Introduction
In recent years, patients suffering an acute myocardial infarction (AMI) have had improved survival due to reperfusion therapies, which has in turn also led to an increased number of patients living with heart failure (HF) [1, 2]. HF is well established as a common complication of AMI, with up to a 50% of HF incidence in patients post-MI [3]. HF in AMI patients has been associated with poor prognosis and a three to four times increase in mortality during the index AMI hospitalization and even after discharge [4, 5]. Given the high incidence of morbidity and mortality from post-MI HF, a strong understanding of risk factors for HF in AMI survivors is essential for implementing proper clinical care for co-management of conditions in AMI survivors.
Chronic obstructive pulmonary disease (COPD) has been established as a risk factor for cardiovascular diseases, related hospitalizations and mortality, and is associated with worse outcomes in patients with chronic HF [6–8]. Patients with COPD who have an AMI are less aggressively treated than those without COPD, which result in increased in-hospital mortality as well as long-term mortality [9–11]. Prior research revealed a higher risk of subsequent new-onset HF after MI in COPD patients [12]. It was also established that COPD, in addition to predicting long-term mortality in patients with AMI, is also a confounding factor for the diagnosis of HF [13]. Only a few studies addressed HF hospitalisations after AMI in patients with COPD, and these analyses are either less contemporary, utilized smaller sample sizes, studied patients with existing HF or left ventricular systolic dysfunction, or studied patients predominantly from Europe [12, 14]. There is a dearth of recent, population-level research addressing differences in HF hospitalizations based on COPD status among all-comers cohort of AMI survivors in the United States.
Therefore, the aim of the current paper is to evaluate the impact of COPD on the 6-month HF hospitalization rate in AMI survivors using a United States population representative national database.
Material and methods
Data source
In this retrospective observational study, data were collected from the publicly available 2014 US Nationwide Readmissions Database (NRD). The NRD is part of the Healthcare Cost and Utilization Project (HCUP) that is sponsored by the Agency for Healthcare Research and Quality (AHRQ) and is a database of all-payer hospital inpatient stays that can be used to generate national estimates of readmissions [15]. The NRD is drawn from HCUP State Inpatient Databases, which contain verified patient linkage numbers that can be used to track a person across readmissions while maintaining privacy. Unweighted, the 2014 NRD contains data from approximately 15 million discharges from 22 geographically dispersed states accounting for 51.2% of the total US resident population and 49.3% of all hospitalizations. Weighted, it estimates roughly 35 million discharges.
Patient population and baseline characteristics
The study sample included all patients ≥ 18 years who were discharged alive, and who are therefore at risk of readmission, between January and June 2014 with a primary discharge diagnosis of an AMI (International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) codes 410.x1). NRD 2014 was utilized because it is the latest yearly dataset that allows ICD-9 based analysis which was previously validated to study HF outcomes [16, 17]. This time period was chosen so that our study patients could be tracked until the end of 2014 for any HF hospitalization, thereby allowing for analysis of 6-month readmissions. Patients with cardiogenic shock were excluded as they represent a complex phenotype associated with heightened acute and post-discharge mortality [17]. COPD was defined as the presence of chronic bronchitis, emphysema, or chronic obstructive asthma. Similar methodology was utilized in prior studies [10, 18].
Baseline patient characteristics identified were age, sex, insurance status, median household income, AMI type, and comorbidities including anemia, connective tissue disease, carotid artery disease, prior MI, prior coronary revascularization, prior ischemic cerebrovascular event, atrial fibrillation, coronary artery disease, cancer, chronic lung disease, smoking, depression, drug abuse, diabetes mellitus, hypertension, hypothyroidism, fluid-electrolyte imbalances, liver disease, obesity, peripheral vascular disease, pulmonary circulation disorders, chronic kidney disease, and HF during the index admission, discharge disposition, in-hospital outcomes including percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), any mechanical revascularization, and acute kidney injury. Hospital characteristics (bed-size and teaching status) were also identified. Elixhauser comorbidity data were extracted from the NRD.
Study outcomes
The primary outcomes of this study were crude and risk-adjusted differences in the rate of HF hospitalization within 6 months (180 days) from discharge after an AMI in patients with and without COPD. In patients with recurrent HF readmissions, only the first HF hospitalization was counted towards the outcome. A composite outcome of 6-month HF readmission or all-cause mortality during a non-HF related admission was studied in the overall cohort and certain subgroups. The primary outcome was evaluated in subgroups of pre-specified cardiovascular risk factors (age, sex, hypertension, dyslipidemia, obesity, atrial fibrillation, chronic kidney disease), AMI type, revascularization status, and in patients with and without HF at the time of index AMI. Secondary outcomes were crude rates of fatal HF readmission and the composite of in-hospital HF during the index admission and a 6-month readmission for HF between patients with and without COPD. HF hospitalizations were identified as those that had a primary discharge diagnosis of HF within 180 days from discharge [15]. Fatal HF hospitalization was defined as a readmission primarily for HF during which the patient died.
Statistical analysis
The NRD has a complex semi-random multistage sampling survey design and survey design-based statistical tests using weighted data were utilized for all analyses. Categorical variables are expressed as percentages, and continuous variables as mean ± standard deviation (SD). Baseline patient characteristics, comorbidities, procedures, hospital characteristics, and outcomes were compared between patients with and without COPD, and in patients with and without a 180-day HF readmission using the Rao-Scott χ2 test for categorical variables and student t-test for continuous variables.
A multivariable logistic regression model (designed to test for 95% confidence intervals (CIs) and a two-sided p-value threshold of < 0.05) and accounting for the sample design of the NRD was created to identify risk-adjusted differences in the rate of the primary outcome between patients with and without COPD. The regression model included all the variables which achieved a p-value < 0.2 in unadjusted analysis stratified by the primary outcome. Results of the logistic regression analyses were reported as odds ratios (ORs) and 95% CIs. The regression model had a c-statistic of 0.8 indicating a strong model [19]. We retained this regression model to also analyze the impact of COPD on the primary outcome in pre-specified subgroups of age (< 65 and ≥ 65 years), sex, presence of diabetes mellitus, atrial fibrillation, dyslipidemia, chronic kidney disease, hypertension, HF at time of index AMI, obesity, AMI type, and coronary revascularization status during the AMI.
To partially account for the competing risk of death on the occurrence of the primary HF outcomes, we performed a sensitivity analysis excluding patients who died during a non-HF admission during the 6-month follow-up period before the occurrence of a HF admission, and also evaluated the impact of COPD on a composite outcome of 6-month HF readmission or all-cause mortality during a non-HF admission. Less than 0.5% of data were missing for the variables: insurance status, median household income and discharge disposition. Missing values were replaced with the dominant categories. All analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). The two-tailed significance level was set at p < 0.05.
Results
Baseline characteristics
Our study sample consisted of 237,549 AMI survivors. The mean age of the study sample was 66.9 ±13.9 years and 37.9% of the study sample were female. Of these, 41,708 (17.5%) patients had COPD. Baseline characteristics stratified by COPD status are presented in Table I. Compared to patients without COPD, patients with COPD were older, more likely female, and had a significantly higher prevalence of smoking, obesity, hypertension, atrial fibrillation, atherosclerotic vascular disease, diabetes mellitus, anemia, cancer, chronic kidney disease, connective tissue diseases, coagulopathy, depression, hypothyroidism, liver disease, and fluid and electrolyte disorders (p < 0.001).
Table I
Differences in the baseline characteristics, comorbidities, in-hospital complications, and procedural utilization among acute myocardial infarction survivors
[i] STEMI – ST-elevation myocardial infarction, NSTEMI – non-ST elevation myocardial infarction, COPD – chronic obstructive pulmonary disease, HF – heart failure, TIA – transient ischemic attack, CABG – coronary artery bypass graft, AKI – acute kidney injury, PCI – percutaneous coronary intervention, SD – standard deviation.
Alternatively, COPD patients were significantly less likely to have dyslipidemia and less likely to be discharged home compared to patients without COPD. The majority of patients had a NSTEMI (71.9%), and this presentation was more common among patients with COPD than patients without COPD (82.1% vs. 69.7%, p < 0.001). Patients with COPD were less likely to undergo mechanical coronary revascularization during the index AMI admission (50.1% vs. 64.2%, p < 0.001), including PCI (39.8% vs. 55.9%, p < 0.001), however were more likely to undergo CABG (11.0% vs. 9.0%, p < 0.001). HF was present in 29.2% of all patients during the index admission, and was significantly more prevalent in patients with COPD (47.0% vs. 25.5%, p < 0.001).
Outcomes
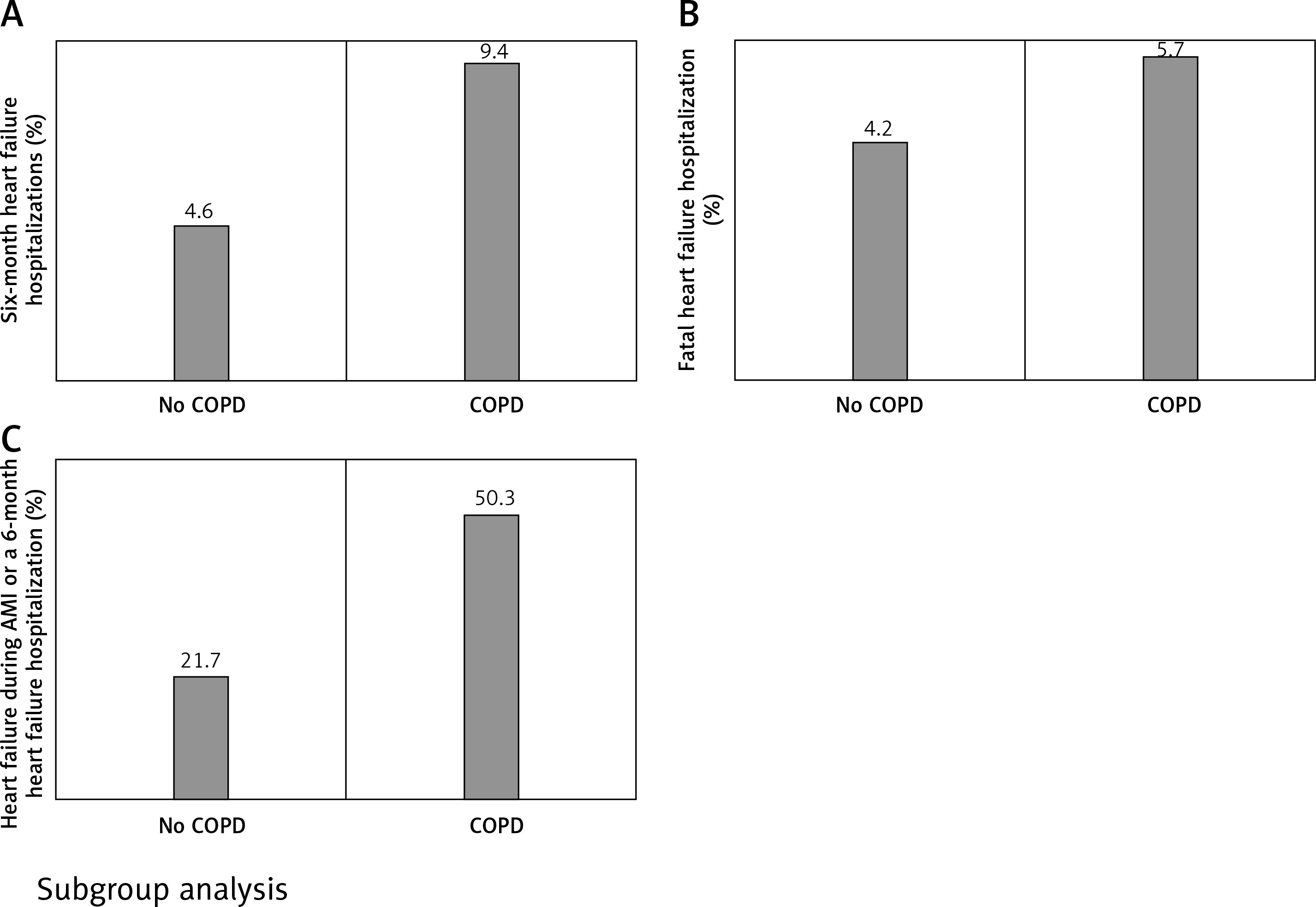
Overall, 12,934 (5.4%) patients were readmitted within 6 months after discharge for HF and 599 patients (0.3%) died during the readmission. Patients with COPD had a 114% higher rate of 6-month HF hospitalization compared to those without COPD (9.4% vs. 4.6%, OR = 2.14, 95% CI: 2.01–2.29; p < 0.001), a 181% higher rate of fatal HF hospitalization (0.5% vs. 0.2%, OR = 2.81, 95% CI: 2.09–3.79; p < 0.001), and a 161% higher rate of composite outcome of HF during index admission or a 6-month HF readmission (49% vs. 26.9%, OR = 2.61, 95% CI: 2.51–2.71; p < 0.001) (Table II). Among patients who had a 6-month HF readmission, COPD patients had a significantly higher prevalence of fatal HF compared to patients without COPD (5.7% vs. 4.2%, OR = 1.40, 95% CI: 1.04–1.89; p < 0.001) (Figure 1).
Table II
Impact of COPD on heart failure outcomes
Figure 1
Differences in heart failure outcomes according to chronic obstructive pulmonary disease status. Patients with any chronic obstructive pulmonary disease had significantly higher rates of 6-month heart failure hospitalizations (A), fatal heart failure hospitalizations (B), and the composite outcome of either in-hospital heart failure or 6-month heart failure hospitalization (C) compared with patients without any chronic obstructive pulmonary disease
Significant differences in baseline characteristics were observed for patients who had the primary outcome compared with those who did not. In the risk adjusted multivariable analysis, patients with COPD had 39% higher odds of a 6-month HF admission compared with patients without COPD (OR = 1.39; 95% CI: 1.30–1.49). The composite outcome of 6-month HF readmission or all-cause mortality during a non-HF admission occurred in 17,306 (7.3%) patients, at a 125% higher rate with COPD than without (12.8% vs. 6.1%; OR = 2.25, 95% CI: 2.12–2.39; p < 0.001). After risk adjustment, patients with COPD had 48% higher odds of the composite outcome compared with patients without COPD (OR = 1.48; 95% CI: 1.39–1.58). In a sensitivity analysis excluding patients who died during a non-HF admission during the 6-month follow-up period before the occurrence of a HF admission (N = 4,382, 1.8%), results for the primary outcome were consistent with the main analysis and patients with COPD had 42% higher odds of a 6-month HF admission compared with patients without COPD (OR = 1.42; 95% CI: 1.32–1.53).
Subgroup analysis
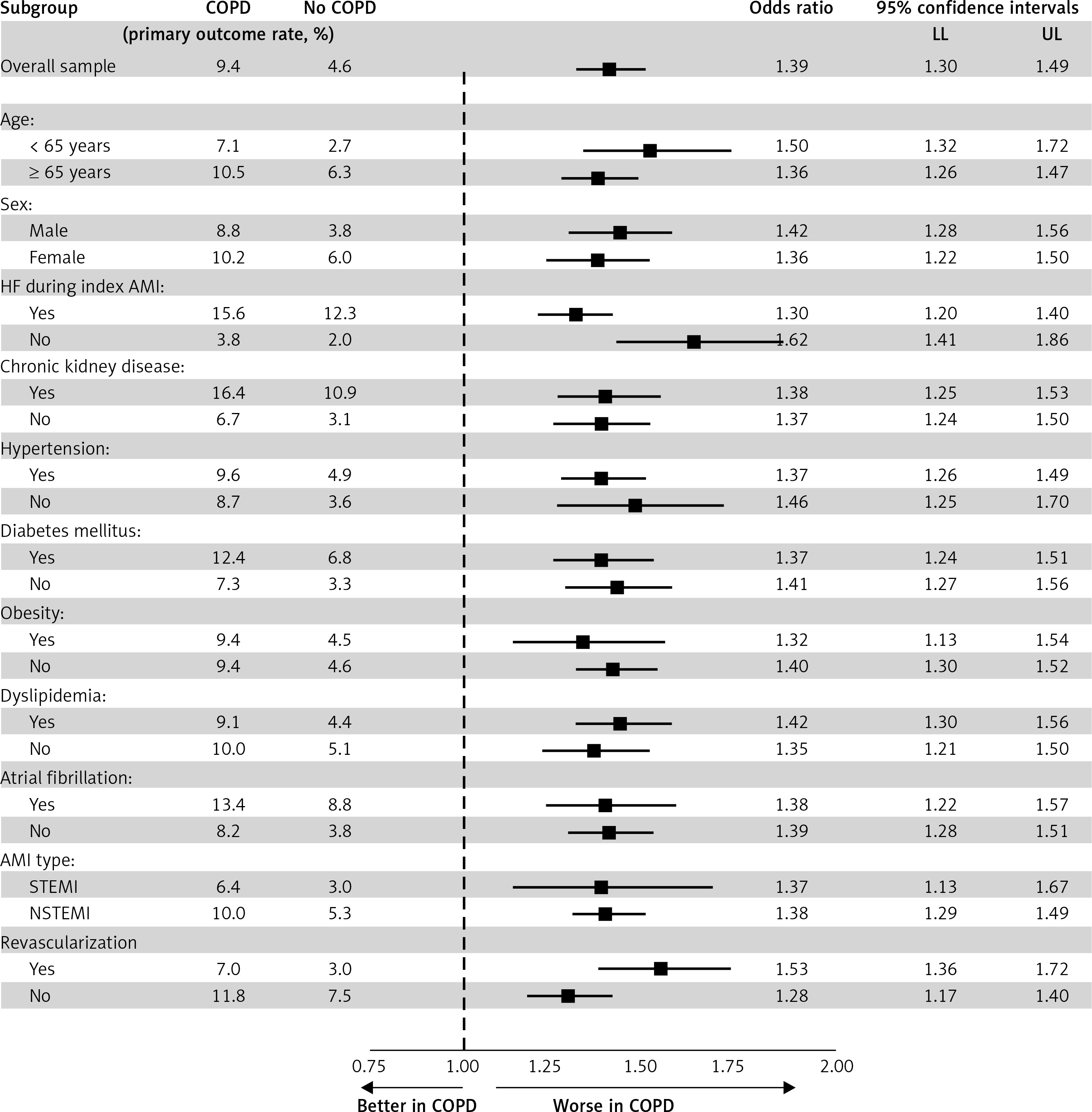
The impact of COPD status on the risk of the primary outcome in clinically relevant subgroups which could impact the occurrence of HF admission are presented in Figure 2. The higher HF readmission risk with COPD was consistent in younger and older patients, in males and females, in STEMI and NSTEMI, in revascularized and medically treated patients, in patients with and without HF during index admission, and across categories of important cardiovascular and HF risk factors (Figure 2).
Figure 2
Sub-group analyses and Forest plots for 6-month heart failure readmission outcome. Among survivors of an acute myocardial infarction, patients with COPD had a higher risk of 6-month heart failure readmission across all the subgroups studied
COPD – chronic obstructive pulmonary disease, HF – heart failure, AMI – acute myocardial infarction, LL – lower confidence interval, UL – upper confidence interval.
Discussion
The aim of our study was to elucidate differences across COPD status in HF hospitalization outcomes in a United States nationally-representative population of all-comers AMI survivors. We report several important findings regarding the influence of COPD on HF outcomes following an AMI, which have significant clinical relevance. AMI survivors with COPD had a significantly higher risk of HF requiring hospitalization and fatal HF within the following 6-month period compared to those without COPD. Patients with COPD had worse baseline characteristics, in-hospital outcomes, and lower revascularization rates, but the increased HF hospitalization risk in COPD patients persisted (although attenuated) even after adjusting for these differences. The higher HF readmission risk in COPD patients was present in both NSTEMI and STEMI subtypes, and higher across categories of age, sex and several cardiovascular risk factors. Our study findings confirm findings from prior reports and also suggest the need for closer follow-up and careful monitoring for the development of HF in COPD patients with an AMI to prevent the occurrence of HF requiring hospitalization.
COPD is a risk factor for cardiovascular diseases and is associated with increased cardiovascular-related hospitalizations and death from cardiovascular events [20]. COPD and cardiovascular diseases share several risk factors such as advanced age and cigarette smoking among others. Besides shared risk factors, COPD-related factors, such as systemic inflammation and hypoxia, underlie the pathophysiological interaction between COPD and AMI [14]. In addition to these similarities in risk profiles and pathophysiological milieu, patients with underlying COPD are less aggressively treated during an AMI. These factors impact the outcomes of AMI during the in-hospital and the follow-up period and increase the risk of AMI-related complications, particularly HF [9, 14]. Stefan et al. retrospectively analyzed 6,290 patients with AMI between years 1997 and 2007 (17% with COPD) and found that patients with COPD had a 59% increased risk of HF during index hospitalization compared to those without COPD (OR = 1.59, 95% CI: 1.37–1.83) [11]. Similar findings of higher HF during the AMI in COPD patients (47.0%) compared with those without (25.5%) were observed in our study.
Although it is known that COPD patients have an increased risk of HF development, only a few studies addressed the impact of COPD on subsequent HF hospitalization risk following an AMI [14]. In a sub-study of the Valsartan in Acute Myocardial Infarction Trial (VALIANT) that included 14,703 AMI patients with either HF or left ventricular systolic dysfunction and published in 2003, 8.6% of patients had COPD (n = 1,258) [21]. The authors reported that the adjusted risk of HF hospitalization at 25-month follow-up was 19% higher in patients with COPD (hazard ratio = 1.19, 95% CI: 1.05–1.34). In another study of 81,191 patients with AMI enrolled between years 2005 and 2010 into the Swedish SWEDEHEART registry (6% with COPD), Andell et al. showed that after adjustment for potential confounders, including comorbidities and treatment, patients with COPD had a 35% higher rate of new-onset HF (hazard ratio = 1.35, 95% CI: 1.24–1.47) [12]. These studies also reported that patients with COPD frequently had an atypical presentation, less often underwent revascularization and less often received guideline-recommended secondary preventive medications of established benefit in AMI [11, 12, 21]. Differences in in-hospital management in patients with COPD compared with their non-COPD counterparts were also evident in our study.
Our study findings corroborate the currently available data of the association between COPD and HF in patients with AMI. Prior research has established that COPD is an independent predictor of increased mortality following an AMI [14, 20]. Despite this increased mortality risk for COPD (which competes with the risk of HF admissions), patients with COPD still have a substantially higher HF hospitalization risk following an AMI, and this was independent of the presence of HF at the time of the AMI as seen in our study. Our study evaluated more contemporary data and evaluated a larger nationally representative population of all-comers AMI survivors and extends previously reported findings to a more contemporary dataset suggesting that changes in management that could have occurred over the years did not greatly improve post-MI HF outcomes in patients with COPD. Furthermore, we also studied the impact of COPD on HF hospitalizations across categories of several important cardiovascular and HF risk factors and report that the poor prognostic impact of COPD was consistent across the categories of cardiovascular risk factors and the effect size was generally similar.
The current study underscores 1) the importance of improving AMI care in patients with COPD; and 2) highlights the necessity of early recognition of HF in COPD patients and clinical co-management of care. COPD patients typically present with atypical AMI symptoms (most frequently dyspnea) and the consequence of misleading symptoms is delayed diagnosis, lower rates of immediate intervention, and the possibility of subsequent greater infarct size and/or worse prognosis [12, 14]. In addition, the utilization of certain pharmacologic therapies, particularly β-blockers with coexisting COPD has been a subject of debate in clinical practice and these agents are less frequently prescribed in patients with COPD despite the evident survival benefit [9, 14]. In patients with COPD, optimal management strategies at the time of the AMI and appropriate guideline directed preventative therapies at discharge should be utilized at similar rates compared to patients without COPD whenever appropriate.
The symptoms and subjective signs, such as dyspnea and fatigue, of COPD and HF are often very similar, which can make clinical differentiation challenging especially with HF with preserved ejection fraction. COPD was recognized as a confounding factor for the diagnosis of HF following an AMI [22]. Studies report a very high prevalence of unrecognized HF (up to 20%) in COPD patients, revealing a critical area for intervention and calling attention to the critical need for multidisciplinary coordination across specialties in high-risk populations [22]. Given the substantially worse prognosis associated with post-MI HF, evidence-based monitoring protocols for HF in COPD patients, optimal preventive therapies, and careful co-management by internists, pulmonologists, and cardiologists are essential in this high-risk population.
The current study relies on inpatient claims-based data that have inherent limitations. Due to the inpatient nature of the data, we are unable to capture outpatient information that has relevance and may lead to some selection bias. Because the primary outcome of our study was the difference in hospitalization for HF, patients who had outpatient HF diagnoses may have been missed from the analysis. ICD-9-CM codes used to extract data are prone to coding errors; however, codes for HF are very commonly used and therefore are less prone to misclassification. More importantly, the NRD does not include data on clinically relevant parameters like medication use and dosages during and after AMI, coronary anatomy, left ventricular ejection fraction, race/ethnicity, spirometry, or the severity of AMI or HF, thereby preventing us from accounting for these factors in our analysis. In addition, we could not estimate the severity of COPD based on information available in the NRD. Despite the above noteworthy limitations, our study provides important estimates of the problem and the large sample size in our study lends credence to its findings.
In conclusion, in this study of a large United States national representative sample of all-comers AMI survivors, 1 in 6 patients had COPD and it was associated with an increased risk of subsequent HF hospitalizations in the 6 months following an AMI even after adjusting for differences in comorbidities and in-hospital treatments. These findings underscore the importance of improving AMI care in patients with COPD and highlight the need for closer follow-up, careful monitoring for the development of HF, and co-management of COPD patients following an AMI to prevent the onset of HF requiring hospitalization.