
Introduction
Cardiovascular disease is the leading cause of death among patients undergoing kidney replacement therapy, with 50% of hemodialysis patients dying of cardiovascular events [1]. A significant percentage of these patients have an arteriovenous fistula (AVF), but end stage kidney disease (ESKD) leads to a) volume overload due to Na+ and fluid retention, b) increased cardiac output (CO) due to chronic anemia, and c) increased incidence of arteriosclerosis and hypertension [1, 2]. Thus, it is not always easy to decide whether a particular cardiac complication is due to ESKD, the deleterious effects of an AVF (mainly the volume overload), or to a combination of both. In this narrative review, we focus on enlightening this area based on the current evidence in the English literature. Keywords: end stage kidney disease, arteriovenous fistula, heart failure, high flow vascular access, flow-restrictive procedures
Pathophysiology
Cardiovascular alterations
Normal flow in the brachial artery is about 50 ml/min. Within a day after AVF creation, flow increases to 40–60% (> 300 ml/min) of its expected maximal rate, which usually occurs at 6 weeks (> 600 ml/min). The typical postoperative flow for a brachiocephalic fistula is twice the flow of a radiocephalic AVF, due to the greater vessel diameter, as is predicted by Poiseuille’s law [1]. In time, any further venous outflow tract dilatation may further aggravate flow.
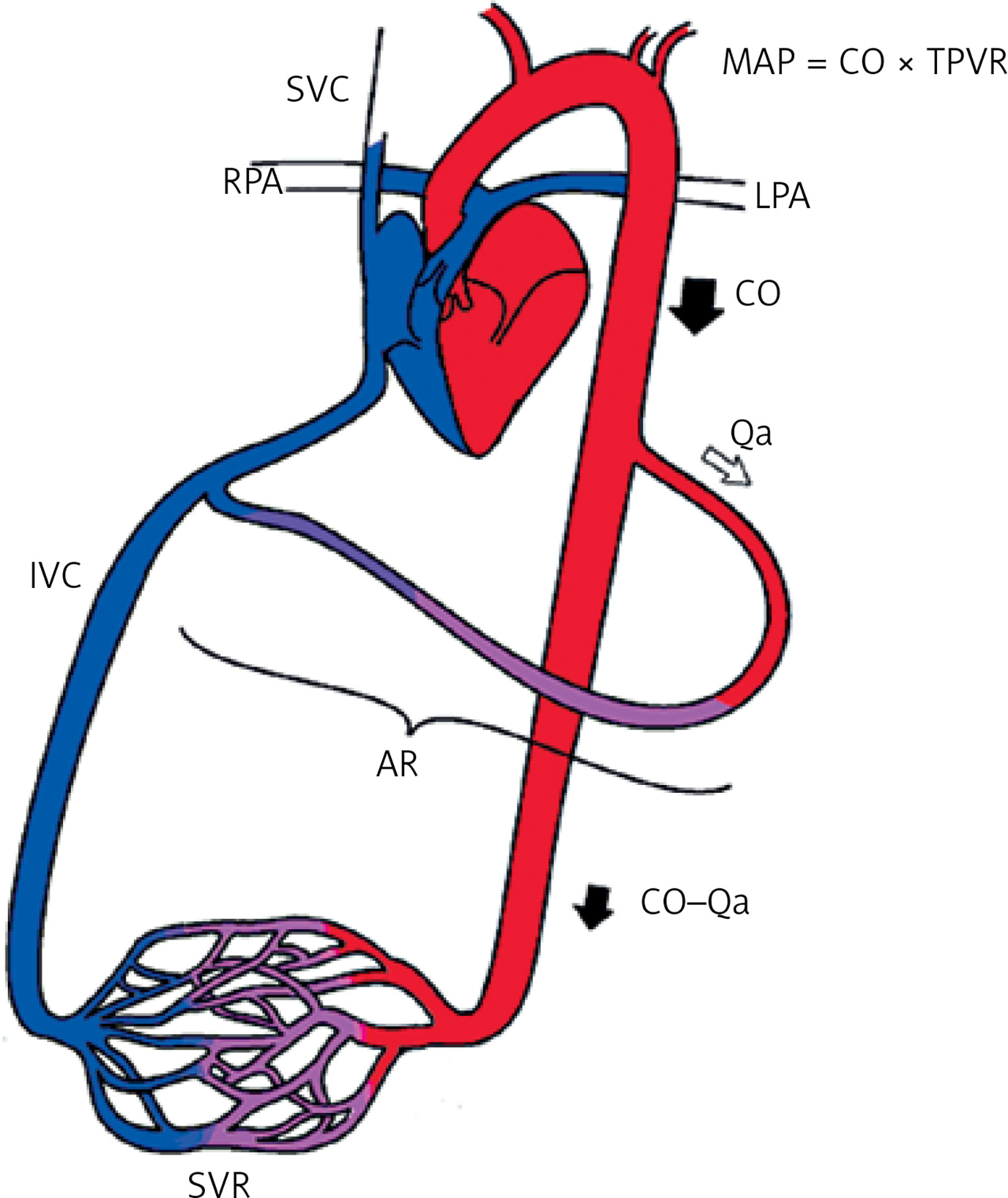
It is generally known that these circuits allow for free blood flow from the high-pressure arterial system to the low-resistance venous circulation. This artificial conjunction lowers peripheral arterial resistance as flow detours the peripheral capillary vascular bed, resulting in blood pressure (BP) reduction. This, in turn, through activation of baroreceptors and ultimately the sympathetic nervous system, leads to increased heart rate and myocardial contractility [1] (Figure 1). Subsequently, the reduction in BP activates the renin-angiotensin-aldosterone system, thus stimulating renal salt and water retention, leading to an increase in blood volume [2]. The subsequent increases in venous return (preload) and cardiac output (CO) are the primary drivers of hemodynamic changes that may compromise cardiac function, especially in patients with subclinical cardiovascular disease. The CO increases to 10–20% immediately after AVF creation. Within the first week, increased blood volume causes an increased left ventricular end diastolic volume (LVEDV). This leads to the release of atrial natriuretic peptide (ANP) and the B-natriuretic peptide (BNP) [2, 3]. These peptides partially inhibit the renin and aldosterone secretion and further reduce the peripheral vascular resistance [4, 5]. As these metabolic changes persist in the long term, cardiac complications may arise.
Figure 1
AV access forms a parallel circuit to the systemic circulation leading postoperatively to lower peripheral resistance, increase in CO, contractility, stroke volume and heart rate
SVC – superior vena cava, LPA – left pulmonary artery, RPA – right pulmonary artery, IVC – inferior vena cava, MAP – mean arterial pressure, CO – cardiac output, Qa – AVF flow rate, AR – AVF resistance, SVR – systemic vascular resistance, TPVR – total peripheral vascular resistance (TPVR = PVR + AR).
Cardiac compensation
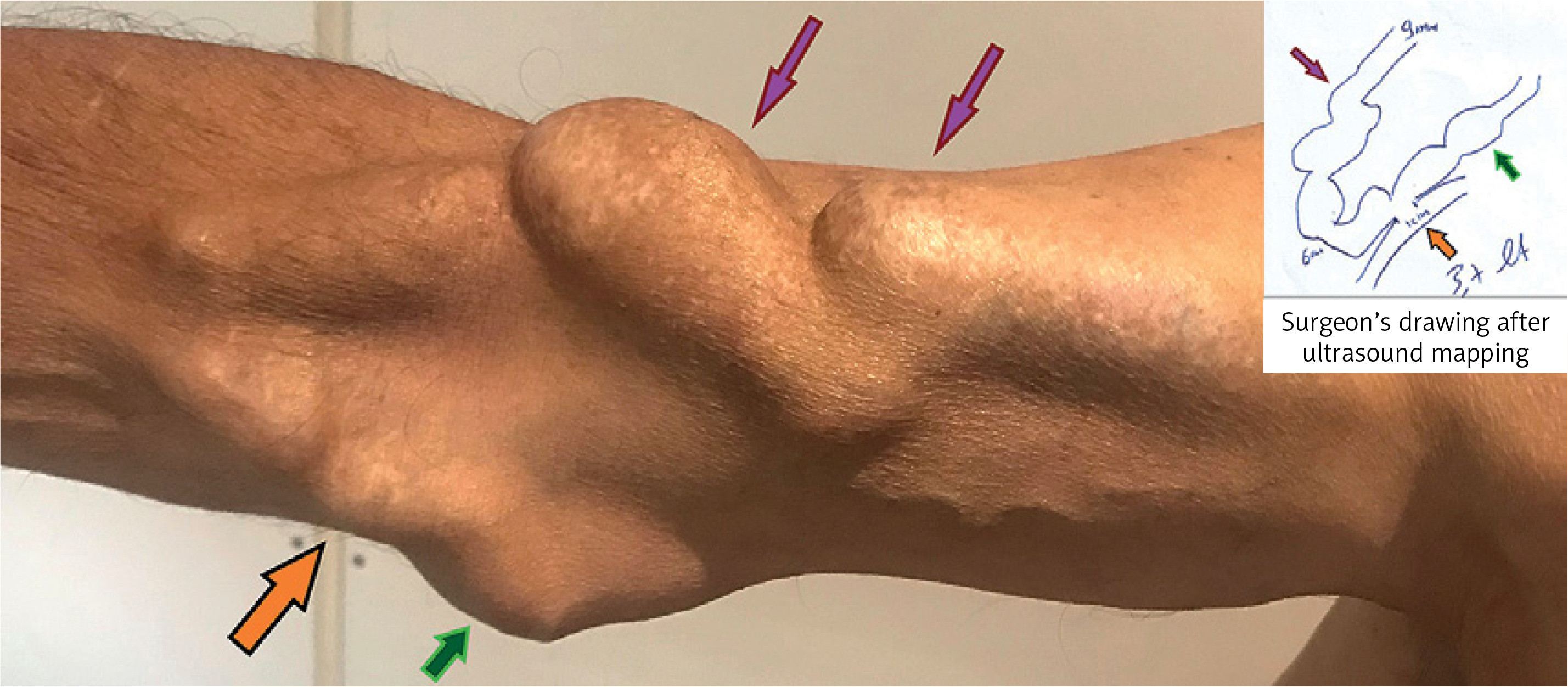
Arteriovenous fistula flow patterns may change substantially after months or years, due to both venous outflow tract dilatation and arterial wall remodeling. Gradually increasing flow occurs typically in brachiocephalic and brachiobasilic AVFs and is less common in radiocephalic AVFs or arteriovenous grafts (AVGs). Grafts cannot dilate over time. In contrast, AVF chronic dilation may sometimes be severe, leading to a megafistula formation, which is defined as generalized aneurysmal dilatation of the outflow venous path (Figure 2). It has been reported that for an AVF flow rate below 2.2 l/min, the CO increase is in proportion to the AVF flow. But when the flow rate exceeds 2.2 l/min, the CO increase cannot compensate for the functional overload, suggesting that there is a threshold above which cardiac compensation is compromised. Consequently, in the early stages, a hyperdynamic state with increased heart rate, stroke volume (SV), CO and left ventricular ejection fraction (LVEF) occurs. At some point this hyperdynamic circulation may be combined with signs and symptoms of heart failure (HF) (high-output heart failure (HOHF) with increased or preserved LVEF) but in the long term it leads to reduced LVEF via reduced myocardial contractility (HOHF with reduced LVEF) [6].
Echocardiographic changes
It is noteworthy that at the beginning of hemodialysis, before vascular access creation, particular echocardiographic findings may be revealed in ESKD patients: a) an increase in left ventricular end-diastolic diameter (LVEDD), b) increased contractility, c) increased SV, d) increased CO and e) increased left ventricular end-diastolic pressure (LVEDP) [2]. Moreover, specific findings may be revealed in transthoracic echo in patients with an AVF, even without a relevant prior cardiovascular history. These include a significant alteration in LVEF, a slight increase in left atrial diameter (LAD), a substantial increase in left ventricular end-diastolic diameter (LVEDD) and an increase in inferior vena cava diameter (IVCD) [7].
Cardiac complications
Arteriovenous fistula creation may contribute to the following pathological conditions affecting the heart: a) heart failure (HF), b) left ventricular hypertrophy (LVH), c) pulmonary hypertension (PH), d) right ventricular dysfunction (RVD), e) coronary artery disease (CAD) and f) valvular dysfunction (VD) in end-stage renal disease (ESRD) patients [2].
Heart failure
It should be noted that about 35–40% of ESKD patients have pre-existing clinical or subclinical HF at the time of dialysis initiation, which is associated with a high mortality risk [2, 8]. The subclinical presentation is due to reduced activity or mobility. HOHF is characterized by the well-recognized signs and symptoms of exertional dyspnea (or at rest), orthopnea, weakness, and edema at rest in combination with increased CO (greater than 8 l/min) or a cardiac index (CI) > 3 l/min/m2 [2]. AVF may provoke or exacerbate subclinical CHF due to extra flow load. Patients in this subgroup are usually those with an AVF flow (Qa) > 2 l/min or a Qa/CO ratio greater than 30% [9, 10]. Fifteen percent of AVF patients belonged in this category in a previous study [2]. The incidence of HOHF is related to AVF flow, but the AVF flow is not correlated with mortality [2]. A recent study conducted in 100 patients with a past medical history insignificant for cardiovascular disease showed that 24% of them with an AVF flow > 2 l/min (mean flow volume: 958 ml/min vs. 3430 ml/min in the two groups) demonstrated larger left atrial (LA) and left ventricular (LV) dimensions, a Qa/CO ratio > 20% (29% vs. 11%), decreased LVEF (57% vs. 62%), and an EF below normal in 12% of the patients (LVEF < 55%) [11]. Although most AVFs are well tolerated by most patients, even overflowing, we must emphasize that patients with reduced myocardial reserves may present with overt HF signs, even if accommodating an AVF with a normal flow (e.g. 600–1200 ml/min). In other words, a normal flow AVF may decompensate a previously compensated or subclinical HF.
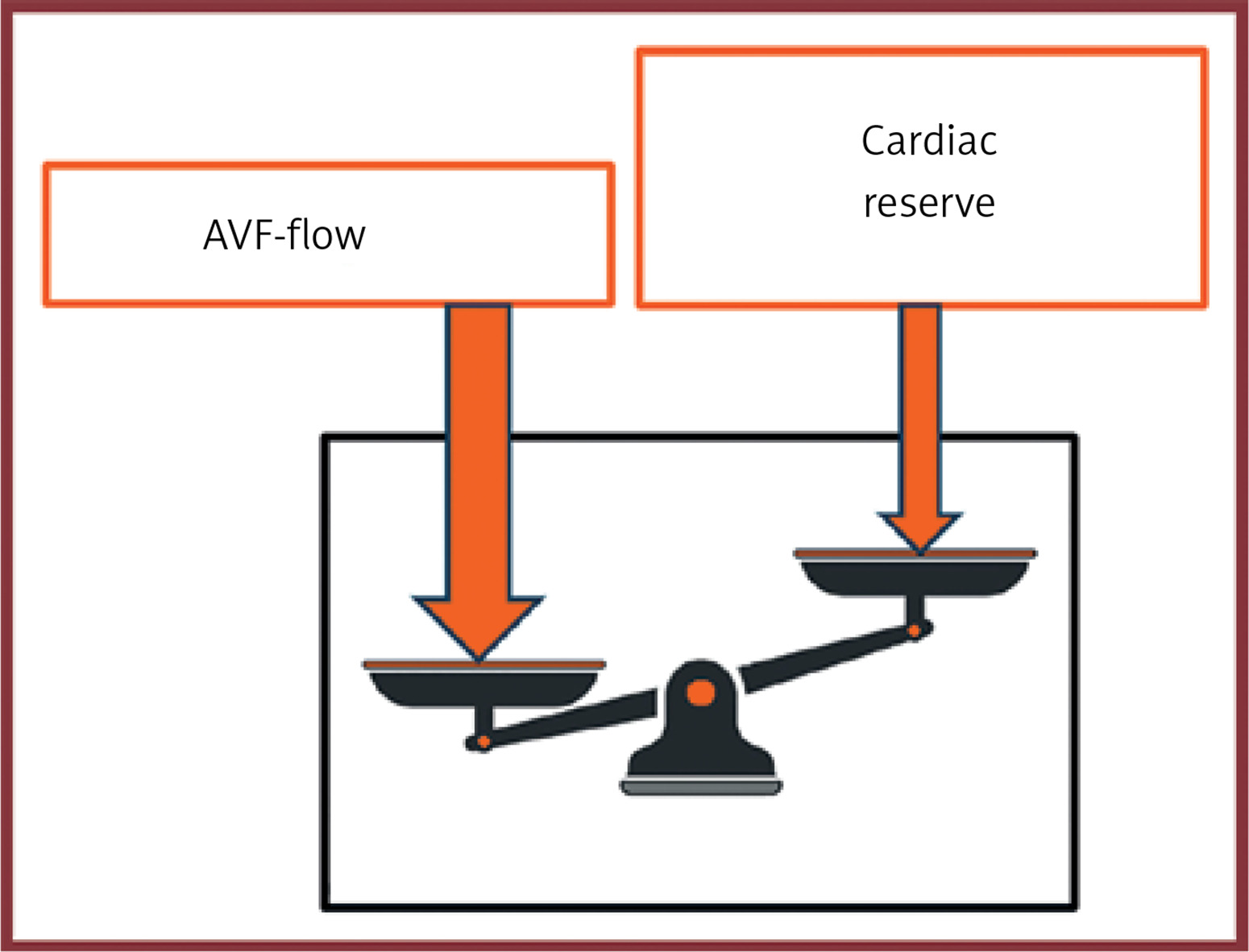
As the above shows, clinical symptomatology is the result of an interplay between the severity of prior cardiac comorbidity and the AVF flow (Figure 3). Patients with a normal heart may tolerate extreme flow volumes with no apparent clinical symptoms. On the other hand, patients with reduced myocardial reserves (e.g. with subclinical or mild HF) will show severe HF symptoms even with low or normal AVF flows. Consequently, it is important to timely identify the small subgroup of patients with an increased risk of developing HF after AVF creation.
Left ventricular hypertrophy and fibrosis
Left ventricular hypertrophy is a common finding among ESKD patients, being present in about 70% of them. This is caused by hypertension, volume overload, and anemia. AVF creation can further aggravate this condition since the increase in CO leads to a significant increase in myocardial mass and LV diameter. In a recent study, among patients with an AVF flow > 600 ml/min, a mean increase in myocardial mass of 7.4 g was evident in cardiac MRI after 6 weeks, whereas in patients with AVF flow < 600 ml/min the increase in myocardial mass was insignificant [12]. Moreover, in a previous retrospective study of our center regarding kidney transplant recipients, we found that a functioning AVF was associated with increased LVEDD in the long term (2 and 5 years after transplantation) in comparison to recipients with no functional AVF [13]. Additionally, it has been reported that LV hypertrophy is sustained in transplanted patients with a functional AVF, while AVF banding with flow restriction leads to regression of hypertrophy in 3–10 weeks [2]. On the other hand, it was reported that myocardial fibrosis, assessed by non-contrast cardiac MRI, was more prominent in ESKD patients with a Qa > 2 l/min, compared with ESKD patients with a Qa < 2 l/min and with healthy volunteers. Hence, the remodeling is directly influenced by both the presence of a high flow AVF and the uremic conditions of the ESKD [14].
Pulmonary hypertension
ESKD is a contributing factor in PH development as PH is found in 12–45% of hemodialysis patients [2]. It is most commonly attributed to ESKD-related conditions such as a) systolic and diastolic LV dysfunction, b) volume overload, c) endothelial dysfunction affecting the vascular muscle tone (via decreased nitric oxide and increased endothelin 1 and wall shear stress), and sleep apnea syndrome [15].
It has been reported that the presence of a functional AVF is an independent risk factor for PH development. This is attributed to the increased blood volume in the pulmonary circulation and to endothelial dysfunction. Pulmonary hypertension tends to worsen over time after AVF creation, and AVF flow and duration are related independently to the severity of PH [15]. Compared with patients undergoing peritoneal dialysis, patients with AVF demonstrated statistically significantly higher pulmonary pressures [16]. In a study of 58 hemodialysis patients with AVF, those with PH showed a significantly higher CO. However, increased CO cannot by itself be the cause of PH due to the enormous capacity of pulmonary microcirculation. Thus, it is speculated that PH is attributable to increased pulmonary vascular resistance or a diminished vasodilatory response to the increased cardiac output [17]. Moreover, it was found that attenuated basal nitric oxide production in patients with PH on hemodialysis contributed to increased pulmonary vascular tone [17].
Temporary AVF closure/ligation by means of external pressure or permanent banding leads to a decrease in pulmonary arterial pressure. The evidence is conflicting, as PH may sometimes be self-limited after transplantation, without AVF banding or ligation. Some believe that pre-existing pulmonary dysfunction is essential as a background for further deterioration by the AVF volume overload. Further evidence is needed for conclusive results [18].
Right ventricular dysfunction
The effects of high-flow AVFs on right ventricular (RV) function have not been studied thoroughly. In initial studies, echocardiographic parameters of RV function were compared between hemodialysis patients and peritoneal dialysis patients [16, 19]. Increased prevalence of RV dysfunction in the hemodialysis group was observed, especially in those patients with an upper arm AVF (vs. forearm AVF). Subsequent studies confirmed these results and also showed that RV dysfunction is not always associated with PH [20]. Others claim that RV function tends to worsen in the presence of PH [20–23]. Conversely, more recent data do not support an association between AVF and RV dysfunction in ESRD patients [7, 24].
Coronary artery disease
Coronary artery disease is common among hemodialysis patients and is accompanied by worse reperfusion outcomes [25]. A prospective study suggested that ESKD patients might be more susceptible to subendocardial ischemia after AVF creation, owing to the increased myocardial oxygen demand secondary to the increased CO, after AVF creation [26]. In patients undergoing coronary artery bypass grafting (CABG), steal phenomena pose another concern. Echocardiographic findings of ischemia have been demonstrated during dialysis in patients in which the internal thoracic artery (ITA) has been utilized as a graft [27]. Although there have been conflicting results, AVF creation contralateral to the grafted ITA should be considered [28]. Lastly, high-flow AVFs might affect perioperative decisions on administration and weaning from cardiopulmonary bypass [2].
Valvular dysfunction
Common physiological mechanisms of ESRD have been associated with valvular calcifications or the development of functional valvular disease [29]. The contribution of AVF access alone in the development of valvular disease has not been studied. Most existing data concern the effects of AVF on aortic stenosis (AS) [30, 31]. A recent study confirmed that AVF can affect echocardiographic parameters differently in mild and severe AS [32]. Other types of vascular access might be preferable for this subgroup of patients owing to the high risk of clinical decompensation in patients with AS [31].
Surgical perspectives
Indications for flow-reduction procedures
Flow-reduction procedures are rarely required in high-flow AVFs, as most patients tolerate the excess load well (Figure 4). In a report by Dixon et al., they were needed in only 2.6% of 322 AVFs [33]. Patients with overt signs and symptoms of HOHF and high-flow AVF are candidates for flow-reduction procedures. In the group of patients with no or minimal symptoms and flow overload (Qa > 2 l/min or a Qa/CO ratio > 30%) there is a subgroup at very high risk of developing progressive cardiac deterioration. It includes those with a) LV diastolic dysfunction and pulmonary hypertension accompanied by high levels of ANP, BNP, and NT-proBNP, b) a significant drop in LV global longitudinal strain (GLS < –18), and c) a reduction of CO > 2 l after external transient AVF closure (Figure 4). These may be considered for flow-reduction interventions [34]. According to the latest guidelines of the European Society of Vascular and Endovascular Surgery (ESVES), patients with vascular access flow greater than 1500 ml/min should be monitored regularly using flow measurements and echocardiography, as well as for clinical signs of HF [35]. The guidelines from the Kidney Disease Outcomes Quality Initiative (KDOQI) suggest an echocardiogram performed every 6 to 12 months and monitoring of changes in Qa/CO [36]. Both agree that patients with a progressive increase in vascular access flow or objective signs of heart failure or gradual deterioration of symptoms, due to decompensation, should be considered for a flow-reduction procedure.
Figure 4
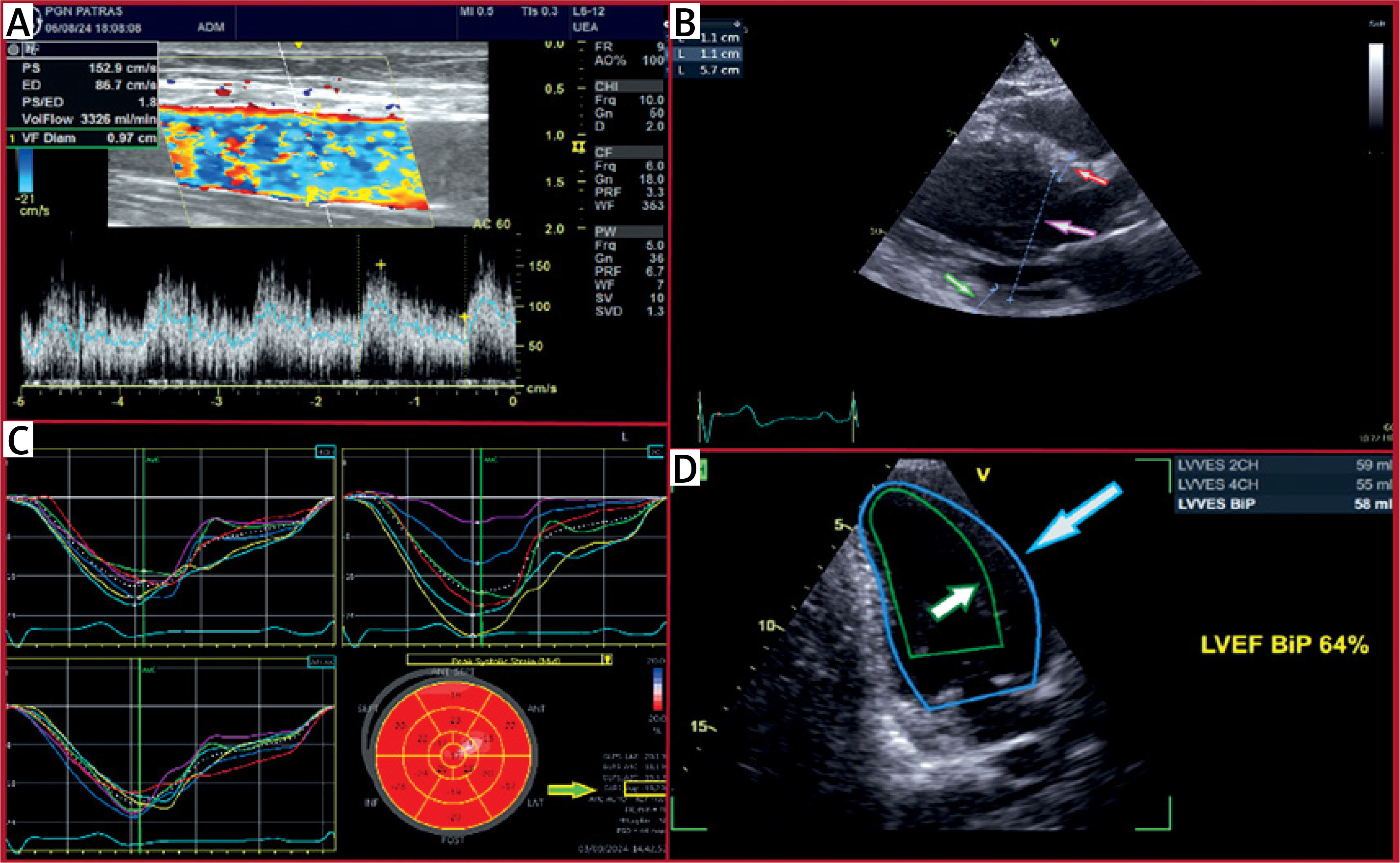
An asymptomatic patient with a well-tolerated high-flow AVF (transposed basilic vein). A – A flow volume > 3 l/min was measured at the brachial artery. B – Echocardiography depicted mild dilated and hypertrophied LV due to volume overload (green arrow: myocardial wall thickness, red arrow: myocardial septal thickness, purple arrow: LV diameter) with systolic indices (LV ejection fraction and global longitudinal strain) in the upper normal range. C – Global longitudinal strain: –19% (green-yellow arrow). D – LVEF: 64% (gray-blue arrow: LV diastole, white-green arrow: LV systole)
Types of intervention
Many procedures have been described to treat hemodialysis-induced distal ischemia (HAIDI) [37]. Some of them treat ischemia through flow reduction in high-flow AVFs. These flow-reduction interventions include the following: a) banding (BD), b) revision using distal inflow (RUDI), c) interposition grafting and d) proximal radial artery ligation (PRAL). AVF ligation is always an option if the patient is at high risk or with a reduced life expectancy or for anatomical or technical reasons [37–40].
BD techniques
A prosthetic band (synthetic PTFE) 10–30 mm in length is wrapped around the outflow vein in the juxta-anastomotic area. To avoid access thrombosis, the minimal accepted flow after banding is 400–600 for AVFs and 600–800 for grafts. Nowadays, banding can be calibrated based on intraoperative flow measurement by ultrasound. Although the intended degree of stenosis is about 60–80%, individualization is required as an increase in diameter by 1 mm increases the flow by 400 ml/min [37].
Plication with metal clips or suturing along the juxta-anastomotic out-flow vein over a Satinsky clamp [37]. This is commonly used to treat venous aneurysms, which are a usual cause of a high-flow state.
BD with a simple ligature: There is a wide variety of different techniques to achieve the ideal out-flow stenosis for the desirable access flow. Some use the Murray nomogram; others suggest reducing the juxta-anastomotic vein diameter by up to 75%, or to less than half of its original size. The minimally invasive limited ligation endoluminal-assisted revision (MILLER) banding procedure includes a tight ligature over an intraluminal balloon (4 or 5 mm), through 2 small skin incisions. It can be performed fully surgically or by a hybrid (endovascular/surgical) procedure, by introducing a balloon with percutaneous access. The extraluminal banding technique suggests placing a balloon or dilator (4, 5, or 6 mm) extraluminally alongside the empty (clamped) outflow vein. Then, the balloon or dilator is removed, and the vein lumen is expanded after the release of perfusion at the predetermined diameter [37].
RUDI
It includes fistula ligation and a short bypass (prosthetic or venous) between the outflow vein and the proximal radial or ulnar artery. In a modification reported as a secondary extension, if technically feasible, the anastomosis is removed distally to the proximal radial or ulnar artery.
PRAL
Radial artery ligation proximal to anastomosis is suggested in Brescia-Cimino high-flow AVFs with cardiac complications and no arm ischemia.
Anastomosis reduction
Anastomosis reduction from within the outflow vein with partial suturing (anastoplasty). Alternatively, a percutaneous covered stent may be placed, protruding to some extent in 3/4 of the anastomosis area or in the juxta-anastomotic outflow vein. Similarly, a tapered flared stent graft can be placed to narrow the lumen as the flared portion is constrained by the width of the vein.
Results of interventions
Banding was shown to produce a clinical improvement in CHF by one NYHA class, which was accompanied by a similar improvement in echocardiography (CO, pulmonary systolic pressure, left ventricular mass index) and decompensation requiring hospitalization [41]. In an interesting case report of a patient who developed severe CHF with a large decrease in EF, 14 years after AVF creation, banding resulted in a marked EF increase [38]. Renal transplant patients showed clinical improvement of HF symptoms after banding [42]. Different flow-reduction techniques achieved a comparable reduction of the access flow and Qa/CO ratio followed by comparable clinical improvement of HF and PH symptoms [43, 44]. However, the access flow may be increased at 12 months after banding, and some suggest a different flow-limiting procedure to be more effective in younger patients [45].
PRAL achieved durable clinical improvement of HF and good patency rates at 24 months in adults and children [46]. In another report where a high-flow radio-cephalic AVF caused HF symptoms, echocardiographic parameters improved immediately after the PRAL procedure as well as at 6 months after intervention [47]. Right-heart catheterization in a patient presenting with HOHF due to a high-flow AVF showed a decrease in CO, pulmonary capillary wedge pressure, Qa and Qa/CO ratio, as well as plasma BNP levels, after the PRAL procedure. No recurrence of HF symptoms was observed [48].
RUDI has also shown adequate patency rates while still efficiently reducing the access flow, confirmed by remission of HF symptoms [49–52]. In one report, the patency of an AVF at 3 years was achieved after re-interventions. High access flow immediately after RUDI and young age were risk factors for the recurrence of high flow [35, 53].
Percutaneous AVF
During the last few years, new percutaneous techniques have been developed for AVF formation. Currently, there are two available devices (the Ellipsys and the WavelinQ systems), both CE-marked and FDA-approved [54, 55]. In percutaneous AVFs, the anastomosis is created at the deep venous system of the forearm, and blood is drained to the superficial system for cannulation via the perforator vein. So far, both studies and anecdotal experience suggest that percutaneous AVFs have lower flow rates compared to surgical ones. This is due to the limited aneurysmal formation at the cannulation site and because deep veins are more difficult to dilate compared to superficial ones. Hence, the deep venous component of the circuit regulates flow and restricts the dilation of the anastomosis [56, 57]. Further studies are required in this field.
Precautions regarding AVF creation
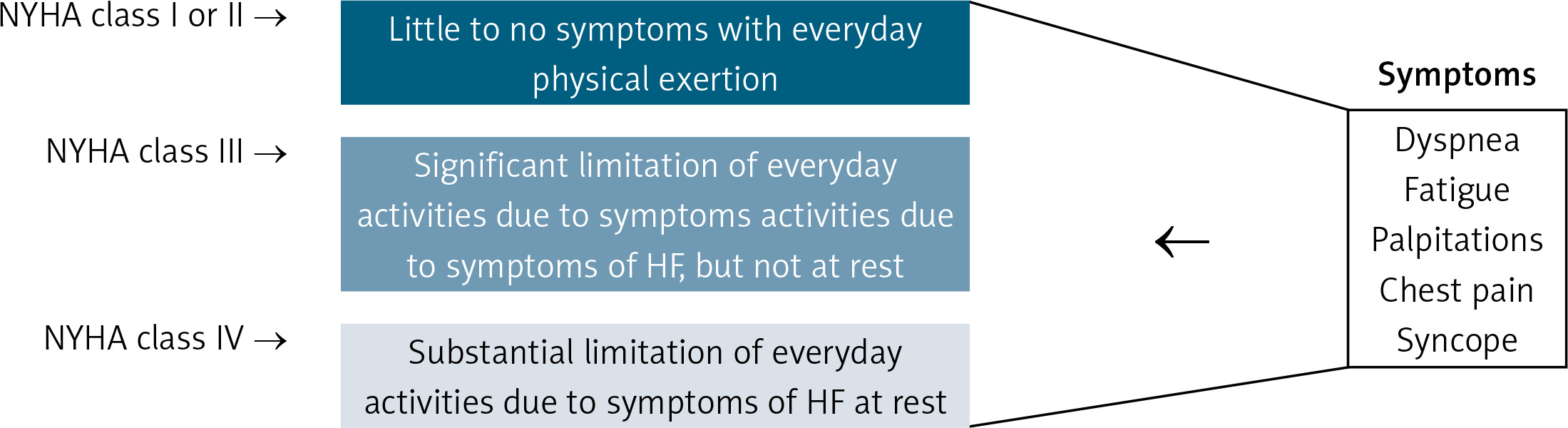
Before AVF creation, careful examination of the cardiovascular system is necessary and should guide the AVF creation strategy in high-risk patients. For patients with HF of New York Heart Association (NYHA) class I or II, the creation of a peripheral AVF (radiocephalic) due to an initial smaller flow rate has been recommended [58]. However, AVF creation for patients with an NYHA class III should be avoided in favor of peritoneal dialysis, and in patients with NYHA class IV, AVF creation is contraindicated [58]. Any unused AVFs should be ligated upon evidence of cardiovascular deterioration [59]. The relative symptoms are dyspnea, fatigue, palpitations, chest pain, and syncope. In certain cases, with NYHA III and contraindication to peritoneal dialysis, forearm AVF may be considered based on the severity of systolic and diastolic LV dysfunction (Figure 5) [58].
Generally, we avoid creating an AVF if the LVEF is below 30%. In the presence of the aforementioned cardiovascular co-morbidity, a forearm AVF (Brescia-Cimino) should be preferred. If this is not feasible, an upper arm AVF (brachiocephalic or a brachiobasilic), with a small anastomosis (e.g. 3 mm vs. the normal 6 mm) may be selected. However, we must keep in mind that despite the initial low flow, it can worsen over time, so close monitoring is essential. A tapered graft (e.g. 4–7 mm) may also be used with the arteriotomy restricted to 4 mm. Of course, endovascular AVF is another new option, as it is generally combined with lower flows. These approaches must be balanced against other dialysis options such as peritoneal dialysis or a permanent catheter and should be implemented if these alternative options are unfeasible or not indicated [37, 40].
Conclusions
AVFs remain the procedure of first choice for vascular access and are well tolerated by most patients. Nevertheless, their deleterious effects on pre-existing cardiovascular disease or in healthy individuals in the long term due to increased flow should not be underestimated. Consequently, cardiology consultation is required before AVF creation. Patients with an access flow greater than 1500 ml/min require close monitoring. Further increase of flow, worsening of echocardiographic findings, or onset of cardiac symptoms necessitates a flow-reduction procedure or ligation of the AVF.