Introduction
Sarcoidosis is a multi-system granulomatous disorder of unknown cause. It is characterized by a wide spectrum of presentations, likely reflecting a complex and poorly understood interplay of genetic, ethnic, immunological, and environmental factors. In the United States, the prevalence of cardiac sarcoidosis (CS) among patients with systemic sarcoidosis ranges between 20% and 27%, but this prevalence can reach up to 58% among Japanese patients [1–4]. Sarcoidosis affects myocardial tissue by causing inflammatory cell infiltration, granuloma formation, and fibrosis, which manifest as complete atrioventricular block, ventricular arrhythmias, congestive heart failure, and sudden cardiac death [5, 6]. Corticosteroid treatment has shown greater benefits for long-term outcomes in patients with higher left ventricular ejection fraction (LVEF) compared to those with lower LVEF, suggesting that timely therapeutic intervention after identifying cardiac involvement may improve prognosis [7–10].
In patients with isolated cardiac sarcoidosis (ICS), cardiac manifestations of sarcoid appear first without apparent evidence of extracardiac involvement [11]. The diagnosis of ICS typically requires histological confirmation through an endomyocardial biopsy (EMB). However, given that the sensitivity of EMB for detecting CS is only around 20% [12], the diagnosis of ICS can be particularly challenging. The Japanese Circulation Society (JCS) introduced the first diagnostic guidelines for ICS [13]. The detection of non-caseating granulomas in myocardial tissue in patients who show no clinical signs of sarcoidosis in other organs is necessary to diagnose ICS. If EMB is not possible or granulomas are not detected, patients can still be diagnosed with ICS if gallium-67 scintigraphy or 18F-FDG positron emission tomography reveals abnormally high tracer accumulation in the heart and at least three of the remaining four major criteria for cardiac involvement are met. By contrast, the 2014 expert consensus statement from the Heart Rhythm Society [14] does not delineate ICS as a specific diagnostic category.
A number of cohort- or registry-based studies have reported on the differences between the clinical characteristics and outcomes of patients with ICS compared to patients with non-ICS or systemic CS (SCS). The emerging evidence generally points to more severe clinical course, with increased risks of arrhythmias and more severe cardiomyopathy in ICS patients [15], although long-term outcomes may be similar between the two groups [16]. In the present systematic review and meta-analysis, data from published literature were pooled to enhance the statistical power and provide a balanced insight regarding any potential differences in outcomes between ICS and SCS patients.
Methods
This systematic review and meta-analysis followed the guidelines established by the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [17].
Data sources and search strategy
Two researchers (AA and MA) independently searched PubMed/Medline, Embase, and the Cochrane Library from their inception until August 2024. The researchers manually examined references of retrieved studies and reviews to ensure that all relevant articles were included. The search strategy used the following keywords and Medical Subject Headings (MeSH) terms: “isolated cardiac sarcoidosis” OR “isolated CS” OR “primary cardiac sarcoidosis” AND “systemic cardiac sarcoidosis” OR “systemic CS” OR “secondary cardiac sarcoidosis” OR ‘’extra-cardiac sarcoidosis’’. Additionally, reference lists of relevant articles were manually screened to identify any further studies that met the inclusion criteria.
Supplementary Table SI provides detailed search strategies for each database.
Eligibility criteria and outcomes
Studies were considered eligible for inclusion in our systematic review and meta-analysis if they: (i) were observational studies (cohort, case-control, and cross-sectional studies); (ii) included patients diagnosed with cardiac sarcoidosis, with subgroups of ICS and SCS; (iii) defined ICS as cases where granulomatous inflammation is confined to the heart, with no clinical, radiological, or histological evidence of sarcoidosis in other organs; (iv) defined systemic CS as cases where cardiac involvement was diagnosed in the context of multi-organ sarcoidosis or sarcoidosis had been detected in at least one other organ system, confirmed by biopsy (e.g., lung, lymph nodes) or by clinical and radiological evidence; and (v) reported on prognostic and clinical outcomes (e.g., MACE, arrhythmias, cardiac death, and heart failure hospitalization).
Studies were excluded if they: (i) did not provide data on both the ICS and SCS cohorts; (ii) had insufficient data on outcomes or prognosis for both the groups; and (iii) were case reports, letters, editorials, conference abstracts, or reviews.
The primary outcome was a composite of MACE, including cardiac death, ventricular arrhythmias, or hospitalization for heart failure. The definition of composite outcome in different studies is given in Supplementary Table SI. The secondary outcomes included sudden cardiac death, arrhythmias, and heart-failure-related hospitalizations. The data for outcomes were extracted for the longest available follow-up.
Study selection and data extraction
The studies obtained from the literature search were imported to EndNote X9 (Clarivate Analytics), and duplicate records were removed. Two authors (MA and AA) independently reviewed the retrieved studies based on titles and abstracts. This was followed by a review of the full texts of the articles. A third author (RA) was consulted in the event of any disagreements.
The following data were retrieved from each eligible study: author’s name, year of publication, country, sample size, definition of composite outcome, duration of follow-up, age of patients, proportion of females/males, NYHA class III or IV, LVEF %, comorbidities such as CAD, device implantation, and medical therapy including ACEIs and β-blockers. A pre-piloted Excel sheet was used for data extraction.
Quality assessment of the included studies
The quality assessment of the observational studies was performed using the Cochrane Risk of Bias in Nonrandomized Studies – of Interventions (ROBINS-I) tool [18]. The ROBINS-I tool uses seven domains to determine overall bias in each non-randomized clinical trial. The risk of bias was assessed in 7 different domains (confounding, selection, intervention classification, deviation from intervention, missing data, measurement of outcome, selection of reported results). Studies were classified as having low, moderate, or serious risk of bias. Studies that had information missing in one or more domains were classified as NI (no information). Risk-of-bias plots were created using the Robvis tool [19].
Statistical analysis
The meta-analysis was conducted using R version 4.4.1 with the application of the “meta” and “metasens” packages via RStudio. The risk ratios (RRs) with 95% confidence intervals (CIs) were calculated using the Mantel-Haenszel method in a random effects model, which was presented in forest plots [20]. The Paule-Mandel procedure was used to estimate χ2, the heterogeneity variance21. Heterogeneity was assessed using the Higgins I2 statistic: values of 0% to 40%, low heterogeneity; 30% to 60%, moderate heterogeneity; 50% to 90%, substantial heterogeneity; 75% to 100%, considerable heterogeneity [21, 22]. Egger’s test was not employed to quantify the asymmetry, nor were funnel plots generated, given the insufficient number of included studies [23]. A p-value of < 0.05 was considered significant.
Results
The literature search identified 393 eligible records. After the removal of duplicates, primary screening was performed using study titles and abstracts. The full texts of 37 studies were retrieved and 7 studies met the pre-determined inclusion criteria (Supplementary Figure S1). The statistical synthesis of data involved 5 studies. Maeda et al. conducted a registry-based study that included data from Japanese CS patients treated at several university hospitals nationwide [16]. Several Japanese studies reporting on outcomes of CS patients from individual centers were also included [24–28]. Although we included all these studies due to their reporting of different outcomes, we ensured that data for overlapping patient populations (i.e. from Maeda et al. and the other Japanese studies) were not pooled for the same outcomes to prevent overestimation of the pooled effect sizes.
The included studies [16, 24–29] reported data for 918 CS patients. 265 patients had ICS while 653 patients were diagnosed with SCS. The mean follow-up duration was 4.34 years (40.1 months). The patients with ICS had a mean age of 61.2 years (SD: ±12.1), whereas those with SCS had a mean age of 61.9 years (SD: ±11.2). Details of the study characteristics and baseline data are provided in Table I.
Table I
Baseline characteristics of patients in included studies
The bias assessment of included studies showed some concerns in 4 studies, mainly related to confounding bias and intervention classification (Supplementary Figures S2, S3).
Results of meta-analysis
Composite outcome
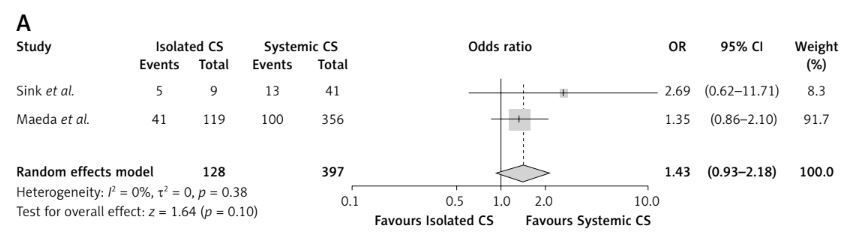
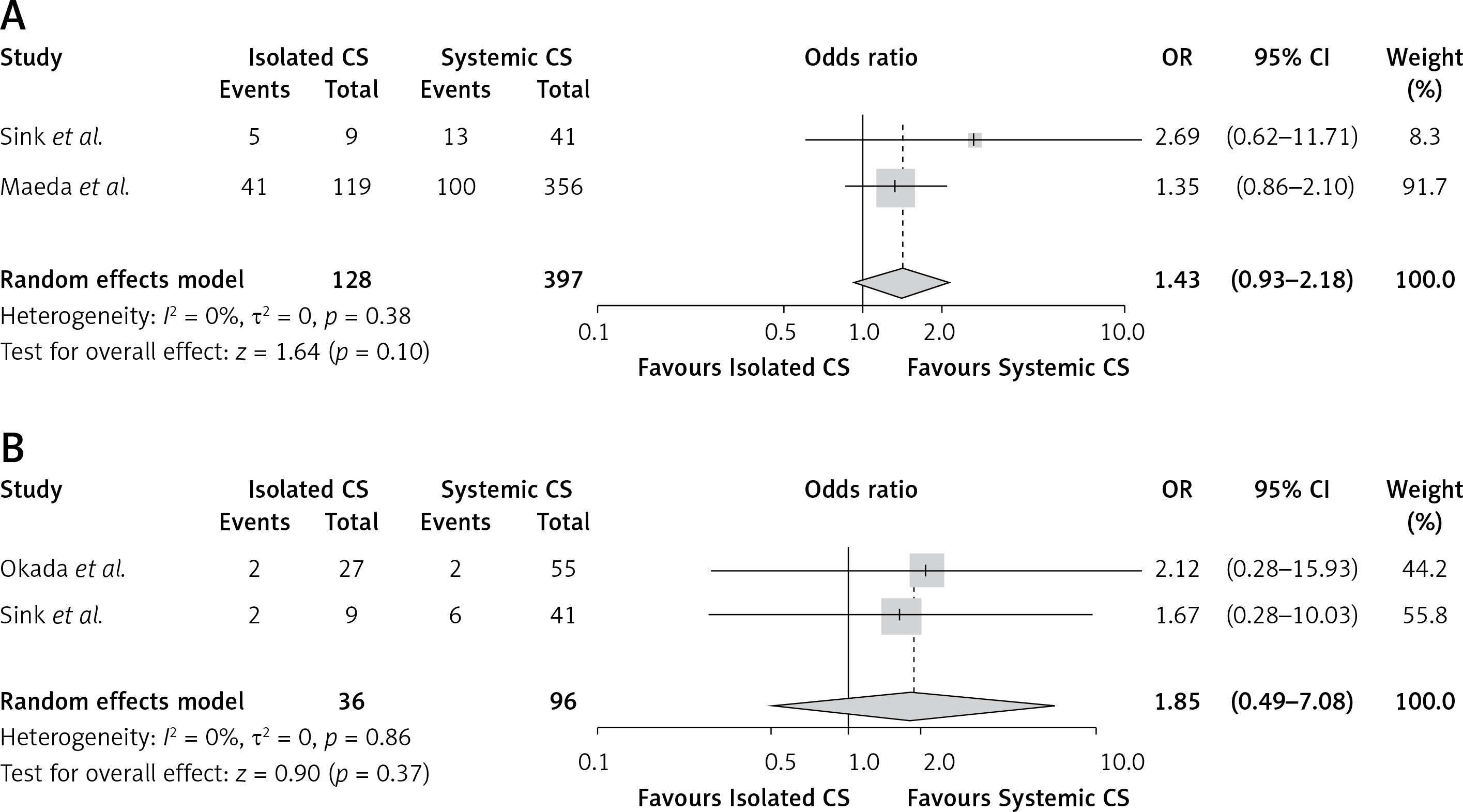
The pooled analysis demonstrated a nonsignificant difference between ICS and SCS for the risk of composite outcome (RR = 1.43, 95% CI: 0.93 to 2.18, p = 0.10, Figure 1 A) compared to SCS. No heterogeneity was observed (I2 = 0%).
Cardiac death
No statistically significant association was observed for cardiac death (RR = 1.85, 95% CI: 0.49 to 7.08, p = 0.37, I2 = 0%, Figure 1 B) between ICS and SCS. Tezuka et al. did not report absolute numbers for deaths in each group; however, the Kaplan-Meier curve indicated a nonsignificant difference in survival between patients with isolated and systemic CS [26].
HF-related hospitalizations
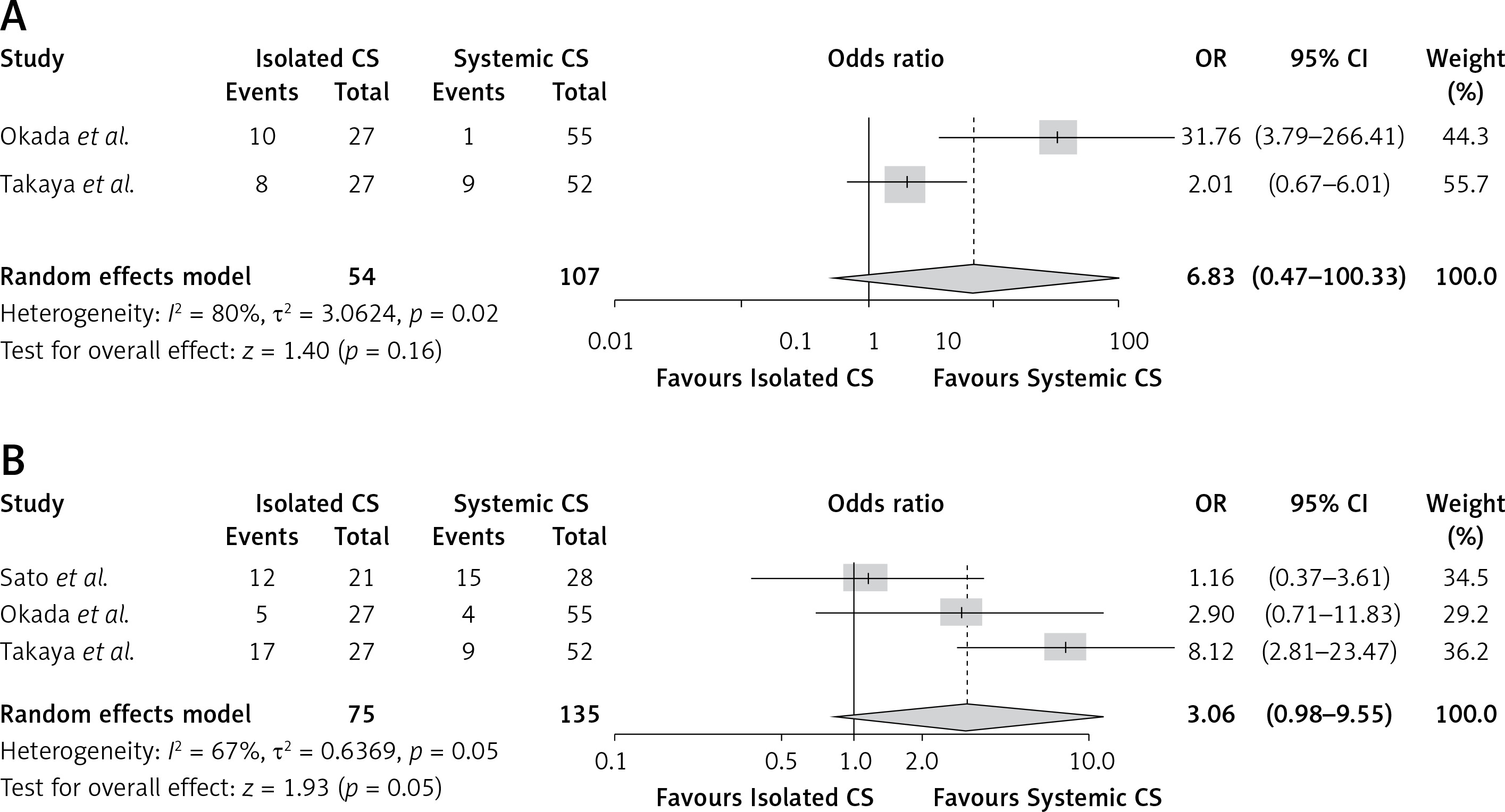
The pooled analysis demonstrated a non-significant difference between ICS and SCS for the risk of HF-related hospitalizations (RR = 6.83, 95% CI: 0.47 to 100.33, p = 0.16, Figure 2 A). Heterogeneity was high (I2 = 80%), and did not decrease on performing sensitivity analysis. Kaneko et al. reported comparable rates of death, HF-related hospitalizations, and arrhythmias across two groups [27].
Arrhythmias
The pooled analysis demonstrated elevated risk of arrhythmias among patients with ICS (RR = 3.06, 95% CI: 0.98 to 9.55, p = 0.05, Figure 2 B) compared to SCS, although it did not reach statistical significance. Heterogeneity was moderate (I2 = 67%).
Discussion
The present systematic review and meta-analysis synthesized data from 918 patients from 7 articles. The salient findings can be summarized as follows: (1) Compared to SCS patients, the cohort of ICS patients had poorer baseline LVEF and demonstrated a higher prevalence of implantable cardiac devices. (2) ICS patients were more likely to present with serious cardiac manifestations, such as ventricular arrhythmias. (3) Despite this, there was no significant difference in the rates of composite outcome, cardiac mortality, or HF-related hospitalizations between ICS and SCS patients.
Cardiac involvement in sarcoidosis, whether in the context of ICS or SCS, is increasingly recognized, but the evidence for the influence of the pattern of organ involvement on outcomes can be conflicting. This discrepancy may stem from factors distinct from the condition itself, such as variations in diagnostic criteria, treatment strategies and follow-up periods, which complicate interpretation of prognostic data. Manifestations of CS range from clinically quiescent myocardial granulomas to symptomatic arrhythmias, progressive heart failure and sudden cardiac death [30]. Presentation patterns vary widely due to factors such as prior medical treatment, presence of ICS and biopsy confirmation [30–32]. While the mean age at diagnosis for patients with extra-cardiac sarcoidosis is 40–50 years [2], CS patients seem to be diagnosed mostly in their fifth or sixth decades of life, as observed in this analysis. There is increasing recognition that CS patients experience diagnostic delays [29], which have been hypothesized to originate from the non-specificity of early symptoms and challenges in accessing appropriate diagnostic tools (endomyocardial biopsy or advanced cardiac imaging) [29, 33]. A few other factors could also contribute to this observation. Firstly, CS patients may have had immunosuppressive treatment for extra-cardiac sarcoidosis at a stage when cardiac involvement was less significant, thereby delaying the conversion from clinically silent to clinically manifest CS [10, 34]. Secondly, as observed in the present study, ICS patients are more likely to present with malignant ventricular arrhythmias. Other studies have demonstrated higher incidence of atrioventricular block in CS patients [35]. The management of these complications with symptomatic treatment, such as anti-arrhythmics or device implantation, can supersede full investigation into the underlying cause, further delaying the identification of ICS until more severe cardiac dysfunction or heart failure develops. In several cases, patients may be misdiagnosed with idiopathic or non-ischemic dilated cardiomyopathy and pursue treatment to the point of heart transplantation, with the correct diagnosis of CS only becoming apparent after examination of the explanted hearts [36, 37].
ICS patients were more likely to demonstrate impaired LVEF, which correlates with an increased risk of ventricular arrhythmias. This observation echoes the finding of a large prospective international cohort study from the Cardiac Sarcoidosis Consortium investigating arrhythmia burden and outcomes of CS patients [38]. The authors noted that the most common arrhythmias experienced by CS patients with reduced LVEF are ventricular arrhythmias, which were also associated with higher risks of adverse events. In a study characterizing the ventricular substrate and electrophysiological mechanism in CS patients who developed VT, the main driver was found to be re-entry circuits around confluent regions of endo- and epicardial ventricular scarring, especially in the right ventricle [39]. Cardiac magnetic resonance imaging (CMR), using T1 and T2 mapping techniques, provides a detailed assessment of myocardial edema and inflammation [40]. CMR also provides an assessment of late gadolinium enhancement (LGE), which serves as a marker of myocardial fibrosis in CS patients [41]. Risk-stratifying CS patients based on LGE has therefore been proposed, based on the observation that the presence of LGE is associated with higher mortality rates, irrespective of LVEF [42, 43]. In the studies we analyzed, despite the higher risk of ventricular arrhythmias seen in ICS patients, there was no significant difference in LGE presence or distribution between ICS and SCS patients [24–27]. Myocardial inflammation, indicated by FDG uptake on cardiac positron emission tomography (PET), was similarly present in ICS and SCS patients except in studies by Kaneko et al. [27] and Okada et al. [25], which actually found higher prevalence of cardiac FDG uptake among SCS patients. This underscores the complexity of ventricular arrhythmogenesis in CS patients and highlights the significant influence of confounding factors, which renders research in this field particularly challenging.
It is tempting to attribute the lack of a significant difference in composite outcome and cardiac mortality between ICS and SCS patients to the prognostic equivalence of these diagnostic sub-categories. However, it is noteworthy that the analyzed studies reflect the detection rate of clinically manifest CS and do not account for subclinical cases or cases that are fatal at presentation. For example, in an autopsy study of sudden cardiac death in CS by Tavora et al., 83% of their ICS cases were diagnosed with sudden cardiac death attributable to CS [44]. By comparison, a smaller proportion of SCS cases (52%) had sudden cardiac death secondary to CS. Moreover, cardiac screening in patients with systemic sarcoidosis has significantly improved with advances in imaging techniques, more robust screening guidelines, and better risk stratification. Updated guidelines from the American Thoracic Society [45] and the European Respiratory Society [46] recommend comprehensive screening for all sarcoidosis patients. Lead time bias, which means that earlier disease detection leads to overestimation of event-free survival, is a distinct possibility. Finally, the treatment strategies for heart failure with impaired ejection fraction and secondary prevention of ventricular arrhythmias – the two main drivers of mortality in CS [47] – are likely to be largely similar in ICS and SCS patients. Combined with the similar response to immunosuppressive therapy in the burden of myocardial inflammation on imaging [16, 27] and NT-pro-BNP levels [26] between ICS and SCS patients, these factors could explain the comparable mortality rates.
Despite the overall robustness of the findings of the present meta-analysis, a few limitations have to be acknowledged. Firstly, the studies included were retrospective in nature, with well-recognized shortcomings inherent to this research design. Secondly, cardiac sarcoidosis is a heterogeneous condition, and the prognosis varies according to geography and ethnicity [48]. This might explain why heterogeneity was relatively high for some outcomes and leave-one-out sensitivity analysis did not consistently identify a single study contributing to this heterogeneity. It is likely that the effect of confounding factors, such as differences in patient populations, duration of follow-up, non-uniform reporting of data, or variations in treatment protocols, may have contributed to the variability observed.
In conclusion, cardiac involvement in sarcoidosis is a marker of poor outcomes and prognosis. However, evidence of whether characteristics and outcomes differed based on the pattern of organ involvement, i.e. ICS vs SCS, was conflicting. In this systematic review and meta-analysis, ICS patients were more likely to have poorer LVEF at baseline compared to SCS patients. This was associated with a higher risk of ventricular arrhythmias. Nevertheless, the rates of composite outcome and cardiac death were comparable between the two groups, indicating the possibility of equivalence of prognosis between these cohorts of patients.