Introduction
Cardiovascular disease remains the leading cause of death worldwide, with acute myocardial infarction (AMI) representing a major contributor to this burden [1]. Recent evidence indicates that the global prevalence of MI is approximately 3.8% among individuals younger than 60 years and increases to nearly 9.5% in those aged 60 years or older [2–4]. In the United States and Europe combined, more than two million individuals experience a MI annually, emphasising its substantial clinical and public health impact [5, 6]. Despite major advances in reperfusion strategies and contemporary pharmacotherapy, survivors of AMI continue to face elevated risks of recurrent infarction, Heart failure (HF), and long-term mortality, highlighting the importance of continued long-term secondary prevention [7–10].
B-blockers have traditionally been continued indefinitely after MI, supported by early landmark trials demonstrating significant reductions in mortality and recurrent ischaemic events, particularly among patients with reduced left ventricular ejection fraction (LVEF) or overt HF [11]. Accordingly, long-term oral β-blocker therapy remains a class I recommendation for patients with HF, LV dysfunction, or ventricular arrhythmias after ST elevation myocardial infarction (STEMI) in both AHA/ACC and ESC guidelines [12, 13]. However, the clinical context in which these trials were conducted differs markedly from current practice. In recent decades, improvements in early reperfusion, most notably with routine use of percutaneous coronary intervention (PCI), alongside the adoption of antiplatelet therapy, high-intensity statins, and comprehensive guideline-directed medical therapy, have substantially reduced infarct size and improved early outcomes [14–16]. As a result, a growing proportion of patients now recover from AMI with preserved or mildly reduced LVEF rather than significant systolic dysfunction [17].
This shift in clinical presentation has made the clinical value of long-term β-blockers for patients with preserved LVEF less clear. Recent randomised trials evaluating β-blocker therapy in individuals with LVEF of at least 40% have produced inconsistent findings, raising doubts about whether routine, indefinite treatment continues to provide meaningful reductions in mortality or major cardiovascular events [18, 19]. Consequently, reevaluating the role of β-blockers in this evolving clinical context has become essential to ensure that long-term secondary prevention strategies remain evidence based and aligned with contemporary patterns of myocardial recovery.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [20]. The study protocol was prospectively registered with PROSPERO (registration number: CRD420251229617). Ethical approval was not required because all the included studies were publicly available and contained only de-identified patient data.
Data sources and search strategy
Two independent researchers (EZ and MA) conducted a comprehensive literature search across the PubMed/Medline, Google Scholar, and Cochrane Library databases. The complete search strategy is provided in Supplementary Table SI. In addition, reference lists of relevant review articles and prior meta-analyses were manually screened to ensure that no eligible studies were missed.
Study selection and eligibility criteria
All records identified through the electronic search were imported into Rayyan (https://new.rayyan.ai/; accessed on 14 October 2025) for screening. Duplicate references were identified and removed. Two reviewers (HS and YM) independently screened titles and abstracts to determine potential eligibility, after which the full texts of relevant articles were assessed in detail. Discrepancies between reviewers were resolved through consultation with a third investigator (EZ).
Studies were eligible for inclusion if they met the following criteria: (1) randomised controlled trial design; (2) included adult patients with a documented history of MI; (3) LVEF ≥ 40%; and (4) comparison of β-blocker therapy with a control group receiving no β-blocker therapy.
Studies were excluded if they (1) included patients with reduced LVEF (< 40%); (2) employed non-randomised designs such as observational cohorts, retrospective analyses, pooled post-hoc studies, case reports, conference abstracts, or letters; (3) involved animal models or healthy volunteers; or (4) were published in languages other than English.
Data extraction, outcomes, and quality assessment
Data extraction was performed independently by two reviewers (RS and HM) using a standardised approach. For each included trial, study name, publication year, follow-up duration, sample size, and baseline demographic characteristics were extracted. Clinical variables relevant to the population and intervention, such as LVEF, previous PCI, previous history of diabetes, hypertension, or smoking were also extracted. Outcome data were obtained directly from the published trials without modification.
The primary endpoint of this meta-analysis was a composite of all-cause mortality and major adverse cardiovascular events (MACE) (defined as a composite cardiac death, MI, or hospitalisation due to HF). Secondary endpoints included cardiovascular mortality, recurrent MI, hospitalisation for HF, and stroke.
Assessment of methodological quality was performed using the Cochrane Risk of Bias 2.0 tool, which evaluates randomised trials across five domains: randomisation process, deviations from intended interventions, completeness of outcome data, measurement of outcomes, and selection of reported results [21]. Each study was assigned a judgement of low risk, some concerns, or high risk of bias within each domain. Traffic light plots and summary figures illustrating these assessments were generated using the Robvis visualisation tool [22].
Statistical analysis
All statistical analyses were conducted using RevMan version 5.4 (Cochrane Collaboration, Nordic Cochrane Centre, Copenhagen, Denmark). For each clinical outcome, odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated and pooled across studies. Inter-study variability was addressed using the DerSimonian–Laird random-effects model [23]. Forest plots were generated to illustrate effect estimates. Between-study heterogeneity was quantified using the I2 statistic, with values of 25–50%, 50–75%, and > 75% interpreted as low, moderate, and high heterogeneity, respectively, consistent with prior meta-analyses [24, 25]. A p-value of < 0.05 was considered statistically significant throughout the analysis.
Results
Study selection
The initial search yielded 10,535 records across all databases. After removing 5109 duplicate entries, 5426 unique citations were screened by title and abstract. A total of 5388 records were excluded at this stage, leaving 38 articles for full-text assessment. Following detailed review, 5 studies satisfied all eligibility criteria and were included in the final analysis [18, 19, 26–28]. The study selection process is illustrated in the PRISMA flow diagram (Supplementary Figure S1).
Study and patient characteristics
All included studies were RCTs published between 2018 and 2025. Across the five included trials, a total of 23,524 participants were enrolled, with 11,744 assigned to β-blocker therapy and 11,780 to the control group. The pooled mean age of the study population was 62.8 ±11.6 years, and approximately 80% of participants were male. The average follow-up duration across the trials was 3.33 years. A comprehensive overview of baseline demographic and clinical characteristics for each trial is provided in Table I.
Table I
Study details and patient baseline characteristics of included RCTs
| Author/study | Year of publication | Follow-up duration [years] | Sample size, n | Age (mean ± SD) | Males, n (%) | BMI [kg/m2] | LVEF (%) | Previous PCI, n (%) | Diabetes, n (%) | Hypertension, n (%) | Current smoker, n (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | |||
| CAPITAL-RCT [26] | 2018 | 3.9 | 394 | 400 | 63.9 ±11.2 | 64.5 ±11.3 | 327 (83) | 312 (78) | 24.0 ±3.3 | 23.9 ±3.2 | 58.1 ±8.6 | 58.0 ±8.9 | 20 (5.1) | 21 (5.3) | 98 (25) | 81 (20) | 239 (61) | 234 (59) | 186 (47) | 188 (47) |
| ABYSS [27] | 2024 | 3.0 | 1852 | 1846 | 63.5 ±10.9 | 63.5 ±11.2 | 1531 (82.7) | 1530 (82.9) | 26.5 ±4.1 | 26.3 ±4.1 | 60 ±5.9 | 60 ±5.9 | 1693 (96.4) | 1709 (97.4) | 375 (20.2) | 372 (20.2) | 805 (43.5) | 786 (42.6) | 342 (18.5) | 385 (20.9) |
| REDUCE-AMI [19] | 2024 | 3.5 | 2508 | 2512 | 65 ±11.9 | 65 ±11.9 | 1945 (77.6) | 1944 (77.4) | NR | NR | NR | NR | 147 (5.9) | 175 (7.0) | 346 (13.8) | 354 (14.1) | 1155 (46.1) | 1163 (46.4) | 478 (19.4) | 530 (21.3) |
| BETAMI + DANBLOCK [28] | 2025 | 3.5 | 2783 | 2791 | 63 ±11.9 | 62 ±11.9 | 2182 (78.4) | 2230 (79.9) | 28 ±3.7 | 28 ±4.4 | NR | NR | 2582 (92.9) | 2577 (92.5) | 332 (11.9) | 363 (13.0) | 1127 (40.5) | 1149 (41.2) | 640 (28.1) | 614 (27.2) |
| REBOOT [20] | 2025 | 2.75 | 4207 | 4231 | 61.4 ±11.2 | 61.3 ±11.1 | 3391 (80.6) | 3420 (80.8) | NR | NR | 57.0 ±7.1 | 57.2 ±7.1 | 3906 (93.5) | 3925 (93.7) | 901 (21.5) | 893 (21.3) | 2182 (52.0) | 2185 (51.9) | 1851 (45.2) | 1824 (44.3) |
Results of quality assessment
Assessment of methodological quality using the RoB 2.0 tool demonstrated that four of the included RCTs were judged to have a low risk of bias across all domains whereas one trial was evaluated as having some concerns. Detailed risk of bias judgements are presented in Supplementary Figures S2 and S3.
Outcomes
All-cause mortality
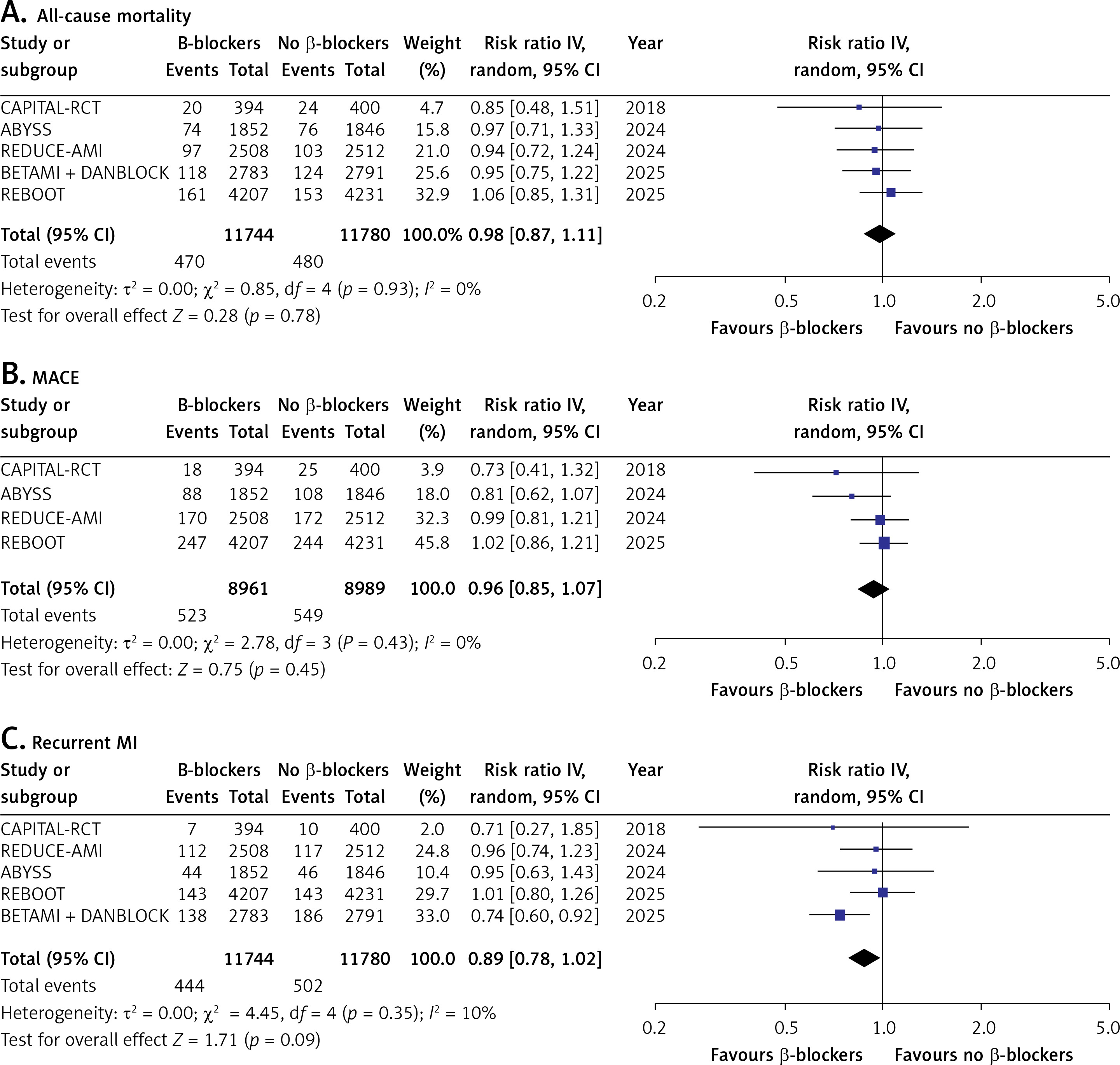
All five trials reported all-cause mortality. In the pooled analysis, β-blocker therapy showed no significant difference in all-cause mortality compared with no β-blocker use (RR = 0.98; 95% CI: 0.87–1.11; I2 = 0%; p = 0.78; Figure 1 A).
Major adverse cardiovascular events (MACE)
Four trials reported MACE. The pooled analysis showed no significant difference in the incidence of MACE between the two groups (RR = 0.96; 95% CI: 0.85–1.07; I2 = 0%; p = 0.45; Figure 1 B).
Recurrent myocardial infarction (MI)
All five trials reported recurrent MI. The pooled analysis did not reach statistical significance, with no significant difference observed between the β-blocker and control groups (RR = 0.89; 95% CI: 0.78–1.02; I2 = 10%; p = 0.09; Figure 1 C).
Cardiovascular mortality
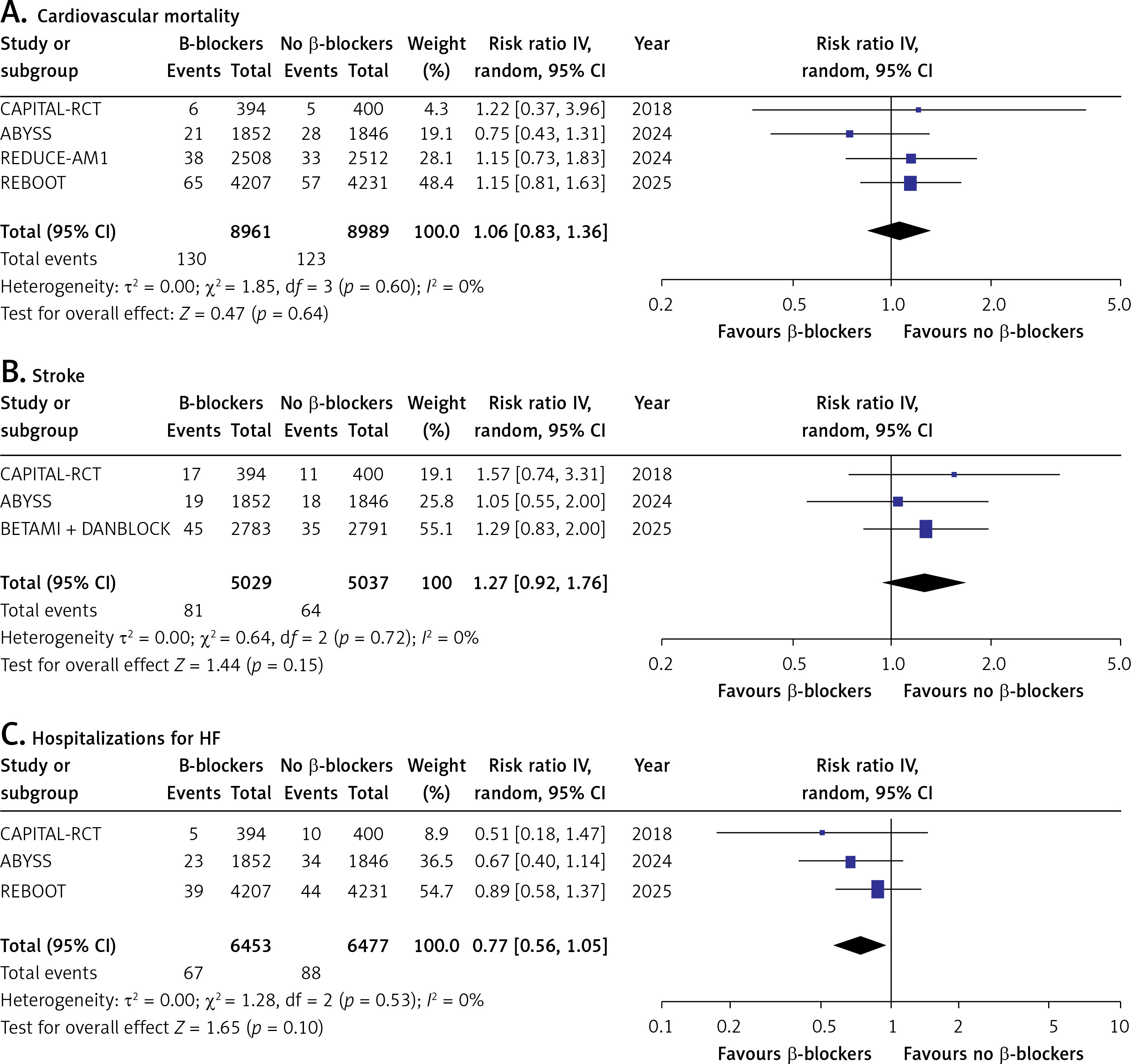
Four trials reported cardiovascular mortality. The pooled analysis demonstrated no significant difference between patients receiving β-blockers and those without β-blocker therapy (RR = 1.06; 95% CI: 0.83–1.36; I2 = 0%; p = 0.64; Figure 2 A).
Stroke
Three trials reported stroke as an outcome. The pooled estimate showed no significant difference in stroke risk between patients receiving β-blockers and those in the control group (RR = 1.27; 95% CI: 0.92–1.76; I2 = 0%; p = 0.15; Figure 2 B).
Hospitalisations for HF
Three trials provided data on hospitalisations for HF. The pooled analysis demonstrated no statistically significant reduction in HF-related admissions with β-blocker therapy compared with control (RR = 0.77; 95% CI: 0.56–1.05; I2 = 0%; p = 0.10; Figure 2 C).
Discussion
This meta-analysis evaluated the effects of long-term β-blocker therapy in patients recovering from AMI with preserved or mildly reduced ejection fraction. Across five randomised trials, encompassing 23,524 total patients, β-blockers did not confer a reduction in all-cause or cardiovascular mortality compared to no β-blocker therapy. Similarly, no significant differences were observed in MACE, recurrent MI, stroke, or hospitalisations due to HF.
These findings contrast with results from historical trials, which demonstrated substantial mortality benefits with long-term β-blocker therapy following MI [11, 29, 30]. However, earlier studies predated modern treatments like early reperfusion, PCI, statins, and potent antiplatelet agents [15, 31]. Patients in those trials often sustained larger infarcts and more frequently had reduced ejection fractions, conditions under which the anti-ischaemic and antiarrhythmic effects of β-blockers likely conferred greater benefit [32, 33]. In the modern reperfusion era, in which early revascularisation and comprehensive medical therapy substantially reduce baseline risk, the incremental benefit of chronic β-blockade in lower-risk patients has become increasingly uncertain [34, 35]. Recent large, randomised trials and meta-analyses report no reduction in mortality or major cardiovascular events among post-MI patients with preserved LVEF and no HF, supporting the evolving view that routine long-term β-blocker therapy may no longer be universally necessary in this population [18, 36, 37].
This shifting evidence is reflected in updated clinical guidelines. European guidelines now advocate for individualised duration of therapy rather than routine long-term continuation. In contrast, U.S. guidelines still recommend β-blockers for most MI patients without contraindications, classified as Class I for STEMI and Class IIa for NSTEMI with preserved ejection fraction, but they acknowledge that the optimal duration of therapy remains unclear and that evidence beyond 3 years is limited [12, 13].
Our pooled analysis demonstrated no mortality benefit from long-term β-blockers in post-MI patients with preserved EF. These findings are corroborated by large registry/cohort meta-analyses; a 2025 meta-analysis of 85,600 MI survivors with preserved EF found no significant decrease in all-cause or cardiovascular mortality with β-blocker use upon sensitivity analysis [36]. Notably, recent evidence indicates that the mortality benefit of β-blockers is influenced by three factors: an event-free period, study inclusion period, and baseline EF [38]. Specifically, patients who remain free of death, recurrent MI, or HF during the first post-MI year appear to derive minimal additional benefit from continued β-blocker therapy, particularly in cohorts included after 2010 with preserved EF. In contrast, the meta-analysis by Alnemer et al. identified significant reductions in both outcomes [39]. This discrepancy probably reflects differences in study composition and methodological differences; their analysis incorporated a disproportionately large number of observational cohort studies (thirteen in total) relative to only three RCTs, limiting their ability to address confounding and between-study heterogeneity. Notably, in their subgroup analysis, the apparent mortality reduction was driven by the cohort data, whereas effect estimates in the RCT subgroup were comparable to those observed in our analysis. Another individual–patient-level meta-analysis of 17,801 patients similarly reported nearly identical death rates in the β-blocker and control groups [40].
We similarly observed no statistically significant impact of β-blockers on MACE, defined as the composite of cardiovascular death, recurrent MI, or HF hospitalisation. These results are consistent with the individual patient-level meta-analysis by Kristensen et al., which reported nearly identical event rates between β-blocker and control groups [40]. In contrast, a pooled individual patient data analysis of four trials in patients with mildly reduced ejection fraction demonstrated a 25% relative risk reduction in a composite of death, MI, or HF [41]. This discrepancy may be explained by differences in population risk profiles; the latter analysis focused exclusively on patients with LVEF 40–49%, whereas our meta-analysis included all patients with LVEF ≥ 40%, encompassing both mildly reduced and preserved EF populations. As a result, any potential benefit confined to the lower EF subgroup may have been attenuated when pooled with patients who had preserved systolic function.
In our pooled data, long-term β-blockers did not significantly reduce the incidence of recurrent MI. This finding is consistent with the broader evidence base, because no large, contemporary trial in the era of routine reperfusion, dual-antiplatelet therapy, and high-intensity statins has shown a clear reinfarction prevention effect in patients with preserved EF. The marked decline in baseline reinfarction risk due to improved secondary prevention strategies may limit the potential for additional benefit from β-blockers [42, 43]. Some studies have suggested a short-term reduction in reinfarction risk particularly within the first year post MI, which is probably related to early anti-ischaemia and anti-arrhythmic effects; however, this benefit did not persist with longer follow-up [44]. Furthermore, the attenuated sympathetic activation and lower residual ischaemic burden in modern post-MI patients with preserved EF may further explain the absence of sustained benefit with chronic therapy. A previous meta-analysis of three RCTs by Sabina et al. similarly found no significant reduction in mortality or recurrent MI with long-term β-blocker therapy in this population [45].
We also observed no significant difference in post-MI stroke incidence between β-blocker and control groups. This lack of benefit is unsurprising given that β-blockers do not directly modify the main stroke risk factors in this context, such as atherosclerotic burden or atrial fibrillation, and any hypertensive benefit is modest [46, 47]. Moreover, stroke events following MI are relatively infrequent, rendering most studies underpowered to detect meaningful differences. Consistent with our findings, Gomes et al. reported a comparable incidence of stroke in their meta-analysis of randomised and observational studies [36]. Similarly, Sabina et al. found no significant difference in stroke outcomes among RCTs included in their pooled analysis [45].
Finally, we found no significant reduction in HF hospitalisations with long-term β-blocker therapy among post-MI patients with preserved EF. This finding aligns with multiple large meta-analyses and original studies conducted in the modern era [36, 44, 48]. Large European and Asian cohort studies similarly indicate that, beyond the first post-MI year, continuation of β-blockers does not lower the risk of HF hospitalisation in patients without clinical HF or left ventricular systolic dysfunction [48, 49]. This contrasts with well-established benefits of β-blockers in patients with reduced ejection fraction or overt HF, in whom therapy effectively reduces HF events and mortality [50]. In contemporary preserved EF populations, robust ventricular function and aggressive revascularisation resulted in a low incidence of new-onset HF, with most events probably driven by comorbid conditions such as hypertension or diabetes, which are not substantially modified by β-blockade [43]. Future large-scale randomised trials are needed to better define the optimal duration and patient selection for β-blocker therapy in the modern post-MI population.
It is important to note that our analysis has certain limitations. Firstly, as a study-level meta-analysis, the absence of individual patient data limited our ability to adjust for confounding factors such as infarct size, medication adherence, and post-discharge treatment variability. Secondly, all included randomised controlled trials employed an open-label design with blinded endpoint evaluation; although blinded outcome adjudication reduces detection bias, the absence of double blinding may still introduce performance bias. Third, variations in β-blocker types, doses, and treatment durations among the pooled studies could have influenced the overall effect estimates. Thirdly, HF hospitalisation and stroke events were relatively infrequent, potentially limiting statistical power for detecting small but clinically meaningful differences. Fourthly, most participants across the included trials were male (ranging from 77% to 83% across intervention and control groups), which may limit the generalisability of our findings to female post-MI patients. Finally, the limited number of available randomised controlled trials in preserved EF populations underscores the need for further high-quality, long-term studies to clarify the role and optimal duration of β-blocker therapy following MI.
In conclusion, in patients with acute MI and preserved or mildly reduced ejection fraction, long-term β-blocker therapy did not reduce all-cause mortality, cardiovascular mortality, or MACE. Additionally, no significant reductions were observed in recurrent MI, stroke, or hospitalisations for HF over an average follow-up of 3 years. These findings suggest that routine long-term β-blocker use in this population may offer limited clinical benefit. Future research should focus on identifying patient subgroups who may still derive benefit, and on evaluating potential safety outcomes associated with continued therapy.