
Atrial fibrillation (AF) is the most common cardiac arrhythmia with the prevalence of up to 2% worldwide, and by 2030, it is expected to affect approximately 14 to 17 million individuals within the European Union [1, 2]. It is considered a major risk factor for thrombus formation, particularly in the left atrium (LA) and its appendage (LAA), due to the irregular atrial contractions in AF. These contractions cause blood stasis, which increases the likelihood of clot formation and can lead to severe thromboembolic complications such as stroke [3]. AF-related systemic thromboembolism is responsible for 20–30% of all ischemic strokes and 10% of strokes of unknown origin [4].
Echocardiography, especially transesophageal echocardiography (TEE), is widely used to detect left atrial thrombi, as it provides detailed imaging of the left heart structures, making thrombi in the left atrium more commonly identified. However, right atrial thrombi are less frequently detected and can be underdiagnosed, as the focus is often on the left heart chambers. Although rare, simultaneous thrombi in both the left and right atria present a significant clinical challenge due to the risk of both systemic and pulmonary embolization.
This case report presents a patient with atrial fibrillation who developed simultaneous left and right atrial thrombi, highlighting the need for comprehensive imaging and multidisciplinary management to reduce the risk of embolic events. A 72-year-old female patient with a known history of AF, anticoagulated with dabigatran, presented to the neurology clinic with dysdiadochokinesia and apraxia of the right upper limb. A brain computed tomography (CT) scan revealed multiple infarcts in the middle and posterior cerebral artery distribution bilaterally, as well as in the left cerebellum, suggestive of a cardioembolic source. TEE was performed, revealing a large thrombus originating in the left atrium and extending through the mitral valve into the left ventricle (Figures 1 A–F). Given the patient’s embolic presentation and the size of the thrombus, surgical intervention was deemed necessary. The patient underwent a median sternotomy for thrombus removal. Intraoperative TEE revealed additional thrombi on the interatrial septum and within the right atrium (Figures 2 A, B). No atrial septal defect (ASD) or significant patent foramen ovale (PFO) was found to explain the right atrial thrombus, raising the possibility of a primary right atrial thrombus. Consequently, a right atriotomy was performed, and all thrombi were successfully removed through the interatrial septum (Figures 3 A–D). Additionally, the left atrial appendage (LAA) was amputated to reduce the risk of future thrombus formation. The intraoperative period was uneventful, with no embolic events. The patient had a smooth and uncomplicated postoperative recovery. Given the presence of thrombi despite anticoagulation with dabigatran, the patient’s anticoagulation therapy was switched to phenprocoumon, a vitamin K antagonist. She was discharged in stable condition on postoperative day 10. Follow-up echocardiographic evaluations at 6 weeks, 6 months, and 1 year revealed no recurrence of intracardiac thrombi. The patient remained in good health, with no further embolic events.
Figure 1
Preoperative transesophageal echocardiography demonstrating the presence of a thrombus in the left atrium. A–C – the thrombus attached to the left atrial wall from different angles (arrow), D – 3D echocardiographic reconstruction clearly illustrates the localization of the thrombus (arrow), E, F – presence of thrombotic material in the right atrium (arrow)
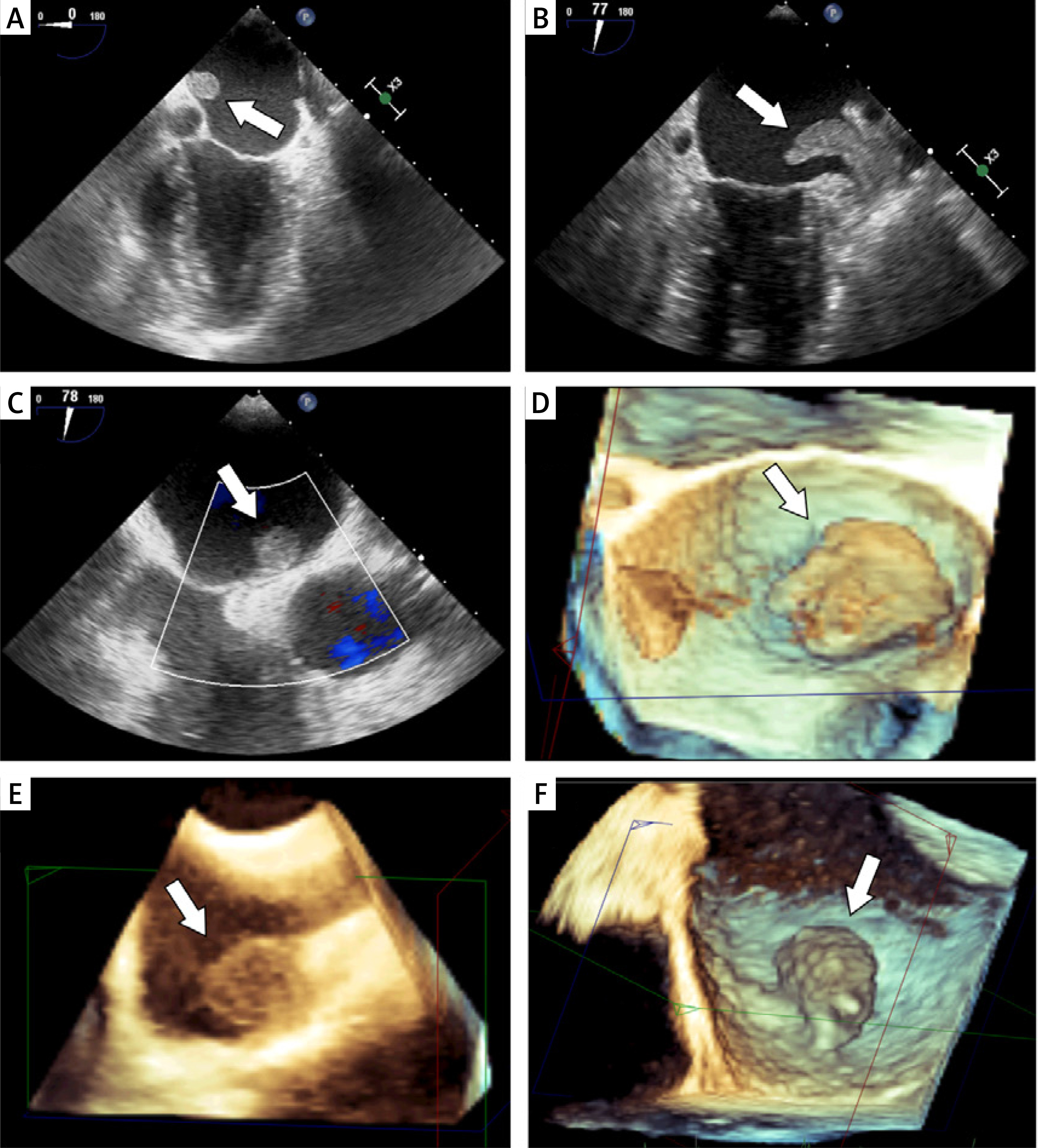
Figure 2
Intraoperative image showing the thrombus in the left atrium extending over the mitral valve (arrow). A – Actual intraoperative photograph. B – Schematic representation of the operative field
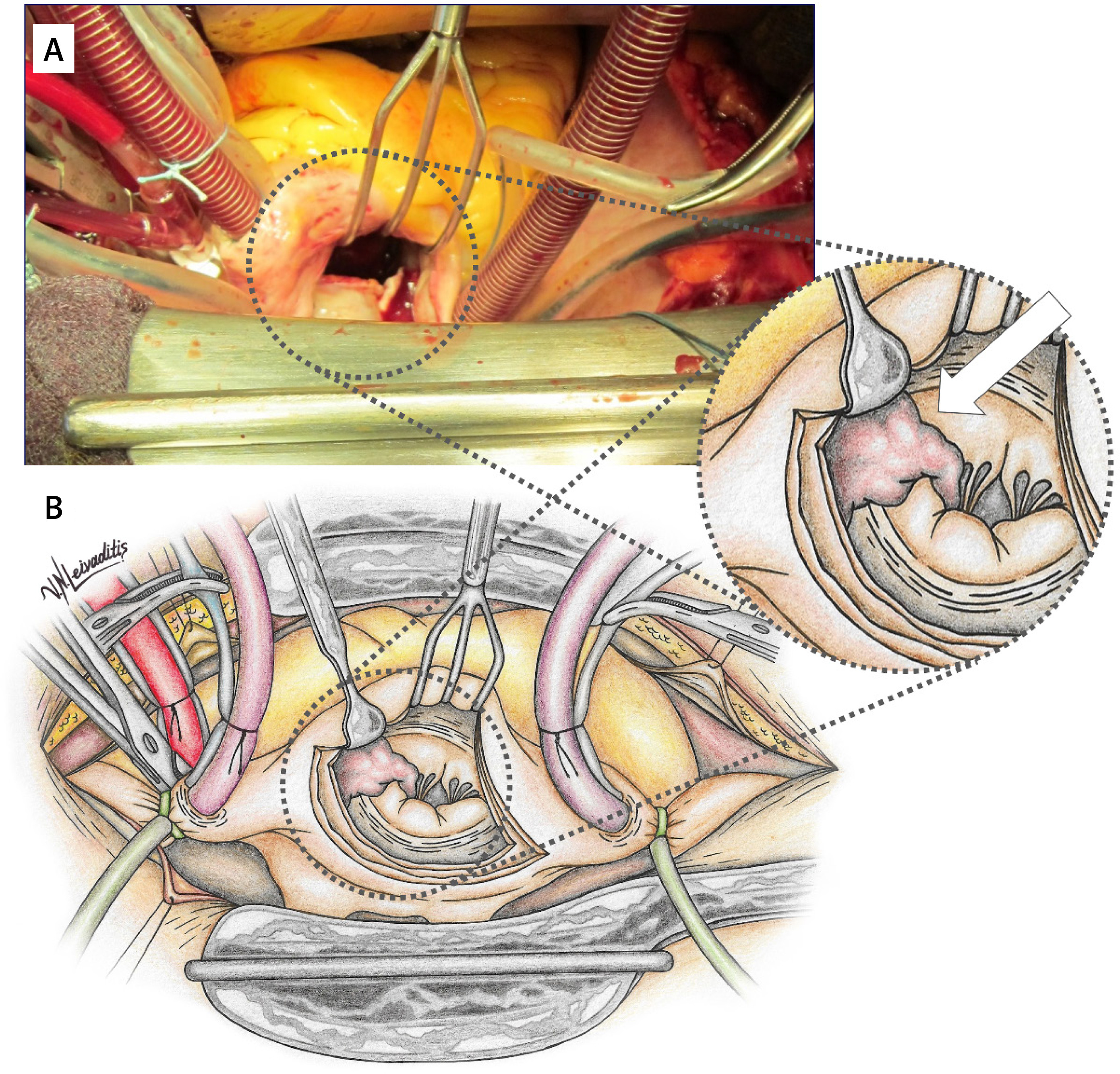
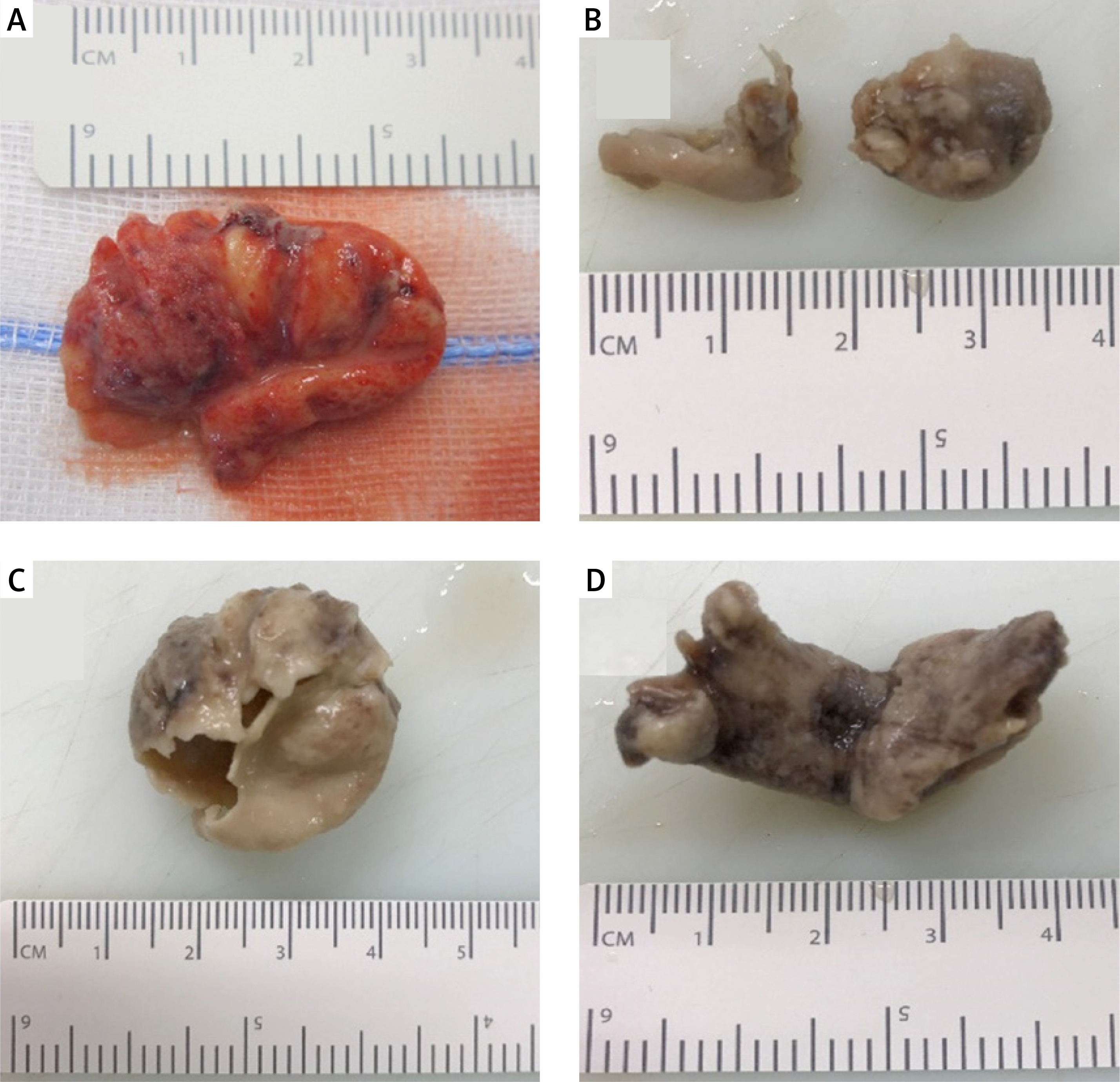
Figure 3
Resected thrombotic material. A, B – the thrombus removed from the left atrium, C, D – the thrombus removed from the right atrium
This case of simultaneous left and right atrial thrombi in a patient with AF emphasizes the need for comprehensive cardiac imaging and vigilant management of thromboembolic risk. While LA thrombus formation, particularly in the LAA, is well documented in patients with AF, thrombi in the right atrium (RA) are significantly less common. The simultaneous presence of left and right atrial thrombi is exceedingly rare, as highlighted by Cresti et al., who reported a 0.75% incidence of right atrial thrombi compared to 10.3% in the left atrium among patients with atrial fibrillation [2]. According to Suratkal et al., the occurrence of RA thrombus in patients with AF varies between 3% and 6% [5]. The low incidence of right atrial thrombi may be attributed not only to anatomical factors but also to underdiagnosis, as the standard routine practice often focuses on the left heart chambers during echocardiographic evaluation. Our case further demonstrates the need for a thorough evaluation of both atria, especially in patients presenting with cardioembolic events. While left atrial thrombi are more commonly detected, the possibility of simultaneous thrombi in both atria warrants a systematic and comprehensive echocardiographic evaluation. Expanding routine diagnostic protocols to give equal attention to the right atrium could help mitigate the risk of underdiagnosis and improve clinical outcomes. Even though it is more challenging to detect RA thrombus because of the anatomical location and trabeculated shape of the RA, a thorough assessment for potential right atrial thrombus using transthoracic echocardiography (TTE) with advanced techniques, such as the right parasternal approach, and TEE, the gold standard for right atrial evaluation, is essential in patients with atrial fibrillation [6]. While TTE is often used as the first-line imaging modality, TEE offers superior sensitivity and specificity, especially for detecting thrombi in the left atrium, left atrial appendage, and less commonly evaluated areas such as the right atrium. This highlights the importance of incorporating TEE into the diagnostic pathway for comprehensive assessment in patients with atrial fibrillation and thromboembolic risk. As seen in our case, the recognition of preoperative undetectable RA thrombus with intraoperative TEE demonstrates the importance of evaluating both the left and right atria, especially in patients with embolic events, as simultaneous thrombi present a more complex and dangerous clinical situation. The absence of an ASD or PFO in this patient further complicates the etiology of the right atrial thrombus, suggesting that the formation of clots in the RA might occur independently in some cases of AF. This raises the possibility that stasis and atrial dysfunction in AF could equally affect both atria under certain conditions, despite the lower incidence of right atrial thrombi. Therefore, the reason for the low incidence of RA thrombus may not be solely due to the larger right atrial appendage (RAA) neck widths and the lack of structural remodeling in the RAA, as some have suggested, but because RA was not examined routinely during echocardiographic examination [4]. The decision to perform the right atriotomy and left atrial appendage amputation indicates the necessity of aggressive intervention in such cases to prevent further embolic events, including potential systemic and pulmonary emboli. Another crucial aspect of this case is the anticoagulation strategy. Despite the patient being on dabigatran, thrombus formation still occurred, which prompted a switch to phenprocoumon, a vitamin K antagonist, postoperatively. Phenprocoumon was chosen due to its longer half-life and consistent anticoagulant effect, which may provide enhanced thrombus prevention in patients with high embolic risk. Furthermore, its effectiveness can be closely monitored through routine measurements of the international normalized ratio (INR), providing a tailored approach to anticoagulation management in complex cases like this one. This highlights the need for careful re-evaluation of anticoagulation efficacy in patients with recurrent or persistent thrombi despite appropriate therapy. This case demonstrates the importance of personalized treatment plans in AF patients, particularly those at high risk for thromboembolic complications, and demonstrates the critical role of interdisciplinary collaboration between cardiology, neurology, and cardiothoracic surgery teams in managing complex cases like this one.
In conclusion, this case reinforces the necessity of thorough echocardiographic assessment in patients with cardioembolic events and AF, including both the left and right heart chambers. Simultaneous thrombus formation in both atria is rare but carries significant risks, necessitating prompt and coordinated multidisciplinary intervention to prevent adverse outcomes. This case underlines the importance of comprehensive echocardiographic evaluation in patients with atrial fibrillation and cardioembolic events, highlighting the need to assess both the left and right atria for thrombi. The simultaneous presence of left and right atrial thrombi, though rare, poses a significant risk of systemic and pulmonary embolism. It also demonstrates the necessity of personalized anticoagulation strategies, as standard therapy with dabigatran was insufficient to prevent thrombus formation in this patient. The switch to phenprocoumon postoperatively highlights the importance of re-evaluating anticoagulation efficacy in high-risk cases. Additionally, the case emphasizes the value of coordinated multidisciplinary care across specialties – cardiology, neurology, and cardiothoracic surgery – to ensure optimal diagnosis, treatment, and prevention of complications in complex thromboembolic conditions.