Introduction
SARS-CoV-2, the virus responsible for coronavirus disease 2019 (COVID-19), primarily manifests as a respiratory illness; however, it can also affect the cardiovascular system. Previous studies have shown that cardiac involvement occurs in 20–40% of affected patients, while more recent research has reported a reduced incidence of approximately 5%, primarily indicated by elevated levels of hs-cTnI [1–3]. Although only a small proportion of patients experience acute heart failure with a reduced ejection fraction due to myocarditis [4, 5], higher hs-cTnI levels have been associated with an increased mortality rate [6]. Numerous mechanisms have been proposed to explain the elevation of troponin levels, including acute coronary syndromes, myocarditis, arrhythmias, underlying cardiovascular diseases that may not be readily apparent, and systemic inflammatory syndrome [7, 8].
The underlying pathophysiological mechanism involves direct viral injury to cardiomyocytes [9]. The virus enters these cells via the angiotensin-converting enzyme 2 (ACE2) receptor, which is abundantly expressed in cardiomyocytes [9]. Once inside the cells, the virus can replicate and trigger inflammatory responses, leading to myocardial damage and inflammation. The immune response, characterized by the release of pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α), occurs in response to the viral infection and can initiate a systemic inflammatory cascade, including inflammation of the heart muscle.
COVID-19 is also associated with endothelial dysfunction, which can impair blood flow to the heart muscle, resulting in ischemia and inflammation. This condition increases the risk of coronary microcirculatory thrombosis, further contributing to myocardial ischemia and inflammation [9]. cMRI serves as a valuable diagnostic tool for patients with elevated hs-cTnI levels of uncertain etiology, as it can quantitatively assess ischemia and provide detailed tissue characterization, including scar tissue, diffuse fibrosis, and edema [10].
The current study aimed to evaluate long-term cardiac function in COVID-19 survivors who had experienced COVID-19 acute myocarditis. We assessed the correlation between the extent of myocardial injury, as indicated by hs-cTnI levels, with findings from multimodal imaging techniques, including echocardiographic and cMRI parameters, in patients hospitalized due to SARS-CoV-2 across two centers in Crete during the first 6 months of follow-up.
Material and methods
Patient population
We conducted a two-center prospective cohort study, including all patients aged 18 to 45 years who were hospitalized at the University General Hospital of Heraklion and the General Hospital of Chania with a COVID-19 diagnosis and elevated hs-cTnI levels, subsequently diagnosed with myocarditis. Diagnosis of COVID-19 infection was confirmed either through tracheal aspirate or oro/nasopharyngeal swabs for SARS-CoV-2 via reverse-transcriptase polymerase chain reaction (RT-PCR). According to guidelines for symptomatic individuals suspected of having COVID-19, swab specimens should be collected and tested from the nasopharynx (NP), anterior nares (AN), oropharynx (OP), or mid-turbinate (MT) regions; saliva or mouth gargle may also be used [11].
The diagnosis of myocarditis in our study was based on a comprehensive evaluation that included clinical presentation, electrocardiography (ECG), echocardiography, laboratory tests, and cMRI during hospitalization when available. Key laboratory findings included elevated (hs-Tn) levels and inflammatory markers such as C-reactive protein (CRP), procalcitonin, ferritin, and IL-6. Symptoms suggestive of myocardial involvement such as chest pain or discomfort, dyspnea, palpitations, and syncope were noted. These symptoms were indicative of myocardial inflammation and guided further diagnostic evaluation. Although ECG abnormalities in myocarditis are not pathognomonic, the most common findings observed in our cohort were ST-segment alterations and sinus tachycardia. Echocardiographic findings in our patients primarily included impaired LVGLS and pericardial effusion. While these findings are not specific to myocarditis, they were instrumental in excluding other causes of cardiac dysfunction and monitoring disease progression. cMRI was not available for all patients during hospitalization in this study. When performed, it provided critical information for confirming the diagnosis based on the updated Lake Louise criteria.
The 6 months post-discharge follow-up included a comprehensive patient history, clinical examination, electrocardiogram, transthoracic echocardiography, cMRI, and a laboratory panel. In our study, patients with septic shock, acute pulmonary embolism, myocardial infarction, established cardiovascular disease, or arrhythmias were excluded. We also did not include patients with valvular or congenital heart disease, nor those with a history of thromboembolic events. The severity of the disease was assessed using the CURB-65 scoring system. For patients exhibiting significant myocardial injury, indicated by troponin levels above 1000 pg/dl, non-invasive tests such as nuclear scintigraphy or dobutamine stress testing were performed to exclude coronary artery disease.
Ethical approval was obtained from the Ethics Committee of the General Hospital of Chania for the use of patient clinical data for research purposes. All participants provided written informed consent. The study protocol complies with the ethical guidelines outlined in the 1975 Declaration of Helsinki.
Severity assessment tools
CURB-65 was applied according to the following criteria:
C – Confusion – 1 point.
U – Blood urea nitrogen (BUN) level greater than 7 mmol/l or greater than 20 mg/dl – 1 point.
R – Respiratory rate exceeding 30 breaths per minute – 1 point.
B – Systolic blood pressure less than 90 mm Hg or diastolic blood pressure less than 60 mm Hg – 1 point.
65 – Age greater than 65 – 1 point.
Patients with a CURB-65 score higher than 2 were considered to be at high risk for mortality [12].
Echocardiography
2D echocardiography and Doppler measurements were used for the evaluation of left ventricular function, and more specifically, peak early (E-wave) and late (A-wave) transmitral filling velocities and their ratio E/A, deceleration time of E velocity (DTE) and the mitral inflow velocity E to tissue Doppler E′ (E/E′) were measured. Two-dimensional speckle-tracking echocardiography (STE) with frame rates of 50–85 Hz was used to assess the global longitudinal strain of both left and right ventricles. Mean global longitudinal strain (GLS) was calculated by averaging the peak GLS values of apical two-chamber, apical three-chamber, and apical four-chamber images. Automatic endocardial margins were observed at end-systole. Manual adjustments were made to ensure accurate tracking where necessary and to include LV wall thickness. The standard GLS limit was identified as < –18%.
cMRI
The Lake Louise Criteria for the diagnosis of myocarditis, established in 2018, stipulate that the presence of at least one T1-based indicator of nonischemic myocardial injury – such as abnormal T1 mapping, elevated extracellular volume (ECV), or (LGE) – is necessary, along with one T2-based indicator of myocardial edema, which can be identified through abnormal T2 mapping or regional irregularities on T2-weighted imaging [13].
Statistical analysis
The summary of descriptive statistics is presented as mean ± standard deviation (SD) for continuous categorical variables. The paired samples t-test or paired Wilcoxon test was used for assessing the effect of treatment, if the distribution was parametric or nonparametric, respectively. Multiple logistic regression analysis was applied to identify the correlations among several variables.
Results
Atotal of 59 patients (31.8% of total 185 admissions with COVID-19 infection and high levels of hsTnI from any cause) with COVID-19 infection and clinical manifestations of myocarditis, characterized by significantly elevated hs-TnI levels, were included in the study. The mean hsTnI values were 281.27 ±400.86 pg/ml. The mean age of the participants was 41 ±20 years, with a predominance of male patients (70%).
Demographic and clinical characteristics of the cohort are summarized in Table I. Notably, 22 (37.3%) patients were hypertensive, 10 (16.9%) had diabetes, 18 (10.9%) were hyperlipidemic, and 22 (30.3%) were active smokers. Additionally, 9% reported a positive family history of cardiovascular events.
Table I
Baseline characteristics of patients
| Clinical parameters | Patients (n = 59) |
|---|---|
| Age | 41 ±20 |
| BMI n (%) | 20.5 ±7.1 |
| Hypertensive (%) | 37.3 |
| Diabetic (%) | 16.9 |
| Smokers (%) | 30.3 |
| SBP/DBP [mm Hg] | 115.7 ±19.3/77.4 ±12.3 |
| hs-cTnI [ng/dl] | 400.861 ±281.27 |
The median duration of inpatient hospital stay was 9 days, with a range starting from 2 days. Furthermore, 54.24% of patients received intravenous antiviral therapy with remdesivir, administered based on disease severity as assessed by the CURB-65 scoring system; scores above 2 indicated severe disease.
Echocardiographic findings
All patients underwent detailed echocardiographic evaluations within the first 6 months of observation. Table II summarizes the echocardiographic findings. LV function was assessed using 2D echocardiography and Doppler measurements. While the overall LV systolic function, as indicated by LVEF, was normal at 57.54 ±5.032%, the LVGLS was significantly lower in COVID-19 recovered patients, measuring –17.01 ±2.396%. In contrast, RVGLS showed no significant reduction, measuring –21.54 ±2.396%.
Table II
Echocardiographic indexes of our patients
[i] IVS – interventricular septum in diastole, PW – posterior wall in diastole, LVEF – left ventricular ejection fraction (Simpson’s biplane), LAVi – left atrial volume index, LVGLS – global longitudinal strain of the left ventricle, RVGLS – global longitudinal strain of the right ventricle, E – peak early diastolic mitral flow velocity, E′ – mitral annulus early diastolic velocity.
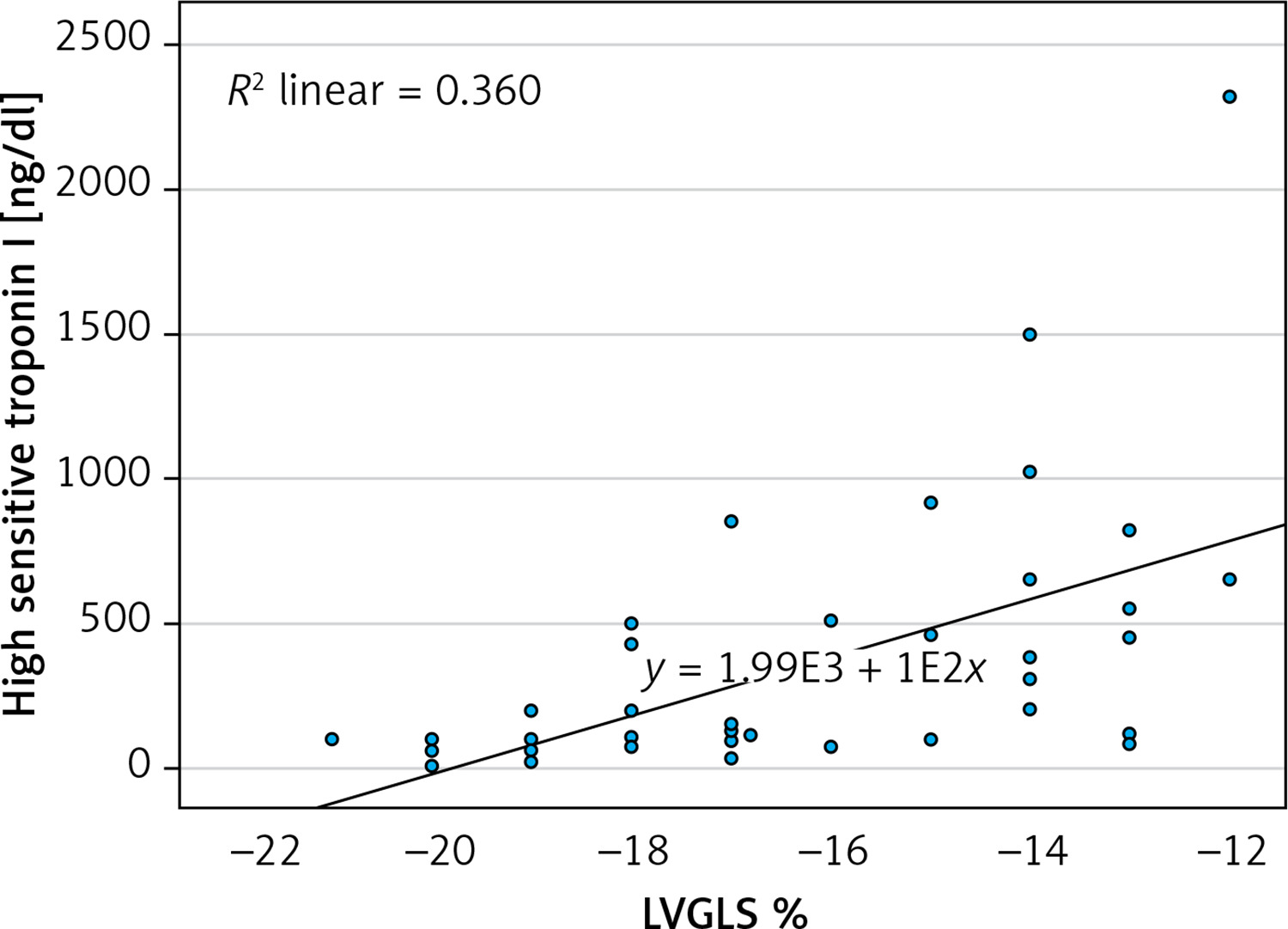
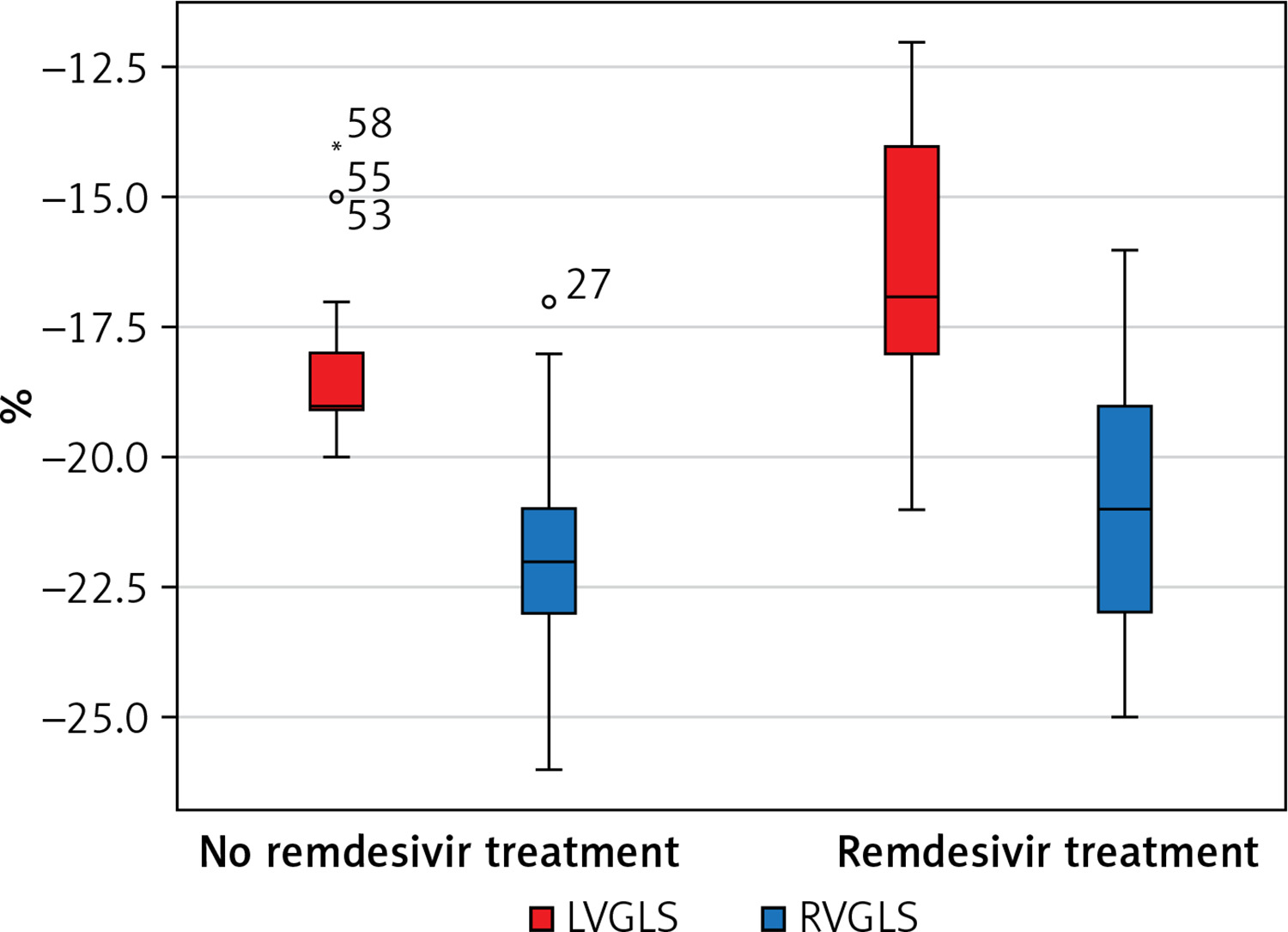
LV filling pressures, assessed through the E/A ratio and E/e′ ratio, did not demonstrate any deterioration. Notably, hs-cTnI levels showed a significant correlation with LVGLS. Specifically, peak hs-cTnI concentrations were higher in patients exhibiting reduced LVGLS (p < 0.001), while no correlation was found with LVEF or RVGLS (Figure 1). Furthermore, the reduction in LVGLS was strongly associated with remdesivir treatment, indicating that patients in more severe states, as determined by higher CURB-65 scores, experienced greater reductions in LVGLS (Figure 2). The strongest predictor of LV systolic dysfunction appeared to be elevated hs-cTnI levels.
cMRI findings
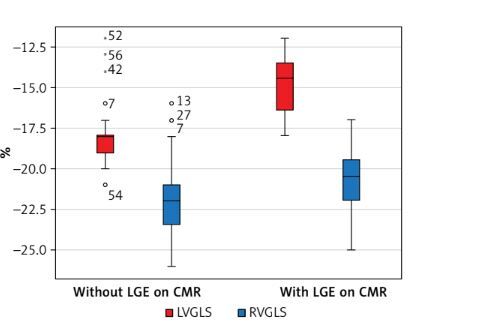
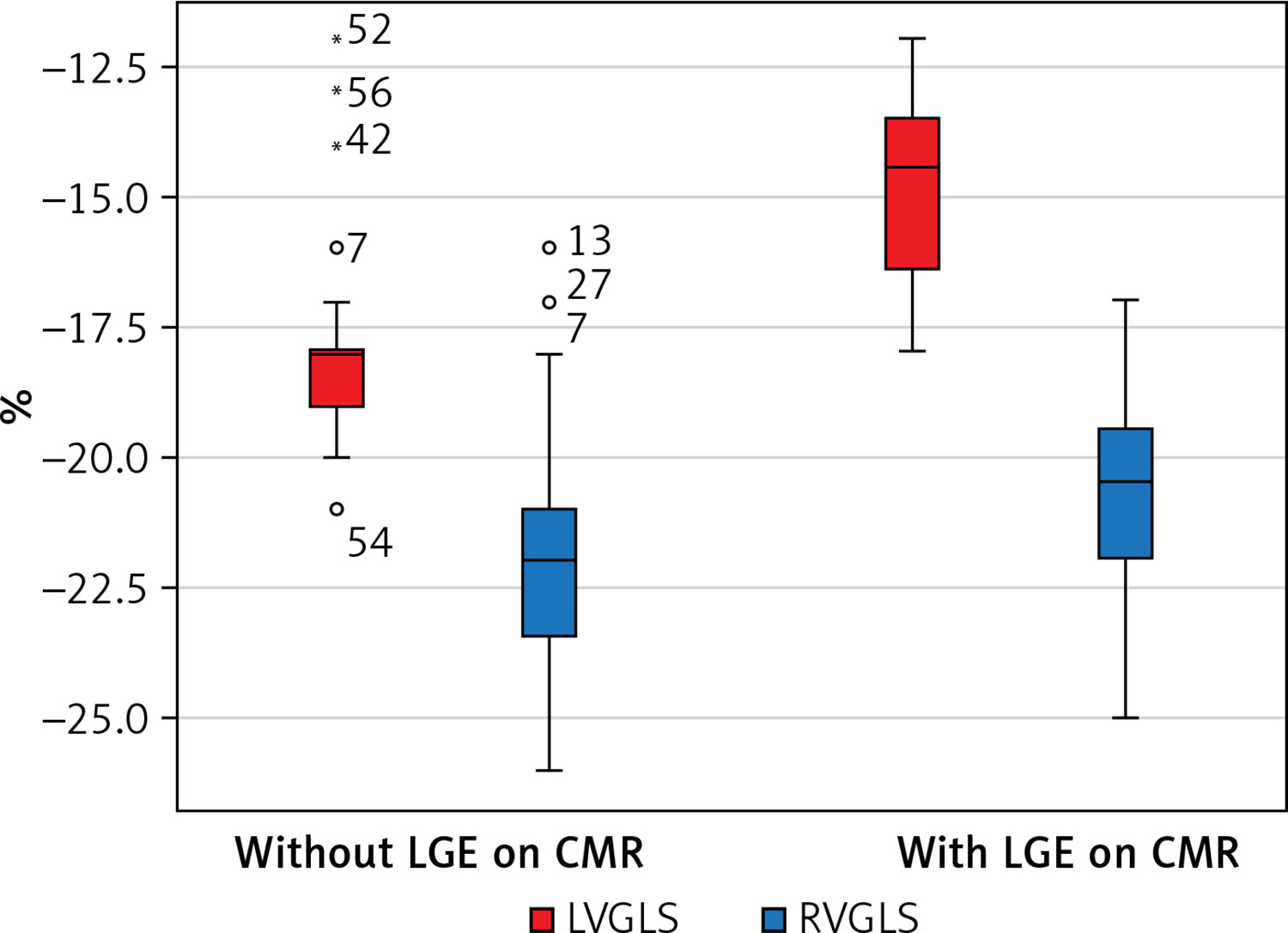
cMRI was performed as the second imaging modality. All of our patients showed abnormal native T1 values and increased T2 signal intensity. Among our patients, 17 (28.82%) exhibited LGE with subepicardial or mid-wall distribution, which can be classified as non-ischemic myocarditis-like LGE. Of these patients, 8 (50%) had involvement of one myocardial segment, 2 (34%) had two segments affected, and 7 (16%) had three segments involved; however, biventricular function remained preserved. The presence of LGE on cMRI was significantly associated with a reduction in LVGLS (–14.79 ±1.69%; p < 0.001) (Figure 3).
Figure 3
Patients with late gadolinium enhancement (LGE) observed on cardiac magnetic resonance imaging (CMR) exhibited impaired left ventricular global longitudinal strain (LVGLS) as measured by speckle tracking echocardiography (STE). In contrast, no significant correlation was found between right ventricular global longitudinal strain (RVGLS) and LGE on CMR
Discussion
COVID-19 is known to affect multiple organ systems, with many patients exhibiting release of troponin, a marker of acute myocardial injury [1]. While hs-cTnI elevation above the upper reference limit (URL) at the 99th percentile is considered the primary indicator of myocardial injury, the underlying pathophysiological mechanisms must be clarified based on specific clinical contexts [14]. Although ischemia is often identified as the most common cause of myocardial injury, several non-ischemic processes may also contribute, including apoptosis, myocardial strain, myocyte necrosis, and increased cell membrane permeability, leading to troponin release through exocytosis [15, 16].
The mechanisms by which COVID-19 contributes to myocardial injury include increased metabolic demands due to acute illness, hypoxemia, and the inflammatory cascade triggered by cytokine release. Additionally, microvascular damage resulting from disseminated intravascular coagulation and thrombosis, as well as acute coronary syndrome due to inflammation-triggered destabilization of atheromas, are significant contributors [10]. Conversely, some studies suggest that microangiopathic thrombosis may occur throughout the vascular system even in the absence of epicardial coronary artery dysfunction.
Hypercoagulability, endothelial injury, vasculitis, cytokine storms, and thrombosis are implicated in various complications such as pulmonary embolism, strokes, small asymptomatic brain infarcts, and peripheral embolism [14].
cMRI has proven effective in characterizing myocardial injury patterns. Three distinct patterns have been identified: non-ischemic non-specific scars, myocarditis-pattern injuries, and dual pathology featuring both ischemic and non-ischemic characteristics. In most patients diagnosed with myocarditis, involvement was limited to three or fewer segments; biventricular function was preserved, with no regional wall motion abnormalities present. Myocarditis-like injury during convalescence after severe COVID-19 appears to be limited in scope and has a minimal functional impact [17, 18].
This study examined the long-term effects of COVID-19 on cardiac function, focusing on hospitalized patients diagnosed with myocarditis. The severity of COVID-19 at presentation was assessed using the CURB-65 scoring system, which considers blood urea nitrogen levels, respiration rate, systolic and diastolic blood pressures, and age.
The initial evaluation for patients with an acute rise in hs-cTnI should involve echocardiography. Our findings indicated that patients did not show reductions in LVEF or diastolic function impairment. However, indices of deformation – particularly LVGLS – were significantly affected in patients with elevated hs-cTnI levels, independent of LVEF. Recent studies have underscored the importance of STE in diagnosing myocarditis by correlating regions of LGE observed on cMRI with reductions in longitudinal strain [18–21].
Our study revealed a strong correlation between hs-cTnI levels and reduced LVGLS that was unaffected by antiviral therapy administration. LVGLS appeared compromised in patients with COVID-19-related myocarditis and remained abnormal 6 months post-admission in those with higher peak hs-cTnI values; this finding corresponded with the presence of LGE on cardiac MRI. Previous studies have similarly demonstrated correlations between abnormal LVGLS and LGE during convalescence after severe COVID-19 infection [14, 18].
Patients diagnosed with myocarditis based on cMRI criteria exhibited subepicardial or mid-wall LGE findings consistent with non-ischemic myocarditis abnormalities. In a small subset of patients, aberrant cMRI findings included elevated T1 and T2 values in the myocardial septum, indicative of widespread fibrosis and edema – consistent with recent publications highlighting cMRI findings in a significant proportion of patients with mild illness [14, 18].
Notably, LVGLS can predict areas of LGE with greater diagnostic accuracy than LVEF. As an echocardiographic marker for subclinical systolic dysfunction, LVGLS can be used for long-term monitoring and prognostic stratification of myocarditis patients. Recent studies have emphasized the importance of LVGLS in risk stratification for COVID-19 patients while acknowledging the limited number of myocarditis cases studied [22].
Echocardiography offers a bedside diagnostic and prognostic evaluation alternative to cMRI, addressing challenges associated with transporting critically ill COVID-19 patients. Furthermore, antiviral therapy appears correlated with lower LVGLS values; this phenomenon may primarily reflect disease severity. Patients scoring above 2 on the CURB-65 scale received remdesivir treatment and exhibited higher hs-cTnI levels alongside greater acute phase inflammatory markers. However, remdesivir has been associated with cytotoxic effects on cardiomyocytes that may exceed those caused by chloroquine due to its interaction with human mitochondrial RNA polymerase [23].
STE effectively identifies subclinical systolic dysfunction and correlates well with the presence of LGE observed in cMRI. Patients with higher hs-cTnI values exhibited non-ischemic LGE patterns and lower LVGLS values, indicating more significant impairment in ventricular deformation and myocardial scarring. These patients also received antiviral treatment during hospitalization, reflecting the severity of their condition according to CURB-65 criteria.
Remdesivir was thought to be associated with significant cytotoxic effects in cardiomyocytes, which appear to be more pronounced than the cardiotoxic effects observed with chloroquine. The mechanism underlying remdesivir-induced cardiotoxicity is primarily attributed to its binding to human mitochondrial RNA polymerase. However, a recent post hoc analysis indicated that remdesivir therapy did not correlate with an increased incidence of cardiac adverse events compared to control groups among hospitalized patients with moderate or severe COVID-19 [23]. LVGLS is compromised in COVID-19-related myocarditis patients and shows progressive deterioration in those with elevated hs-cTnI levels while maintaining preserved EF. Although these findings contribute valuable insights into COVID-19-related myocarditis, our study has limitations, including a small sample size that restricts accurate evaluations regarding the role of STE in this context, and the non-use of cMRI in the acute phase due to COVID restrictions. Other studies have also recognized the significance of STE in COVID-19 myocarditis patients; thus, our research adds important evidence for understanding this complex condition [24].
In conclusion, our study supports the use of STE for diagnosing and monitoring COVID-19 myocarditis, as it correlates well with LGE detected by cMRI. In convalescent patients with COVID-19 who were hospitalized due to severe illness, as indicated by CURB-65 criteria, higher elevation of hs-cTnI levels may suggest a worse future outcome.
Our findings indicate that hs-cTnI levels can serve as a predictor for future deterioration in GLS among COVID-19 patients. Future studies should focus on assessing whether this impairment in LVGLS worsens over time and whether it is associated with adverse cardiac events following myocarditis.