6th post-traumatic day.
2 c) Placebo group – sacrifice on the 9th post-traumatic day
This group consisted of 6 rats that were sacrificed on the 9th post-traumatic day.
Determination of plasma inflammatory mediator levels, TNF-α, and procalcitonin levels
After a macroscopic estimation, the values of the following parameters were determined as well:
– Procalcitonin (PCT) levels. Procalcitonin is a polypeptide of 116 amino acids. After a severe burn, high serum PCT levels are released, enforcing the systemic inflammatory response syndrome (SIRS). Consequently, high PCT plasma levels are correlated with delayed wound healing, septic complications, and clinical consequences (systemic inflammatory response index) [21–23].
– Tumor necrosis factor (TNF-α), a potent chemotactic agent that promotes local or systemic inflammation (TNF-α is a potent pyrogen) and stimulates the acute phase response [24, 25].
Subsequently, the values of the above parameters were determined on the 3rd, 6th, and 9th post-burn day.
Finally, the tissue sections from the above tissues were sent for histopathological examination with an optical microscope.
The levels of TNF-α tumor necrosis factor were determined using the ELISA method. The antigen was added to the wells for the first incubation. After incubation, the wells were washed and a monoclonal antibody that is specific to TNF-α was added and incubated for an hour. A second-detector antibody and finally, after washing, a substrate solution was added, to produce a colored reaction product. The levels of PCT were measured by a chemiluminescent detection system and an immunoluminometric method [26]. For histopathological examination, the preparations were embedded in paraffin blocks, cut into 3 µm thick sections, and stained with hematoxylin-eosin staining, as well as immunohistochemical staining.
Monitoring of wound healing
In all rats, the lesion was macroscopically evaluated, and photographed, and the burnt surface was measured. The burning surface size was measured digitally using ImageJ Software, version 1.45 (National Institutes of Health [NIH], USA). Burn lesions were used to calculate wound healing based on the following formula: wound healing rate = [burn area (day X)/burn area (day 0)] × 100, planimetry method.
Statistical analysis
Statistical data processing was conducted using the R Studio software. The significance level was set at 0.05. If the data were normally distributed, the results were described by calculating the mean and the standard deviation. Comparison between values was done by Student’s t-test. If the data did not follow a normal distribution, the results were described by calculating the median and range of values. The comparison between the groups was done by the Mann-Whitney test. If there was a statistically significant difference using eta squared, we could find out what percentage of this difference was due to the intervention. The measured values were expressed as the arithmetic mean ± standard deviation. For the comparison of the variables in the groups of animals under study, the normality test was used, the t-test for independent samples if there was a normal distribution, or the non-parametric Mann-Whitney test if there was no normal distribution, these being tests used to compare averages. Due to the small number of animals per group, the Levene test for equality of variances was applied within the t-test.
Outcome measures
The primary outcome was the confirmation of the hypothesis of the anti-inflammatory activity of rosuvastatin in the healing of partial-thickness burn wounds. This was done by recording reduced values of the measured parameters in the experimental group. Our initial hypothesis was supported by the histological examination, the reduced levels of pro-inflammatory cytokines, and the faster macroscopic healing of the trauma compared to the control group.
Results
Effect of rosuvastatin on burn-induced TNF-α and procalcitonin levels
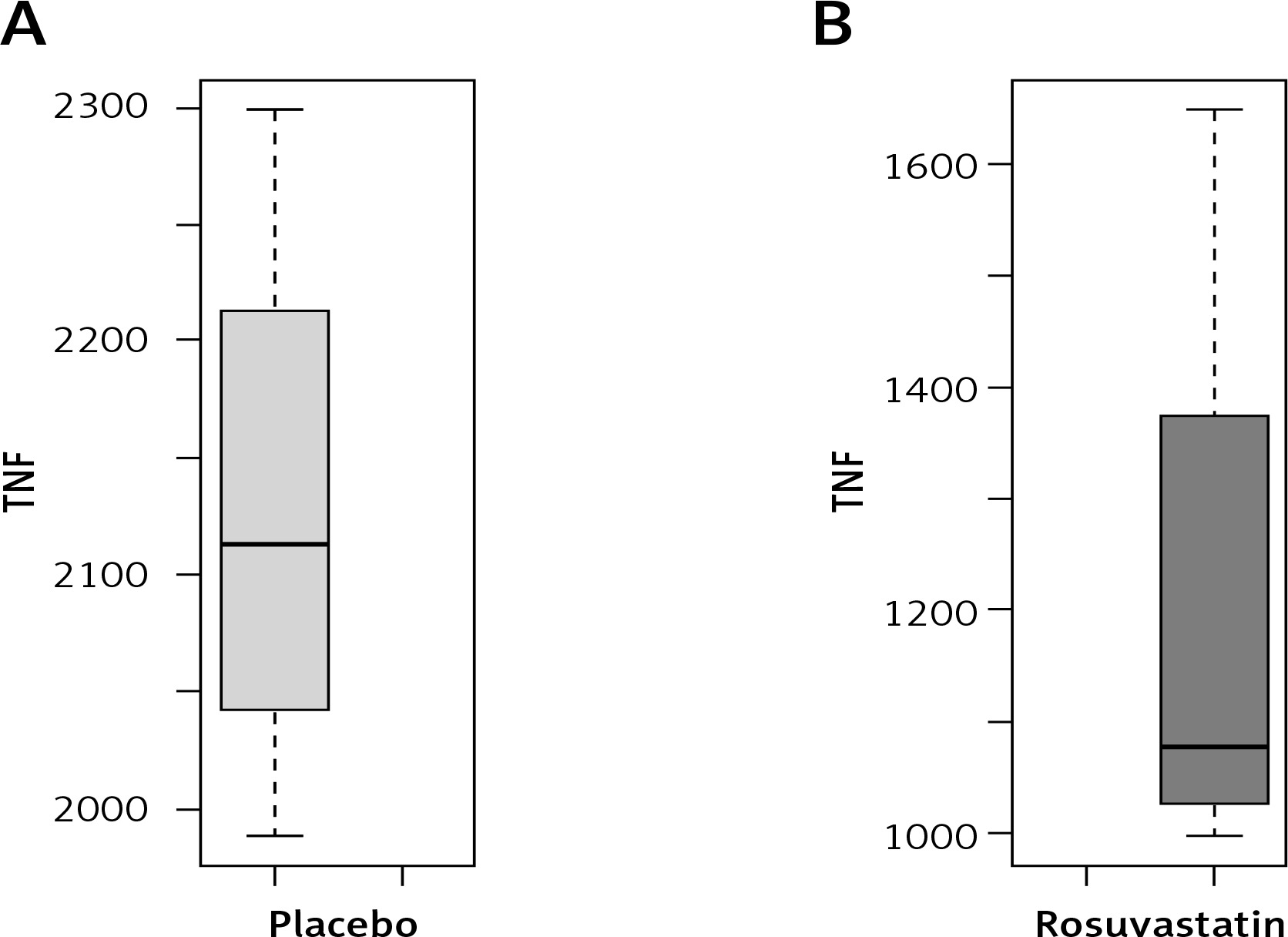
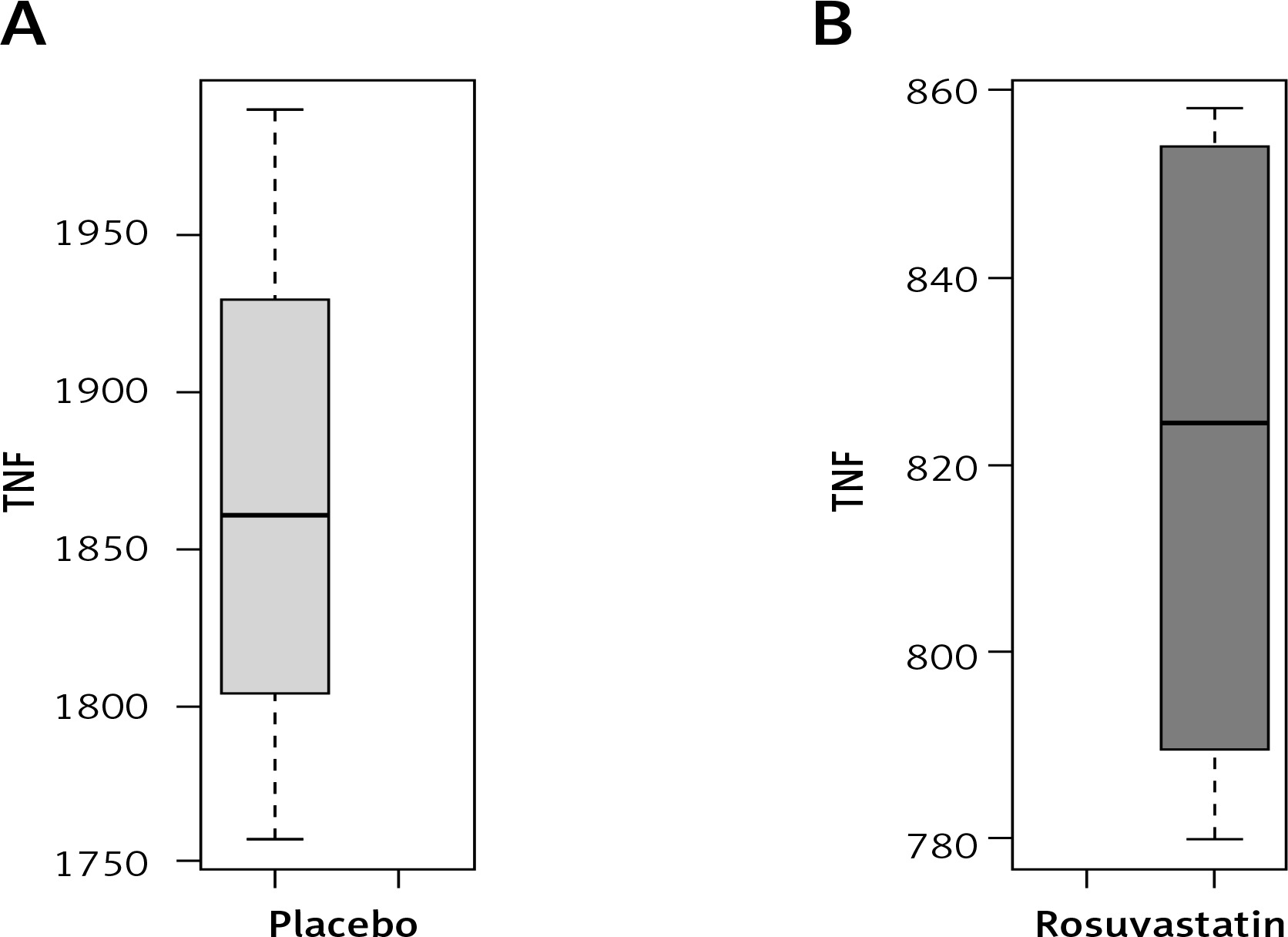
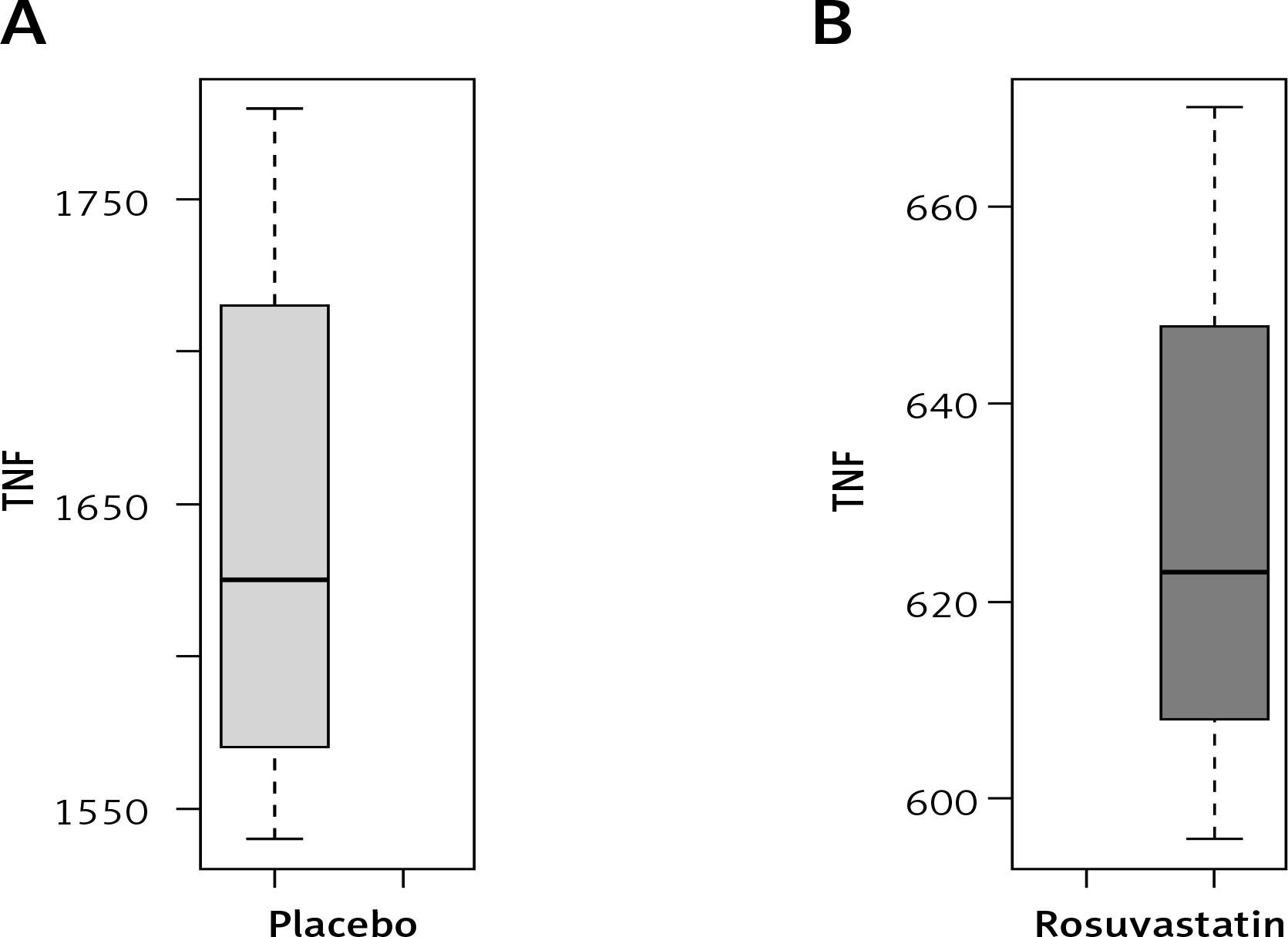
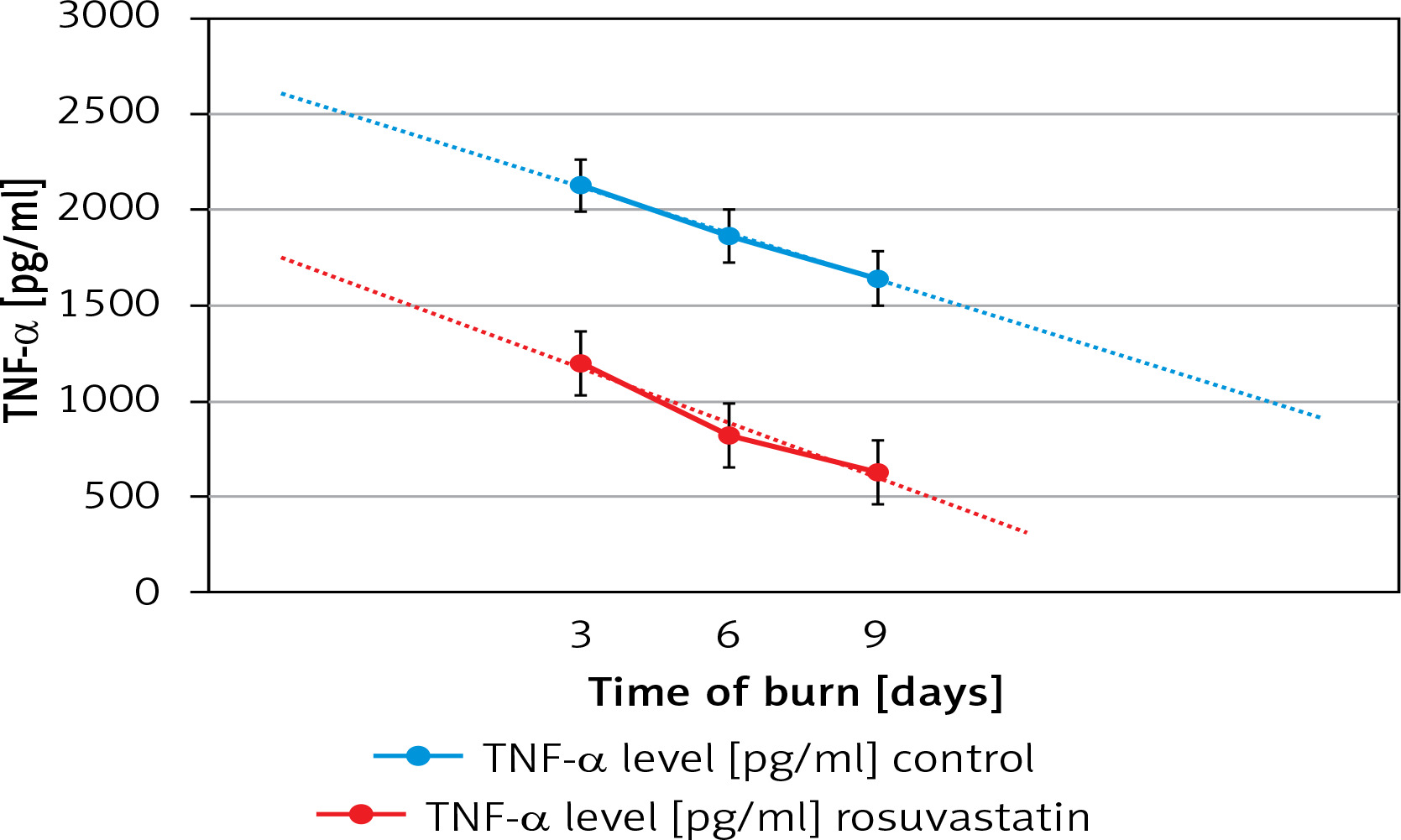
Burn-injured mice showed significant increases in TNF-α levels in the plasma. Both rosuvastatin- and placebo-treated rats showed maximum levels of TNF-α on the 3rd post-burn day and both groups demonstrated a decrease of the above-mentioned levels on the 6th and 9th post-trauma days. However, we observed reduced expression of TNF-α in all rosuvastatin-treated rats on days 3, 6, and 9 compared to the placebo group (p < 0.05) (Tables I–VI).
Table I
Summary measures for TNF-α levels in study group – 3rd day
| Measure of central tendency | Measure of variation |
|---|---|
| Mean = 1201 | IQR = 195 |
| Median = 1079 | Standard deviation =302.36 |
Table II
Summary measures for TNF-α levels in placebo group – 3rd day
| Measure of central tendency | Measure of variation |
|---|---|
| Mean = 2128 | IQR = 97 |
| Median = 2112.5 | Standard deviation = 129.4321 |
Table III
Summary measures for TNF-α levels in study group – 6th day
| Measure of central tendency | Measure of variation |
|---|---|
| Mean = 821.75 | IQR = 57.75 |
| Median = 824.5 | Standard deviation = 38.17831 |
Table IV
Summary measures for TNF-α levels in placebo group – 6th day
| Measure of central tendency | Measure of variation |
|---|---|
| Mean = 1866.75 | IQR = 73.25 |
| Median = 1860 | Standard deviation = 95.78927 |
Table V
Summary measures for TNF-α levels in study group – 9th day
| Measure of central tendency | Measure of variation |
|---|---|
| Mean = 628 | IQR = 23 |
| Median = 623 | Standard deviation = 30.8545 |
Table VI
Summary measures for TNF-α levels in placebo group – 9th day
| Measure of central tendency | Measure of variation |
|---|---|
| Mean = 1642.5 | IQR = 97.5 |
| Median = 1625 | Standard deviation = 102.1029 |
Based on our statistical analysis, as regards the variable of TNF-α levels of the 3rd, 6th, and 9th-day levels, we can state that:
The shape of histograms looks like a bell, the Q-Q plot is linear and the boxplot is symmetrical.
The mean, median, and mode are proximal to each other.
Consequently, we concluded that the TNF-α levels of the placebo and study group are normally distributed. The Shapiro-Wilk test was performed. According to the Shapiro-Wilk normality test, p-value > 0.05 for the 3rd, 6th, and 9th days of both placebo- and rosuvastatin-treated groups. Since the p-value is larger than 0.05, the TNF-α levels are normally distributed.
Association between TNF-α levels in placebo- and rosuvastatin-treated group
To describe the basic characteristics of the two groups, we investigated the measures of central tendency and variability (Table VII).
Table VII
Summary measures of TNF-α levels in placebo- and rosuvastatin-treated rats
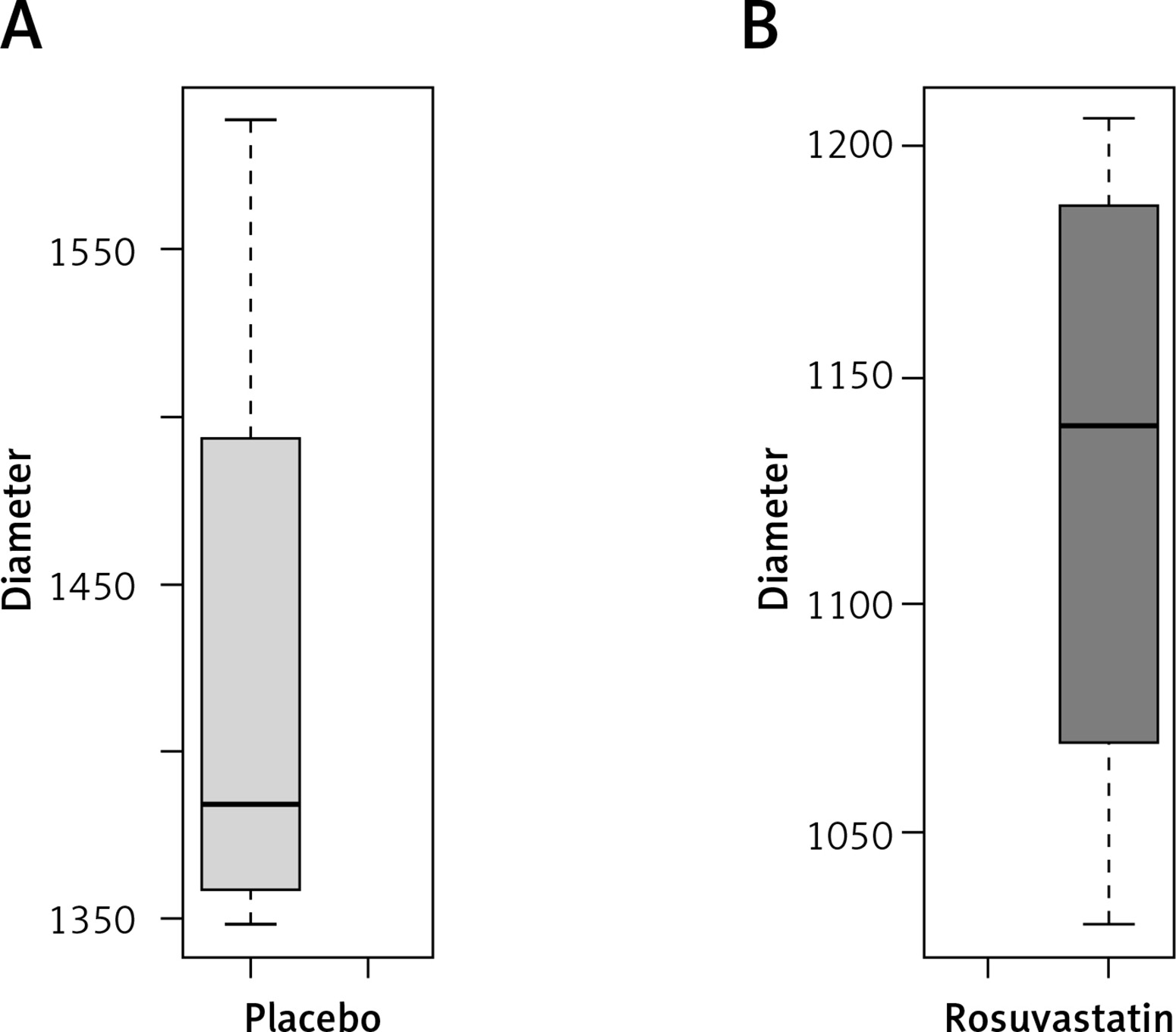
Graphical assessment
The tests of normality suggest that the data for TNF-α levels in placebo- and rosuvastatin-treated groups are normally distributed (p > 0.05). If we combine the data extracted from graphs, measures of central tendency, and normality tests, the overall decision is in favor of normality for TNF-α levels (Figures 4–6).
We performed Levene’s test in order to determine whether the variance is homogeneous between rosuvastatin and placebo-treated rats. We tested our null hypothesis through a two-sample test. The p-value was lower than 0.05. Consequently, there was a statistically significant difference in mean TNF-α levels between the two groups, on the 3rd, 6th, and 9th day.
Based on Figure 7, burn-wounded rats expressed significant increases in serum TNF-α levels. We can also note that TNF-α serum levels rise after the first post-burn hours and approach their maximum values on the third day and their minimum on day 9, not only for the study but for control groups as well. Moreover, the curve that represents each group seems to be similar. However, the concentration of TNF-α is statistically significantly different (p < 0.05) between rosuvastatin- and non-rosuvastatin-treated rats, concerning all post-wound studied points.
Procalcitonin
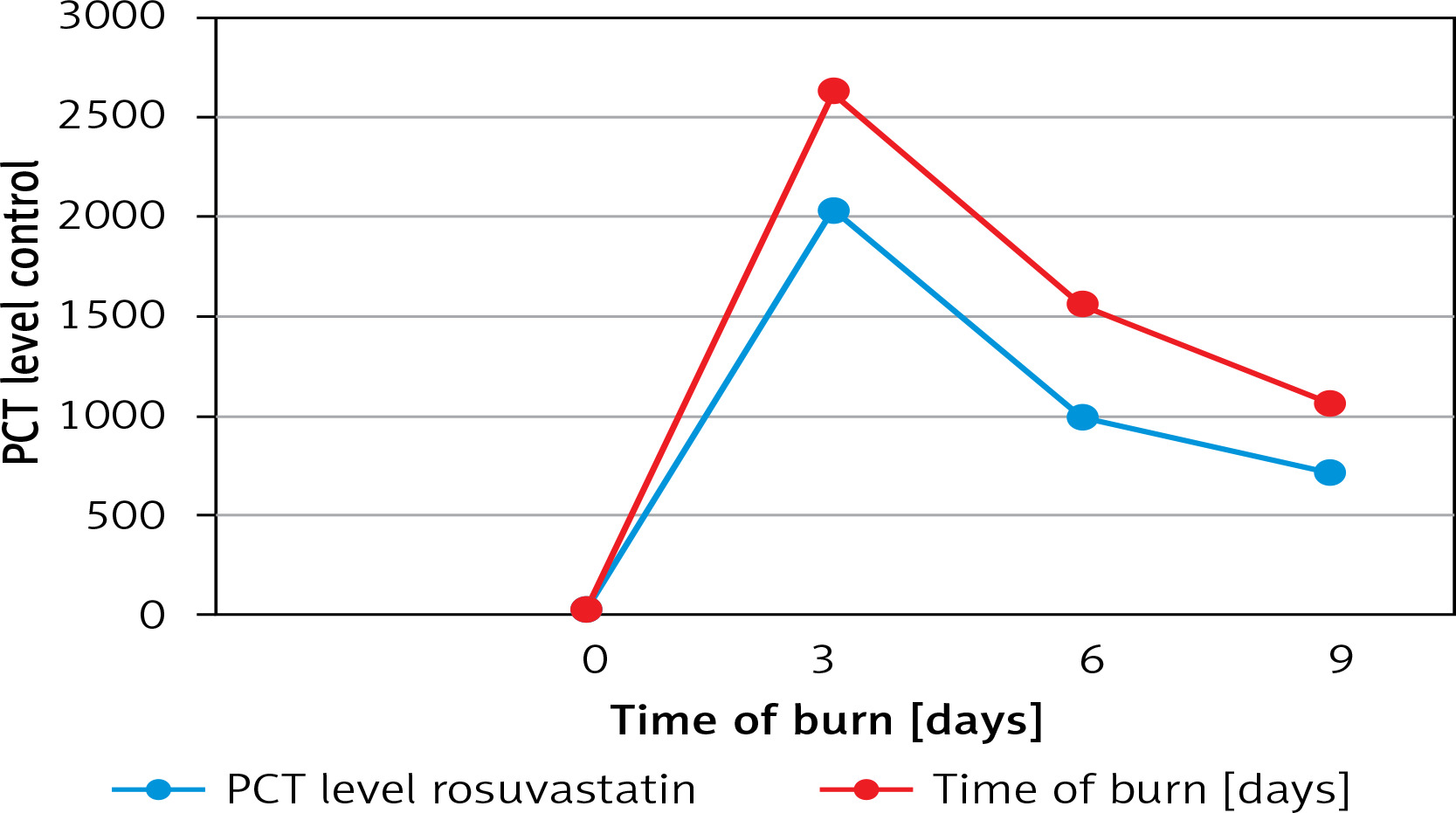
The mean values of PCT serum levels are presented in Figure 8. Based on our figure, we can note that mean PCT serum levels are increased after the first post-traumatic hours and reach their maximum levels on day 3 and the minimum on day 9, for both the control and study group. These levels are statistically significantly different between the day of the burn (day 0: day of burn removal) and the 3rd day in the two groups. When PG and SG are compared, it appears that both treated animals follow a similar curve. However, there is a statistically significant difference in the concentration of PCT (pg/ml) between the two groups not only on day 3 but also on days 6 and 9.
Macroscopic assessment – planimetry
Rosuvastatin accelerates wound healing
Based on our statistical analysis, to define the main characteristics of the two groups we have to investigate the measures of central tendency and variability (Table VIII).
Table VIII
Summary measures of wound size (mm) in placebo- and rosuvastatin-treated rats
Graphical assessment
As we described before, the tests of normality we performed suggest that the data for the wound size in placebo- and rosuvastatin-treated groups are normally distributed (p > 0.05). Combining the information extracted from graphs, mean-median, and normality tests, the overall decision is in favor of normality for macroscopic assessment (Figures 9–11).
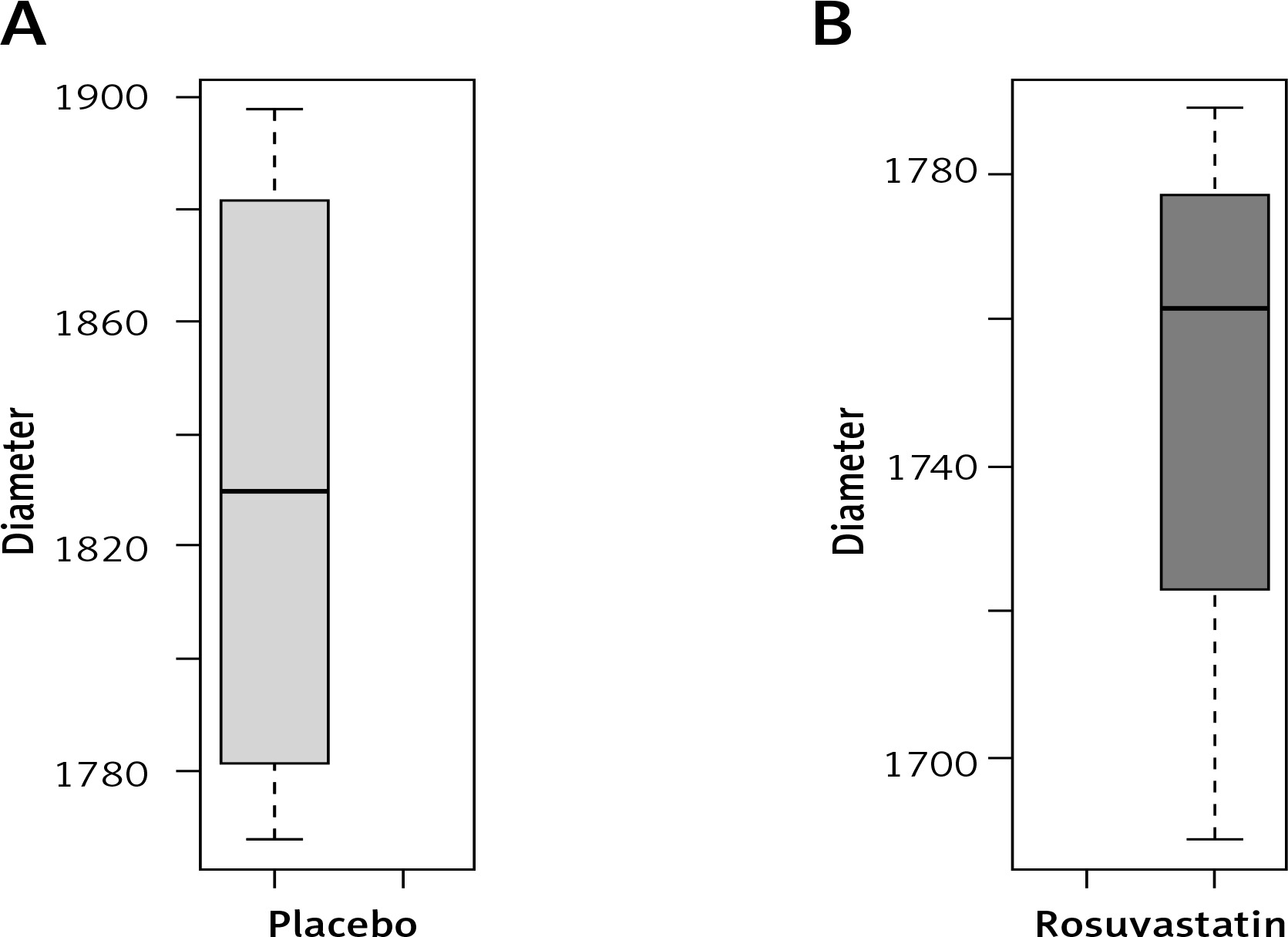
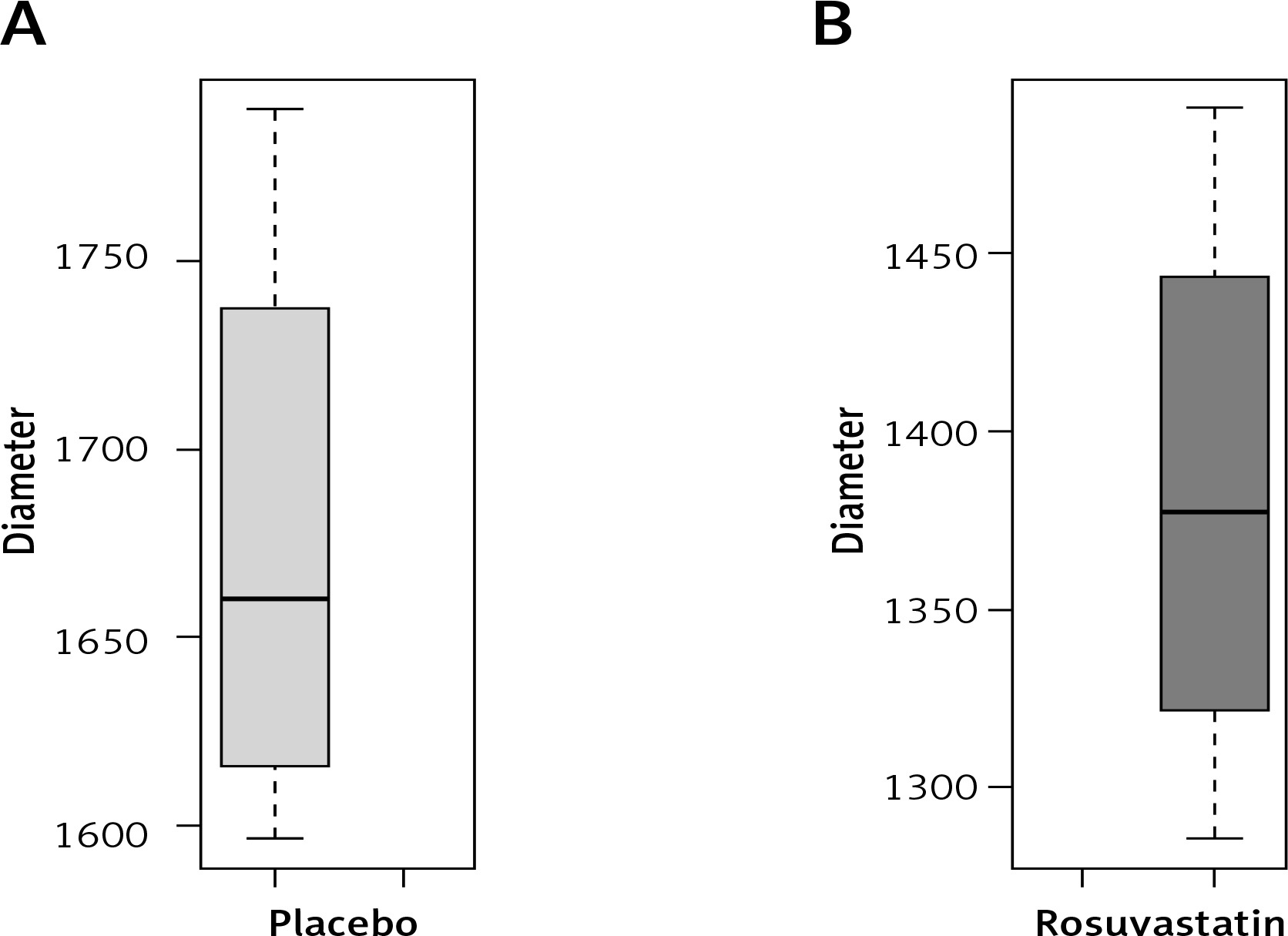
We performed Levene’s test in order to determine whether there is homogeneity of variance between the two groups, and finally we tested our null hypothesis through a two-sample t-test. The p-value was lower than 0.05. Consequently, there was a statistically significant difference in mean diameter between the two groups, on the 6th and 9th day.
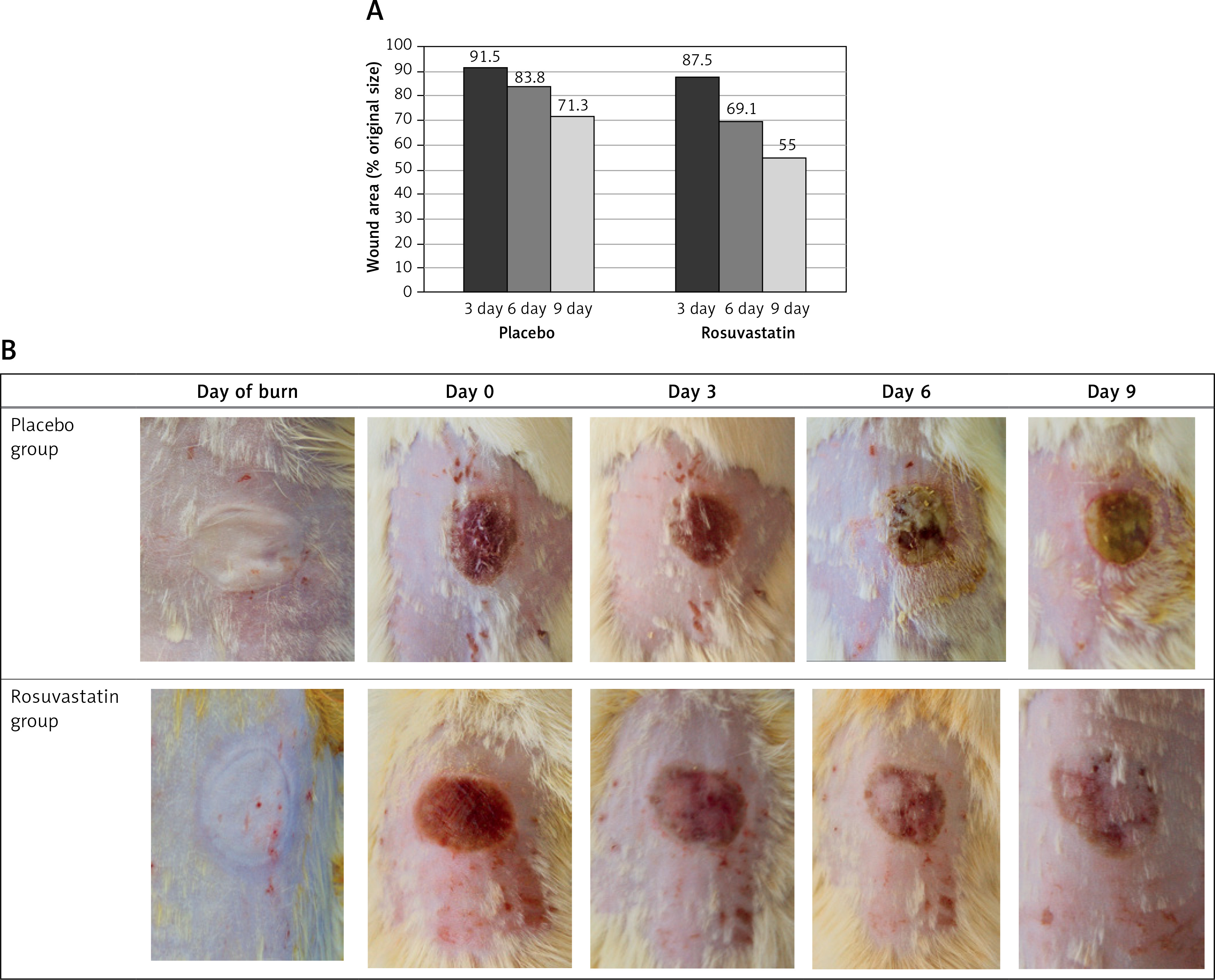
All the burn lesions were photographed and then macroscopically evaluated. Changes in wound diameter until the 9th day are expressed as a percentage of the initial burn area. Wound healing rate = [burn area (day X)/burn area (day 0)] × 100, planimetry method.
On day 3, rosuvastatin-treated groups presented almost 12.5% wound closure, whereas placebo-treated rats presented 8.5%, with no statistically significant difference. Rosuvastatin treatment resulted in significant differences in epithelization after day 6. Precisely, for placebo and rosuvastatin groups, 16.2% and 30.9% tissue repair was noted on day 6, and 28.7% and 45% on day 9, respectively (Figure 12).
Histopathological assessments
According to the Table IX, on the 3rd day, the average neutrophil infiltration was lower in the rosuvastatin group (average 40.5) than the placebo group (average 60). Moreover, as regards fibroblast proliferation, angiogenesis and re-epithelization, rosuvastatin-treated rats demonstrated higher levels, which led to up-regulation of the above-mentioned processes. Furthermore, on days 6 and 9, we can note that rosuvastatin stimulated both angiogenesis and re-epithelization.
Table IX
Summary of average levels of subepithelial neutrophils, fibroblast proliferation, angiogenesis, and re-epithelization on days 3, 6 and 9 for placebo and rosuvastatin groups
Discussion
Statins: mechanism of action
Cutaneous wound healing is a dynamic biological process, which involves the phases of inflammation, proliferation, and remodeling. Treatments that accelerate the skin repair procedure seem to be strong therapeutic weapons. Statins, primarily known for their hypolipidemic effects, exert their main pharmacological action by inhibiting 3-hydroxy-3-menthyl glutarate coenzyme A (HMG-CoA) reductase, a pivotal enzyme in cholesterol biosynthesis [27]. This inhibition reduces endogenous cholesterol synthesis in the liver, leading to increased expression of LDL receptors, enhanced circulation of LDL cholesterol, and subsequent lipid-lowering effects [28]. Beyond their hypolipidemic properties, statins exhibit pleiotropic actions [29], including antithrombotic effects, improvement of endothelial function, antioxidant properties, immunomodulation, and impact on various physiological systems such as the central nervous system, glucose metabolism, bones, and kidneys [28, 30–32]. These pleiotropic effects are thought to be lipid-independent and contribute to the broader therapeutic benefits of statins in addition to cholesterol reduction.
One of the significant pleiotropic effects of statins is their anti-inflammatory action. They reduce the expression of adhesion molecules [33], inhibit the binding of inflammatory cells to the endothelium, and decrease the secretion of pro-inflammatory cytokines IL-6, IL-1b, TNF-α, IL-8 and MCP-1 [34]. Additionally, they reduce C-reactive protein (CRP) levels, suppress Th17-mediated neutrophilic inflammation and inhibit macrophage and T cell activation [35]. Statins also affect the isoprenylation of proteins, including Rho, Ras, and Rac proteins, which play crucial roles in cell signaling pathways [36]. By inhibiting the isoprenylation process, statins disrupt important transduction pathways, influencing the concentration of adhesion molecules on endothelial cell surfaces. Additionally, statins reduce the transcriptional activity of NF-κB in inflammatory cells, suppressing the expression of cytokines and adhesives [37]. This anti-inflammatory effect extends beyond the vascular level, impacting systemic inflammation by lowering CRP levels [38].
Pleiotropic effects of statins on burn-wound healing
Based on statins’ anti-inflammatory effects, studies indicate that topical application of simvastatin enhances angiogenesis and collagen deposition, contributing to the amelioration of second-degree burn wounds [39]. Combining simvastatin with bone marrow mesenchymal stromal cells (BMSCs) further promotes healing by positively influencing angiogenesis through the SDF-1α/CXCR4 pathway, showing improvements in wound closure percentage, epithelial thickness, collagen remodeling, and up-regulation of relevant biomarkers [40]. Additionally, the use of a self-nanoemulsion drug delivery system incorporating coconut oil loaded with simvastatin demonstrates synergistic benefits in managing burn wounds, emphasizing reduced wound diameter, decreased IL-6 levels, and intensified antimicrobial effects [41]. Furthermore, research on mice suggests that simvastatin protects against liver damage in burn injuries by inhibiting the TNF-α signaling pathway [42].
In another line of investigation, atorvastatin has been explored for its lipophilic characteristics and tissue diffusion capacity. Administration of atorvastatin during hospitalization for burn injuries demonstrated safety, with no adverse events or notable laboratory abnormalities reported [43]. Moreover, in a porcine burn model, atorvastatin administration exhibited enhanced graft take, demonstrating improved re-epithelialization of full-thickness burns, reduced inflammation, enhanced vascularization, and accelerated resolution of myofibroblasts [44].
Another study investigated the effect of atorvastatin on tissue repair in mice following skin trauma to the spine. In this study, administration of atorvastatin led to a decrease in the expression of IL-6 and TNF-α, thereby contributing to the faster wound healing [45]. Further data demonstrated that administration of pravastatin for wound healing in Sprague Dawley diabetic mice enhanced wound stability, hydroxyproline accumulation, and expression of endothelial nitric oxide synthase [46]. In a similar study, low-dose, pre-traumatic oral therapy with simvastatin increased angiogenesis, reduced inflammation, and improved wound healing in diabetic mice [47]. Simvastatin is, perhaps, the only statin whose role has been investigated in the healing of burn injuries, and studies have shown some positive effects.
Interestingly, a study involving the administration of simvastatin to mice demonstrated notable enhancement in the viability of free flaps by exerting effective anti-inflammatory, vasodilatory, and anticoagulant effects and by increasing the expression of endothelial thrombomodulin in the flap zone, which is also a zone of marginal viability [48]. These findings underscore the potential of statins, such as simvastatin and atorvastatin, as therapeutic agents for promoting burn wound healing through various mechanisms, including angiogenesis, anti-inflammatory effects, and tissue regeneration.
Rosuvastatin
Rosuvastatin, a synthetic hydrophilic statin, stands out within its class due to its exceptional pharmacokinetic and pharmacodynamic characteristics. It boasts the longest half-life among statins, attributed to its molecular structure allowing effective binding to HMG-CoA reductase, resulting in potent enzyme inhibition at lower doses [49]. The statin’s liver selectivity minimizes bioavailability to non-hepatic tissues, reducing the risk of myotoxicity. Its metabolism, primarily by the 2C9 enzyme with minimal involvement of 3A4, contributes to fewer drug interactions involving cytochrome P450 [50].
The hydrophilic nature of rosuvastatin, in combination with the aforementioned selectivity of this statin to hepatocytes, results in its passive diffusion through the cell membranes being minimal, and it is almost completely absorbed by the liver [51]. As a result, the hypolipidemic effect of this statin is superior to that of simvastatin and pravastatin [52, 53].
Despite concerns about its pleiotropic effects in other tissues due to low uptake, studies affirm its pleiotropic actions, particularly through the inhibition of isoprenylation of Rho and Ras family proteins, critical for intracellular signal transmission. This inhibition results from the suppression of mevalonic acid synthesis, highlighting rosuvastatin’s multifaceted impact beyond cholesterol reduction [54].
Pleiotropic effects of rosuvastatin
The pleiotropic effects of rosuvastatin are increasingly evident, with growing evidence pointing towards its beneficial impact on various neurological and myocardial function outcomes. Precisely, Qiu et al. observed significant enhancement in 7-day survival with rosuvastatin treatment. During the post-cardiac arrest phase, rosuvastatin demonstrated the ability to promptly enhance and stabilize circulatory function while mitigating cerebral injury. This effect was linked to the reduction of apoptosis in both myocardial and neural tissues [55].
The increasing evidence of rosuvastatin’s effectiveness in neurological disorders, including epilepsy, Alzheimer’s, Parkinson’s, spinal cord injury, and cerebral ischemia, suggests its broad therapeutic potential. Rosuvastatin’s neuroprotective effects are likely attributed to its anti-inflammatory, antioxidant, and anti-apoptotic activities, as demonstrated in recent research studies [56].
Another study aimed to examine how rosuvastatin influences angiotensin-converting enzyme 2 (ACE2) during neointimal formation following vascular balloon injury in rats and proved that rosuvastatin’s ability to inhibit intimal thickening is associated with the elevation of ACE2, augmentation of Ang-(1-7), suppression of AT1, and activation of the P-ERK pathway [57].
Moreover, numerous viral pathogens contain components that undergo prenylation through the mammalian mevalonate pathway. In certain viral infections, rosuvastatin exhibits antiviral activity by inhibiting HMG-CoA reductase, thereby reducing the expression of prenylated proteins [58].
Boczar et al. attempted to assess both systemic markers and imaging indicators of inflammation in the ascending aorta, bone marrow, and spleen using 18F-FDG PET/CT in HIV-positive patients before and after rosuvastatin therapy. At baseline, HIV-positive patients exhibited significant markers of systemic inflammation, including monocyte activation, leading to the conclusion that treatment with a low dose of rosuvastatin in this HIV-positive cohort leads to a notable reduction in FDG uptake in the bone marrow, spleen, and thoracic aorta [59]. A study which led to a similar conclusion suggested that the lipid-lowering and anti-inflammatory properties of statins could potentially aid in preventing cardiovascular disease in individuals with human immunodeficiency virus (HIV) experiencing chronic inflammation, through elevation in proportions of CD16+ monocyte subsets [60].
Another investigation explored the impact of short-term administration of low- and high-dose rosuvastatin on the expression of ABCA1 and ABCG1 in human atherosclerotic plaques. Interestingly, high-dose rosuvastatin was found to elevate macrophage ABCA1 protein levels within atherosclerotic plaques, despite a decrease in mRNA, and this effect was unrelated to reductions in plasma cholesterol [61].
Finally, data indicated that the collective genetic potential of the gut microbiome to transport and metabolize metabolites along the phosphatidylcholine/carnitine-TMA-TMAO pathway was reduced in rosuvastatin-treated patients, with a corresponding increase of several metabolites in plasma. Consequently, these findings suggest that statins could have a clinically relevant impact on the gut microbiome [62].
Pleiotropic effects of rosuvastatin on wound healing
Experimental evidence suggests that rosuvastatin plays a significant role in wound healing by counteracting wound-healing inhibitors, such as farnesyl pyrophosphate (FPP), and enhancing endothelial and microvascular functions [63]. Additionally, it demonstrates antimicrobial properties against bacteria, including MRSA, and reduces inflammation by suppressing the expression of inflammatory cytokines [64]. Studies also highlight its potential in managing chronic periodontitis by improving the repair process through the suppression of associated inflammation [65]. Researchers have explored various delivery systems, such as nanocubic vesicles with silver particles and transethosomal formulations, to enhance rosuvastatin’s efficacy in wound management [66]. Despite challenges related to solubility and bioavailability, innovative approaches such as self-nanoemulsifying drug delivery systems (SNEDDS) and nanoemulsions are being investigated to overcome these constraints and improve the topical delivery of rosuvastatin for wound healing [67].
As we have mentioned, the existing support for the potential beneficial effects of rosuvastatin on wound healing primarily stems from animal studies, which are characterized by small sample sizes and relatively short observation periods. Additionally, the precise contribution of rosuvastatin in the context of burn wounds remains largely uninvestigated. Although the findings outlined above suggest that rosuvastatin may present a promising alternative for the treatment of burn wounds, it is crucial to note that further substantiation is required. In future, these outcomes necessitate validation through rigorous controlled clinical trials of high quality before any consideration for routine clinical application.
In our randomized prospective experimental study, we found that topical treatment of a partial-thickness burn with rosuvastatin ameliorates tissue repair. Through evaluation of the activity of rosuvastatin and procalcitonin levels in serum of burn-induced rats, we noted that the topical use of rosuvastatin reduced the above-mentioned levels. Specifically, topical rosuvastatin causes down-regulation of TNF-α and procalcitonin levels, modulates the inflammation process and improves burn outcomes.
In this experimental study we used 36 male rats that were randomly divided into two main groups. A partial-thickness burn trauma was induced on the back of the rats and 3rd, 6th and 9th post-burn days were examined. Half of the animals were treated with Eucerin cream and 50% with a mixture of Eucerin and rosuvastatin cream. Regarding our variables, we concluded that TNF-α, procalcitonin and wound size were normally distributed and we presented the mean and median values. Subsequently, we tried to identify the association between TNF-α and procalcitonin levels and the rate of wound closure on days 3, 6 and 9 for rosuvastatin and non-rosuvastatin treatment groups. Precisely, we proved that the data of TNF-α, procalcitonin and macroscopic assessment were normally distributed among the two groups on all studied days, and based on Student’s t-test we found that there was a statistically significant difference in mean TNF-α and procalcitonin on day 9 between the two groups. Concerning the rate of wound closure, a statistically significant difference was not found for day 3 between the two groups, whereas tissue repair showed significant differences for the other days, in favor of rosuvastatin-treated rats.
Strengths
The effect of rosuvastatin on partial-thickness burn trauma has not been studied previously. We believe the study is of particular interest since rosuvastatin, as a younger generation statin, is characterized by fewer side effects and increased activity. Hence, the study may be considered original because it is the first study investigating the effect of rosuvastatin on an experimental model of partial-thickness burn injury in rats. Moreover, in this study we included an updated summary of evidence on the pleiotropic effects of rosuvastatin and the impact of statins on wound repair. Our results are generally in line with the previous experimental studies. Further points of our study include a thorough literature search both of major electronic databases and of grey literature.
Limitations
Finally, some limitations have to be acknowledged. Although in vivo burn models offer a detailed understanding of pathophysiological processes correlated with burn wounds, the use of larger animals seems to be one of the main limitations due to ethical or financial barriers. Despite their popularity, rat burn models present some wound healing differences and show reduced tissue repair time compared to those of humans [68]. Hence, it needs to be explored whether the conclusions in rats can be extrapolated to human burn models. Moreover, despite our thorough literature search, we identified only a few eligible studies and no meta-analyses that correlate the anti-inflammatory activity of statins with burn injury. The overall sample size was limited, leading to wide confidence intervals in our summary results.
In conclusion, our experimental study proved that the use of rosuvastatin through topical application treatment can modulate certain aspects of the inflammatory cascade, leading to improved clinical burn outcomes. In the absence of adequate evidence, further evidence-based studies seem to be crucial. Data should be collected to thoroughly assess the most effective statin drug, the appropriate doses, and the administration choices. Moreover, the majority of disposable data that detect the potential beneficial effect of statins on skin tissue repair are based on animal-rat studies with limited overall sample sizes. Hence, large-scale clinical trials are needed to further prove the potential correlation of statins with an enhanced wound healing procedure. According to the World Health Organization (WHO), almost 265,000 deaths are caused by burns each year, most of which occur at home or in the workplace [69]. In addition, it is a global public health problem that affects people from all countries and of all ages. Nevertheless, the therapeutic landscape remains cloudy. Every day, new products are introduced to the market, aiming to heal the burn more effectively and esthetically. Focus is placed on the use of statins, which has a growing role in the treatment of burns and seems to be a promising, locally applicable, and low-cost solution [70]. Rosuvastatin is potential drug that, through topical application, is able to ameliorate tissue repair outcomes.