Introduction
As the age of the population and the burden of chronic diseases continue to increase, the need for more proactive and cost-effective health strategies becomes mandatory. Primary Health Care (PHC) remains the first point of contact for most individuals in the health system, delivering comprehensive, continuous, and person-centered care while focusing on health promotion and disease prevention [1]. Preventive care of non-infectious diseases includes – among others – early detection, risk reduction, and longitudinal patient care. Non-communicable diseases (NCDs), such as cardiovascular and ophthalmological diseases, diabetes and cancer, represent a growing global health burden. Early identification of these conditions in PHC settings can significantly reduce morbidity, mortality, and healthcare costs.
Most PHC systems face constraints such as restricted clinical time, fragmented data, workforce shortages as well as variability in the quality of delivered care. Because of both recent advances in computational power and growing availability of health data, Artificial Intelligence (AI) has emerged as a powerful tool in PHC [1]. AI may enhance early disease detection, personalized risk assessment and optimized resource allocation leading to more effective and efficient preventive care in PHC [2, 3]. Computational techniques such as machine learning (ML), natural language processing (NLP), clinical decision support (CDS) tools, and predictive analytics can process huge amounts of health data, ranging from electronic health records (EHRs) to wearable sensor data. All these technologies can analyze large and complex datasets to identify patterns that may not be immediately apparent to clinicians, thus enabling earlier detection of disease, more accurate risk classification, and enhanced patient outcomes [2, 4]. While AI adoption in tertiary care has already gained significant importance, its application in PHC settings remains less systematically studied.
This scoping review aims to explore the role of AI in advancing preventive care of NCDs within PHC settings by reviewing its current implementation and effectiveness as well as assessing potential challenges and impact on patient outcomes.
Methods
Study design
The Population, Concept and Context (PCC) framework utilized for structuring the research question is presented in Table I.
Table I
PCC framework of the study
Search strategy
Two scientific databases, PubMed/Medline and Scopus, were systematically searched to identify studies on the AI-based systems or applications in prevention, early detection or health risk assessment of NCDs within PHC settings. Last search was performed on November 8, 2025. A combination of keywords and MeSH terms was used: “Artificial Intelligence” OR “Machine Learning” OR “Deep Learning” AND “Disease Prevention” OR “Preventive Health” AND “Primary Health Care” OR “Family Practice” OR “General Practice”. All English-language studies published within the last five years in the aforementioned databases were eligible for participation in the present review.
Inclusion criteria
Only studies involving primary healthcare adults (≥ 18 years, at risk of or affected by NCDs) and primary healthcare providers (general practitioners/family physicians) were included. More specifically, studies referring to AI-based technologies (ML, predictive analytics, NLP, AI-driven CDS) implemented in clinical practice in preventive medicine of NCDs in PHC were incorporated in the study. AI-supported preventive care was compared to standard preventive care or non-AI-based interventions in the included studies. Preventive medicine was defined as at least one outcome related to disease incidence, risk reduction and early detection rates of non-infectious diseases. Only primary research studies i.e. randomized controlled trials (RCTs), cohort studies, case-control studies and cross-sectional studies were analyzed.
Exclusion criteria
Studies conducted in secondary or tertiary settings or focusing on treatment rather than prevention or exploring the role of AI in infectious diseases were excluded from the review. Non-AI-based interventions such as manual risk calculators or traditional clinical guidelines without AI support were not incorporated in this review. Additionally, non-English studies, expert opinions, editorials, commentaries, conference abstracts, systematic or scoping or umbrella reviews, meta-analyses or purely technical computer science papers were excluded as well.
Information sources
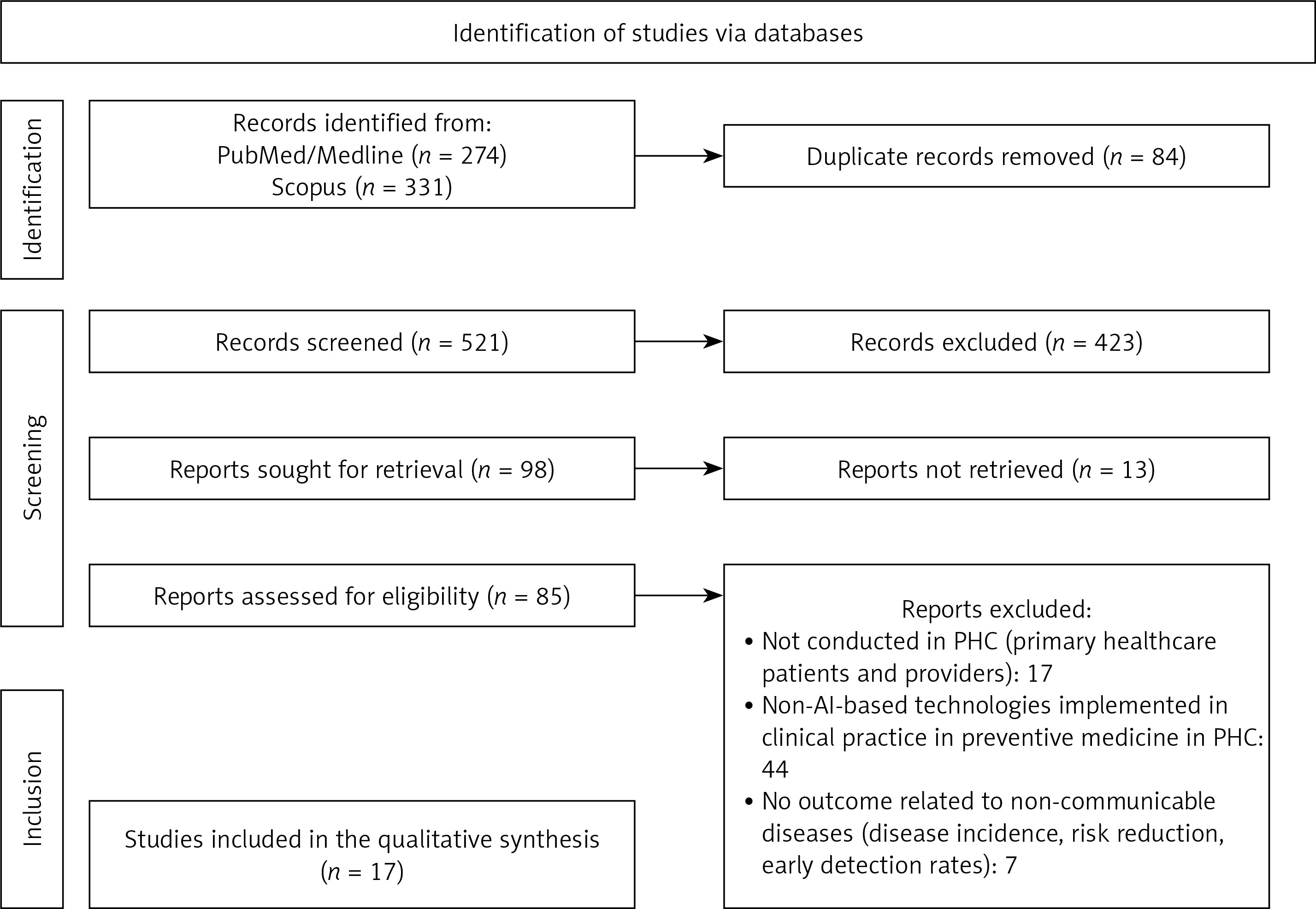
The screening and selection process is illustrated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) flowchart (Figure 1). The search revealed 605 potential sources. Firstly, 84 duplicates were removed. Two independent members of the team (P.K. and F.M.) evaluated the remaining 521 titles/abstracts for relevance and only 98 articles were sought for retrieval and further studying of the full-text article. Any disagreement between the two team members with regard the eligibility of a study was resolved by the third one (P.P.) who reviewed it. Finally, 17 articles were retained for this review.
Results
Seventeen studies met eligibility criteria, encompassing populations across the United States, Australia, the United Kingdom, Netherlands, China, India, and Indonesia. AI interventions targeted specific medical conditions like diabetes mellitus (DM) and hypertension (HTN), ophthalmological diseases like diabetic retinopathy (DR) and age-related macular degeneration (AMD), cardiovascular diseases such as atrial fibrillation (AF) and cardiomyopathy, and cancer. In some of the included references, low-income population or low-resource settings were studied [5–7]. Most studies utilized ML algorithms, automated image analysis systems, NLP or CDS tools integrated into primary care workflows. Comparison of AI-based technologies was performed against usual, traditional or standard risk assessment. Table II summarizes the included studies, their location, the medical condition under study as well as the AI interventions utilized.
Table II
Literature studies included in the present research, location, medical condition under study and AI intervention implemented
| Study | Country | Year | Medical condition | Implemented Artificial Intelligence technology |
|---|---|---|---|---|
| Chima et al. [8] | Australia | 2025 | Cancer prevention | Clinical decision support |
| Liu et al. [17] | USA | 2023 | Lung cancer | Natural language processing |
| Emery et al. [10] | Australia | 2023 | Colorectal cancer | Clinical decision support |
| Briggs et al. [16] | UK | 2022 | Oesophago-gastric cancer | Machine learning risk prediction |
| Elliott et al. [9] | USA | 2022 | Cancer | Clinical decision support ± shared decision making |
| Malhotra et al. [14] | UK | 2021 | Pancreatic cancer | Machine learning risk prediction |
| Shah et al. [19] | USA | 2021 | Prostate cancer | Risk-stratified clinical decision support |
| Schut et al. [18] | Netherlands | 2025 | Lung cancer | Natural language processing |
| Bhuiyan et al. [21] | USA | 2021 | Age-related macular degeneration and diabetic retinopathy | Automated retinal image analysis |
| Chen et al. [15] | USA | 2025 | Diabetic retinopathy | Artificial Intelligence-based retinal image analysis |
| Liu et al. [13] | USA | 2021 | Diabetic retinopathy | Automated retinal image analysis |
| Gu et al. [11] | China | 2024 | Multiple fundus disease | Artificial Intelligence-based fundus image analysis |
| Fuller et al. [7] | USA | 2022 | Diabetic retinopathy | Automated retinal image analysis |
| Hill et al. [12] | UK | 2022 | Atrial fibrillation | Machine learning risk prediction |
| Estiko et al. [6] | Indonesia | 2025 | Hypertension | Machine learning risk prediction |
| Boutilier et al. [5] | India | 2021 | Diabetic mellitus and hypertension | Machine learning risk stratification |
| Kinaszczuk et al. [20] | USA | 2025 | Cardiomyopathy | Artificial Intelligence-based screening tools |
In general, outcomes included screening uptake, referral adherence and feasibility of implementation. Improvement in risk-appropriate screening and clinical follow-up was revealed in the included RCTs during the comparison of the AI-supported preventive care with the standard one [8–10]. Observational and validation studies consistently reported that AI models outperformed conventional approaches in identifying high-risk individuals for conditions such as DR, AF, DM and multiple cancers [11–14]. Economic evaluations indicated that AI-based screening strategies were cost-effective, particularly in underserved populations [7, 12]. Although improvement in workflow efficiency was detected, barriers related to usability, integration and clinician trust were identified [15].
Discussion
Existing evidence for AI integration in PHC in the sector of preventive care of NCDs is highlighted in the present review. The included studies demonstrate that AI can play a transformative role in preventive care within PHC settings as AI interventions consistently demonstrated improvement in the early detection rate and risk stratification across a range of conditions. Importantly, these technologies can address key challenges in PHC such as limited time per patient and the need for proactive management of chronic diseases. However, implementation challenges and ethical considerations remain a critical barrier to large-scale adoption.
Early cancer detection saves lives by identifying the disease before it spreads when treatment is most effective and less invasive. Thus, survival rates improve, treatment costs are decreased, and patients have a better quality of life. Almost half of the included studies referred to cancer preventive care [8–10, 14, 16–19]. More specifically, lung, esophago-gastric, colorectal, pancreatic and prostate cancer early detection with the implementation of AI-tools have been analyzed. Two retrospective studies based on EHRs and GP clinical notes revealed that CDS systems as well as NLP-based AI improve completeness of lung cancer screening and enables earlier lung cancer detection [17, 18]. Additionally, in the RCT of Emery et al., the use of CRISP risk prediction CDS system enabled better targeting of colorectal cancer [10]. In the retrospective studies of Briggs et al. and Malhotra et al., the integrated ML-models allowed improved risk prediction for esophago-gastric and pancreatic cancer, respectively [14, 16]. The use of risk-stratified CDS system in the primary care network in the USA improved prostate screening practice as well [19]. Finally, in the RCTs of Chima et al. and Elliott et al., the integrated CDS tools enhanced cancer risk detection in general and the cost-effectiveness increased when the CDS system was paired with shared decision making [8, 9]. Implementing AI-based tools in cancer preventive care in the PHC settings seems promising in early diagnosis and subsequent restriction of cancer morbidity and mortality.
Cardiovascular diseases show high morbidity and mortality worldwide, placing a heavy burden on individuals, families and healthcare systems. Early detection allows for on-time intervention and lifestyle changes that can significantly lower the risk of heart attacks and strokes. In the PHC sector, AI has been implemented in the early detection of AF, hypertension and cardiomyopathy [5, 6, 12, 20]. In the retrospective studies of Boutilier et al. and Estiko et al., ML models showed improved predictive performance and supported hypertension screening without laboratory tests [5, 6]. In addition, AI-based AF screening allowed early detection and turned to be economically viable [12]. The early detection of AF is of importance as proper treatment can minimize stroke risk. Finally, in the observational study of Kinaszczuk et al. in 2025, AI implementation enabled the identification of individuals at elevated risk for cardiomyopathy, thus supporting early preconception cardiac risk screening [20].
The integration of AI-technology in early detection of ophthalmic diseases has been studied mostly in the case of DR [7, 13, 15, 21]. AMD and fundus disease has also been targeted [11, 21]. Unfortunately, DR remains a major cause of vision impairment and blindness among people with DM. Except for affecting the quality of life and daily functioning of the patients, its growing prevalence places a significant burden on caregivers and healthcare systems worldwide. Automated image analysis successfully detected referrable eye disease in PHC patients, turned out to be cost-effective and improved access and care continuity [7, 13, 21]. High diagnostic accuracy across multiple fundus diseases with AI-assisted screening system has been described in the multicenter, cross-sectional study of Gu et al. [11]. Early ophthalmological referral as well as follow-up adherence can minimize the burden of DR and other eye diseases and subsequently reduce blindness risk.
Although current evidence is encouraging, successful implementation of AI in clinical practice requires attentive integration, data quality, clinician acceptance and validation in diverse PHC populations. Additionally, ethical considerations such as transparency, explainability, and patient consent must be addressed to maintain trust in AI systems. Continued research is critical for maximizing AI’s contribution to population health and preventive service delivery.
In conclusion, AI has strong potential to redefine preventive care of non-infectious diseases in PHC. Cost-effectiveness evidence across the reviewed literature was generally favorable, particularly for AI-enabled screening programs targeting high-prevalence or high-burden conditions. Future research could focus on large-scale, multi-center implementation studies, integration of AI tools into electronic health record systems, clinician training and engagement to enhance trust in AI outputs as well as economic evaluations to guide policymakers and healthcare organizations.