Introduction
Heart failure is a clinical syndrome characterized by the inability of the heart to pump sufficient blood to meet the body’s metabolic demands [1]. It is a serious public health problem with a high death rate and a substantial financial burden affecting millions globally. Approximately 6.5 million people in the United States have heart failure (1–2% of the general population), with about 550,000 new cases diagnosed yearly. Heart failure incidence and prevalence rates are increasing globally, with rates as high as 10% in people over 70 years old. This trend is mainly attributable to an aging population and increased risk factors such as hypertension, diabetes, and obesity [2–4].
Systemic and pulmonary congestion is a significant prognostic indicator of heart failure outcomes. Loop diuretics, including furosemide, torsemide, and bumetanide, are the most effective treatment for heart failure to optimize volume status. Furosemide is the most commonly used loop diuretic in heart failure [5]. However, it has pharmacokinetic limitations, with slower absorption than its elimination half-life, a phenomenon called flip-flop kinetics, and a bioavailability of 50% [6, 7]. On the other hand, torsemide has rapid absorption, reaching peak concentrations within 0.5 to 2 h after an oral dose and a bioavailability of 80-100%.
Furthermore, torsemide has an anti-aldosterone effect by inhibiting aldosterone production, receptor binding, and blocking the renin-angiotensin-aldosterone system (RAAS) [8, 9]. Such neuro-hormonal modulatory effects can potentially enhance myocardial fibrosis and ventricular remodeling [10]. There are conflicting data regarding the efficacy of torsemide vs. furosemide in heart failure patients. Hence, we performed a comprehensive systematic review and meta-analysis to compare outcomes between furosemide and torsemide use.
Methods
This meta-analysis was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the Cochrane Collaboration Handbook [11].
Search strategy and study selection
Two independent reviewers (MME, MRM) conducted a literature search of electronic databases, including Medline/PubMed, Embase, and the Cochrane Central Register of Controlled Trials, without language limitations, from database inception to January 2023. We also searched Google Scholar and two clinical trial registries (the World Health Organization’s International Clinical Trials Registry Platform and ClinicalTrials.gov). The references of the retrieved studies were screened for additional studies appropriate for this meta-analysis. The search included the following query terms: (“Furosemide”) AND (“Torsemide”) AND (“heart failure”). There were no restrictions on sample size or follow-up duration. Studies were considered eligible for inclusion in the meta-analysis if they met pre-determined inclusion criteria: (1) studies evaluating furosemide versus torsemide; (2) studies enrolling patients with congestive heart failure; and (3) studies evaluating cardiovascular outcomes. RCTs were included. Observational studies, editorials, reviews, and non-human studies were excluded.
Screening, data extraction, and quality assessment
Two reviewers (SM, AS) conducted initial title and abstract screening, and discrepancies were resolved by a third reviewer (MN). Potentially eligible studies underwent full-text review and assessment for inclusion. Study and patient characteristics and outcomes data were extracted into a spreadsheet. Study and patient characteristics data included the first author’s name, study design, study country, sample size, median age, percentage of male subjects, hypertension, diabetes, dyslipidemia, and CKD. Two authors (MN and SM) independently assessed the quality of studies and the risk of bias.
Outcomes
Outcomes of interest included all-cause mortality, hospitalization due to heart failure, and weight change. Hospitalization due to heart failure is defined as any hospitalization within 12 months due to worsening heart failure symptoms.
Statistical analysis
Continuous data (e.g., weight change) were pooled as a standard mean difference (SMD comparing the furosemide and torsemide groups. The random-effect model was adopted in all analyses. We used the inverse variance method with DerSimonian and Laird approach to calculate tau-squared (τ2) for random-effects analysis. Odds ratios (for mortality and heart failure hospitalization) were pooled using the inverse variance method with the Paule–Mandel estimator of τ2. We assessed between-study heterogeneity using Q and I2 statistics. An I2 statistic of < 25% indicates low heterogeneity, and > 50% reveals high heterogeneity. Analyses were conducted using STATA 16 (State Corp LLC). P-values < 0.05 were considered statistically significant.
Results
Summary of studies
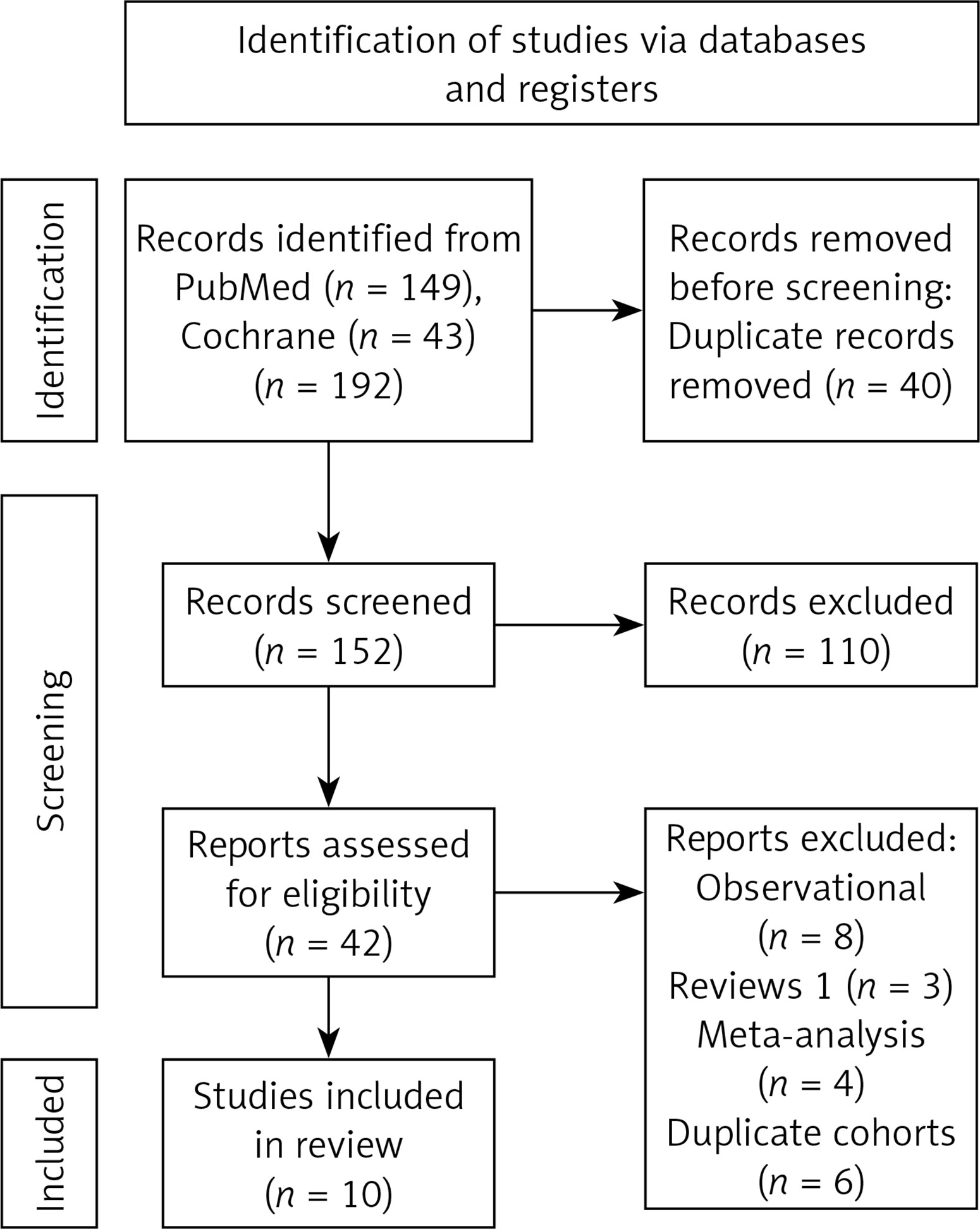
The initial search identified a total of 192 studies. After title and abstract screening, 42 studies underwent full-text review based on our inclusion criteria. Ten studies, all RCTs, met the inclusion criteria and were included in the meta-analysis [12–21]. The search process is outlined in Figure 1. A total of 4011 patients were included in our final pooled analysis, of whom 2019 were treated with furosemide and 1992 patients were treated with torsemide. The baseline characteristics of the patients in each study are presented in Tables I A and I B. Across the included studies, the mean ages ranged from 60 to 80 years. Men represented 55% in the furosemide group and 61% in the torsemide group. The length of follow-up ranged from 6 to 18 months. Study characteristics and diuretics doses are reported in Table II.
Table I
A – Baseline characteristics of patients in the included studies. B – Baseline characteristics of included studies
| A | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Age (mean) [years] | Men % | HTN % | Body weight [kg] | CAD % | |||||
| Furosemide | Torsemide | Furosemide | Torsemide | Furosemide | Torsemide | Furosemide | Torsemide | Furosemide | Torsemide | |
| Lopez 2004 [12] | 63 ±3 | 63 ±3 | 68 | 75 | 52 | 55 | 76 ±3 | 84 ±3 | 21 | 25 |
| Müller 2003 [13] | 73.2 ±10.2 | 74.4 ±14 | 41 | 45 | 31 | 27 | 76.2 ±18.7 | 77.9 ±17.1 | 51 | 41 |
| Han 2014 [14] | 59.4 ±10.2 | 58.2 ±9.5 | 52 | 63 | 9 | 13 | n/a | n/a | 9 | 11.6 |
| Noe 1999 [15] | 75.1 | 75.1 | 54 | 57 | 59 | 63 | 72 | 81 | n/a | n/a |
| Yamato 2003 [16] | 64.9 ± 6.2 | 64.7 ±6.1 | 60 | 56 | 24 | 28 | n/a | n/a | 48 | 52 |
| Murray 2001 [17] | 64.1 ±12.4 | 64.1 ±10.9 | 46 | 49 | 57 | 61 | 84.6 ±22 | 85.9 ±23 | 41 | 35 |
| Kasama 2006 [18] | 68 | 68 | 70 | 75 | 25 | 25 | 58 | 59 | n/a | n/a |
| The TORAFIC 2011 [19] | 69.3 | 68.1 | 61 | 54 | n/a | n/a | 80.4 | 82.3 | n/a | n/a |
| Mentz 2023 [20] | 65 | 64 | 61 | 65 | n/a | n/a | n/a | n/a | 26.6 | 29.8 |
| Trippel 2017 [21] | 69.3 ±8.1 | 68 ±8.3 | 39 | 76 | 94 | 100 | n/a | n/a | 39 | 53 |
Table II
Characteristics of included studies
| Study | Country | Sample Size | Design | Furosemide dose | Torsemide dose | Follow-up duration |
|---|---|---|---|---|---|---|
| Lopez 2004 [12] | Spain | 39 | Individually randomized, open-label, parallel-group pilot study | 20–40 mg/day | 10–20 mg/day | 8 months |
| Müller 2003 [13] | Switzerland | 237 | Prospective, randomized, unblinded study | Dose chosen by the physician on an individual basis | Dose chosen by the physician on an individual basis | 9 months |
| Han 2014 [14] | China | 185 | Prospective, randomized, unblinded study | 20 mg/day | 10 mg/day | 12.3 months |
| Noe 1999 [15] | USA | 240 | Prospective, randomized, unblinded study | Dose chosen by the physician on an individual basis | Dose chosen by the physician on an individual basis | 6 months |
| Yamato 2003 [16] | Japan | 50 | Prospective, randomized, open-label trial | 20–40 mg/day | 4–8 mg/day | 6 months |
| Murray 2001 [17] | USA | 234 | Prospective, randomized, open-label trial | 80–160 mg/day | 20–80 mg/day | 12 months |
| Kasama 2006 [18] | Japan | 40 | Prospective, randomized, unblinded study | 20–40 g/day | 4–8 mg/day | 6 months |
| The TORAFIC 2011 [19] | Spain | 155 | Prospective randomized open-label blinded end points | 40 mg/day | 10 mg/day | 8 months |
| Mentz 2023 [20] | USA | 2859 | Open-label, pragmatic randomized trial | Dose chosen by the physician on an individual basis | Dose chosen by the physician on an individual basis | 17.4 months |
| Trippel 2017 [21] | Germany | 35 | Randomized, double-blind, two-arm, parallel group, therapeutic confirmatory phase III trial | 20 mg/day | 5 mg/day | 9 months |
Outcomes
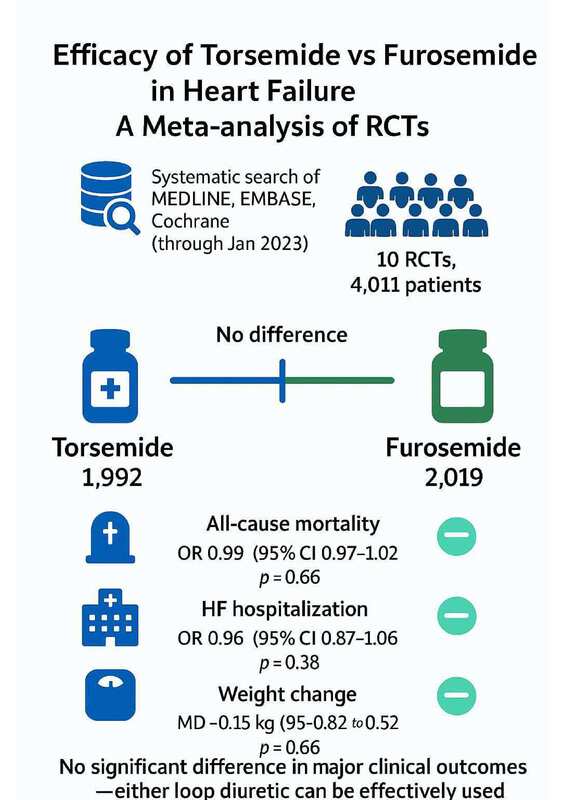
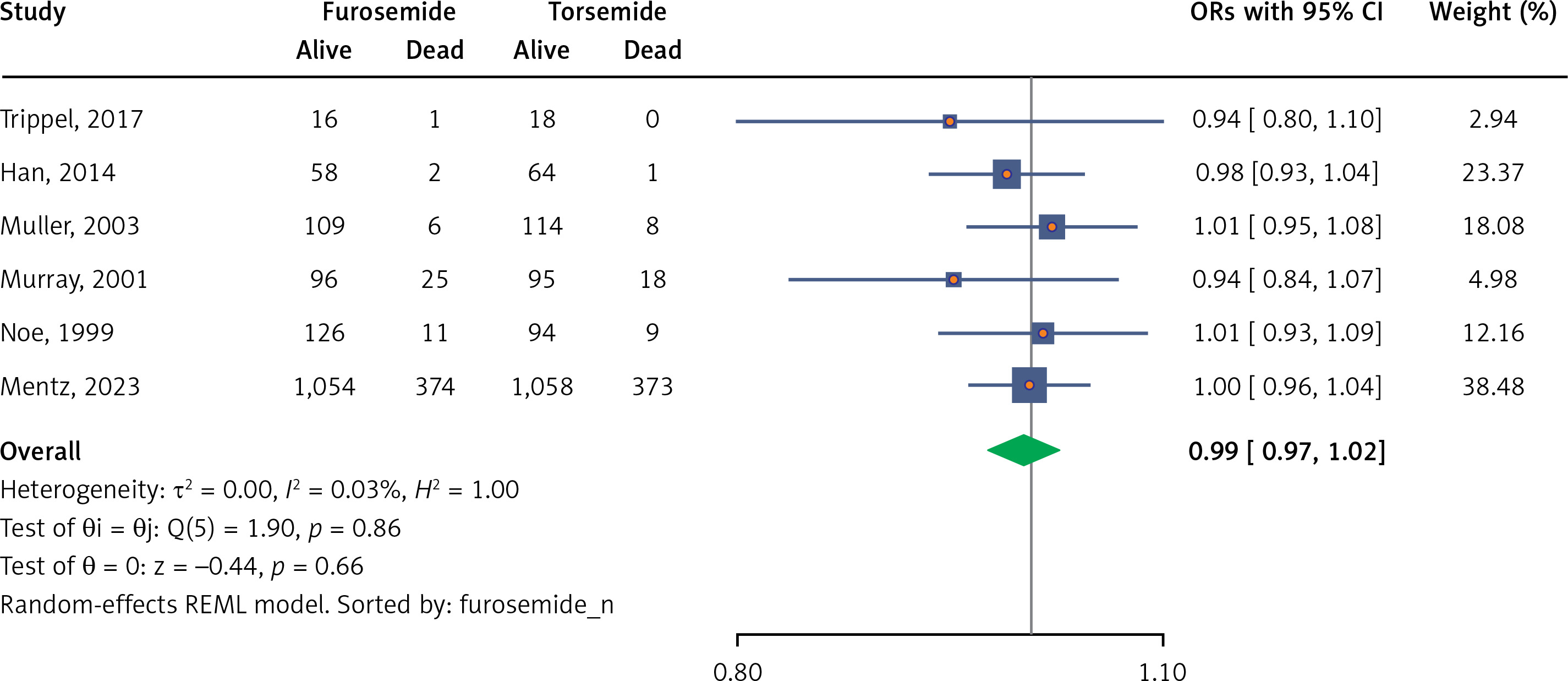
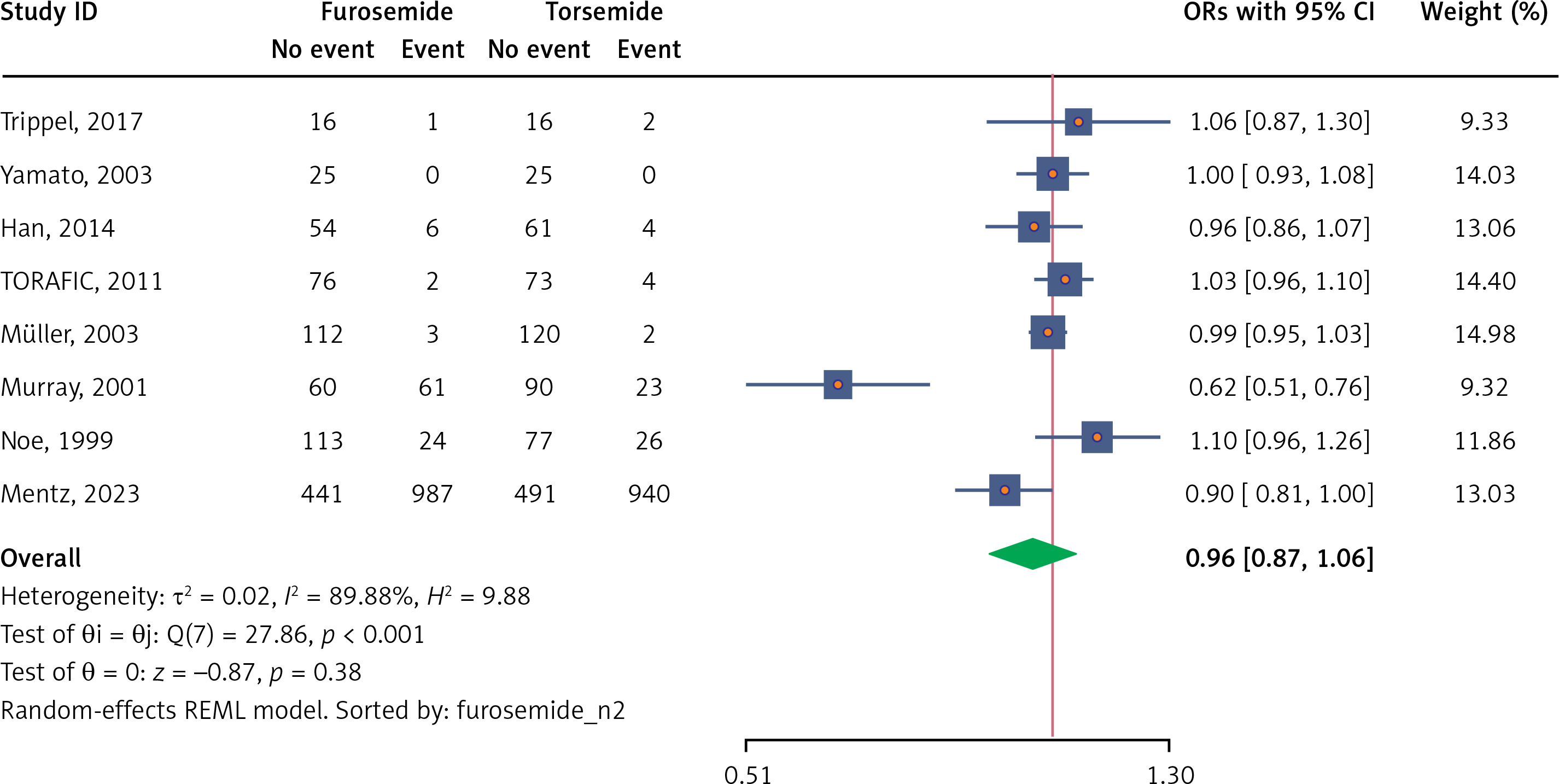
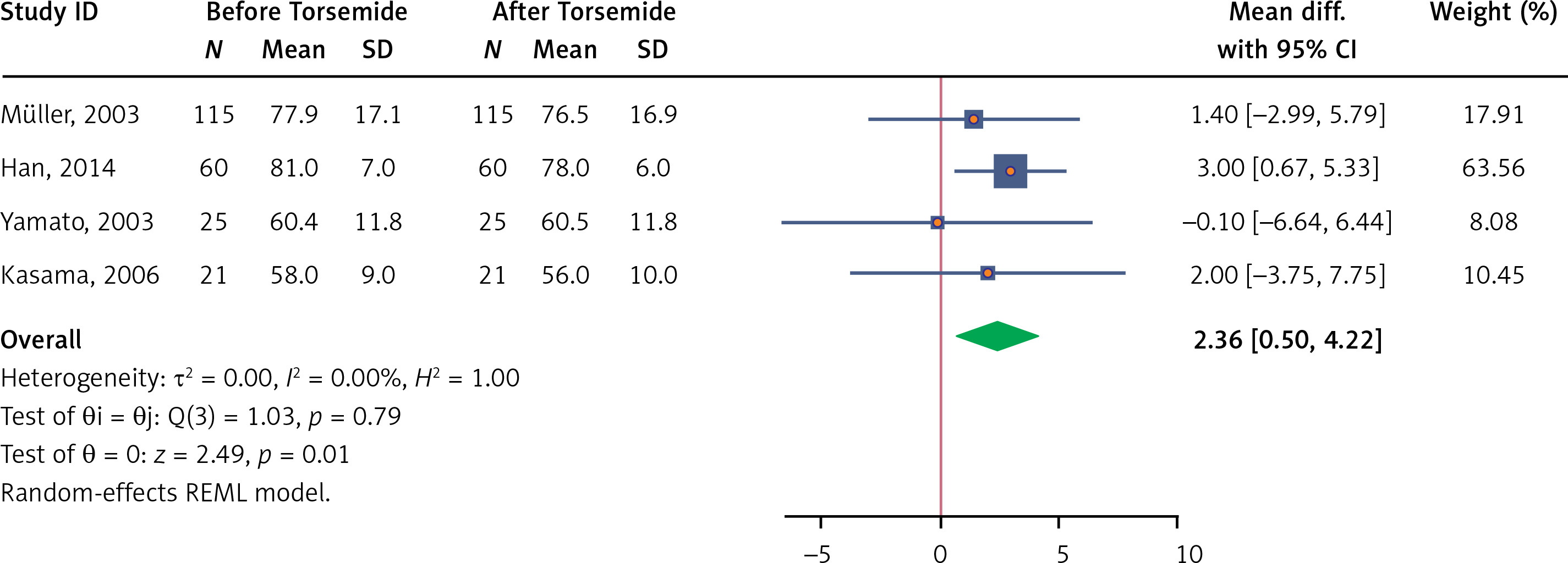
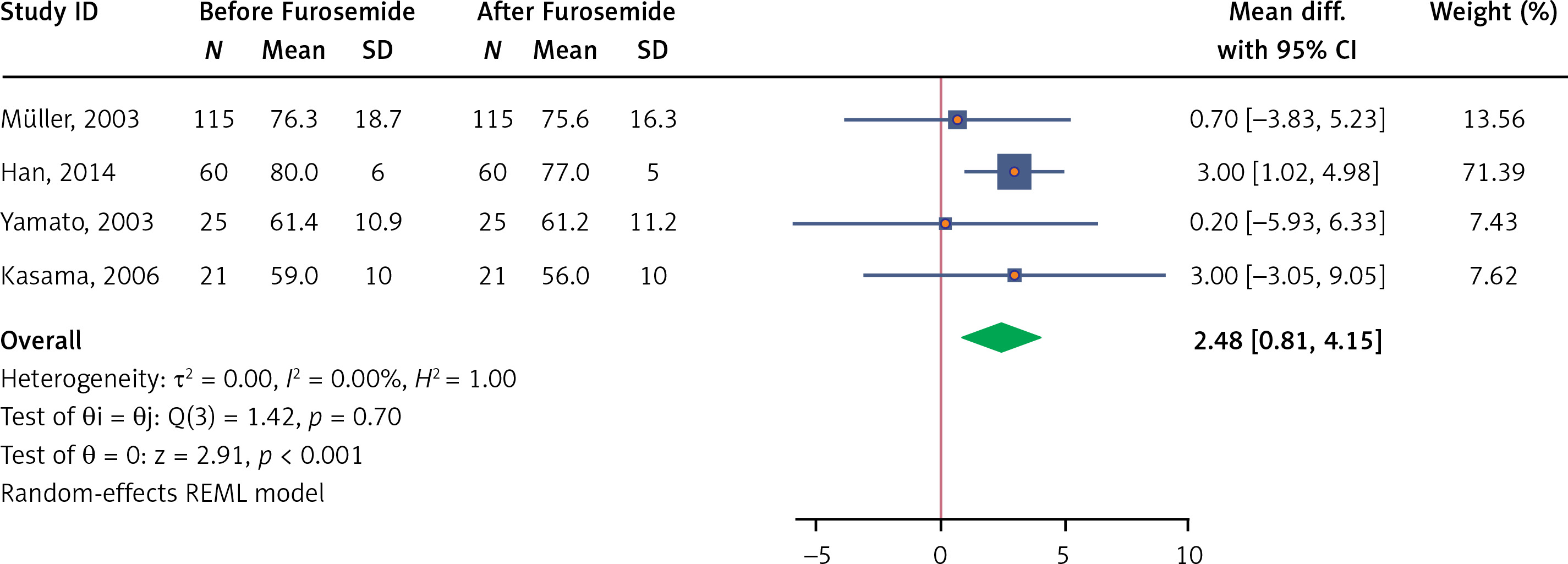
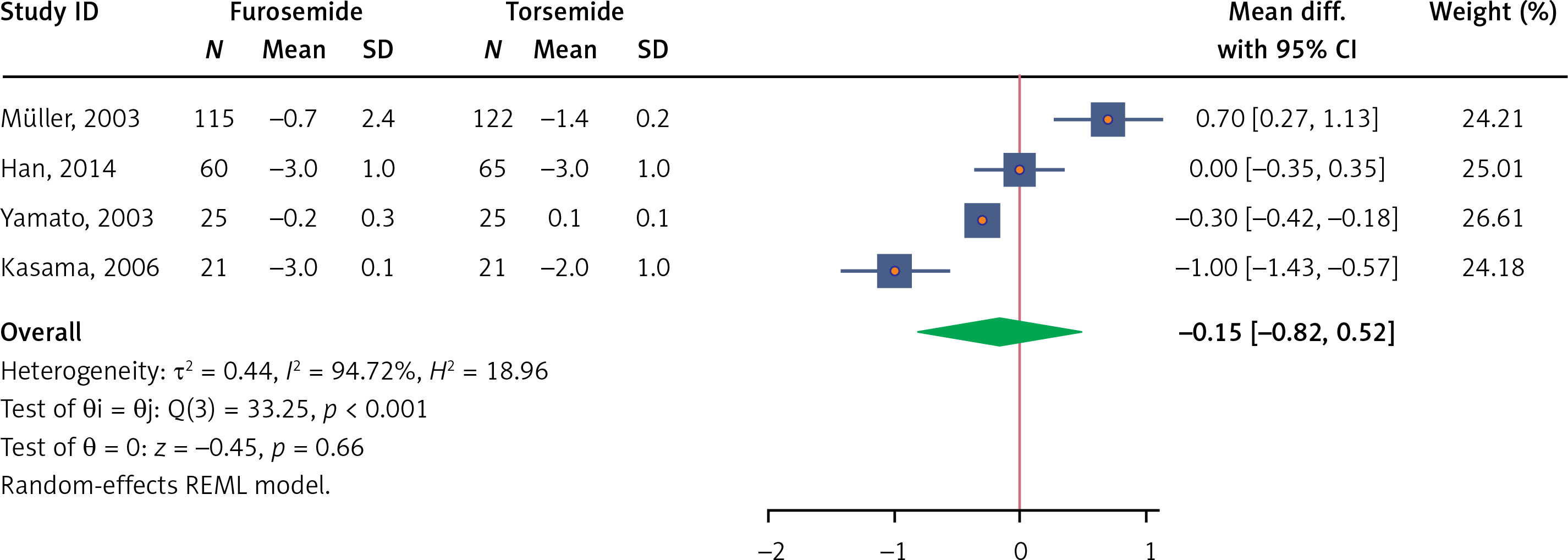
There was no significant difference between the groups in terms of all-cause mortality (OR = 0.99; 95% CI: 0.97–1.02; p = 0.66; I2 = 0.03%) (Figure 2) or heart failure hospitalization (OR = 0.96; 95% CI: 0.87–1.06; p = 0.38; I2 = 89%) (Figure 3). Torsemide was associated with a significant weight change (mean difference 2.36; 95% CI: 0.5–4.22; p = 0.01; I2 = 0.0%) (Figure 4); and similarly, furosemide showed a significant effect (mean difference 2.48; 95% CI: 0.81–4.15; p = 0.00; I2 = 0.0%) (Figure 5). There was no significant difference in weight change between the two diuretics (mean difference –0.15; 95% CI: –0.82–0.52; p = 0.66; I2 = 94%) (Figure 6).
Discussion
To our knowledge, this is the most contemporary pooled analysis comparing furosemide and torsemide in 4011 heart failure patients. In our analysis, ten randomized controlled trials (RCTs) were included. Furosemide and torsemide showed no apparent difference regarding all-cause mortality, recurring admissions for worsening heart failure, or weight changes.
Diuretics are regarded as the essential treatment for controlling pulmonary and peripheral congestion in heart failure and improving a patient’s quality of life. Although torsemide and furosemide differ in their pharmacokinetic and pharmacodynamic profiles – such as torsemide having higher oral bioavailability, a longer half-life, and more consistent absorption – neither has demonstrated a clear clinical advantage over the other. Both drugs act on the thick ascending limb of the loop of Henle and provide similar natriuretic effects when given at equivalent doses.
The effect of diuretics on heart failure outcomes was studied by Selvaraj et al., who included 8300 heart failure participants in the PARADIGM trial. The study showed that congestion is an independent prognostic value in those patients, and achieving a euvolemic state can independently improve functional status and quality of life and may reduce cardiovascular events, including mortality [22]. Furosemide and torsemide are the most commonly used diuretics in daily practice. Better results were anticipated from torsemide due to the higher bioavailability and longer half-life over furosemide. An observational study by Cosin et al. compared torsemide and furosemide in patients with congestive heart failure (NYHA I–II). Although the study was not designed to evaluate mortality outcomes, torsemide was associated with a significantly lower risk of death [23].
In contrast, other observational studies have reported a higher mortality rate with torsemide, because patients treated with torsemide had more severe disease [24]. The limitations of the observational studies and the discrepancy in results necessitate large RCTs to address these differences. The TRANSFORM-HF trial, the largest RCT comparing the efficacy of the two diuretics, provided the most substantial contribution to our meta-analysis. The study randomized 2859 patients with heart failure to either receive furosemide or torsemide. At 12 months of follow-up, both groups showed no difference in all-cause mortality and total hospitalization across the different types of heart failure.
Similarly, our meta-analysis found no discernible difference between torsemide and furosemide in terms of outcomes for heart failure. This contrasts with a prior meta-analysis by Abraham et al. that demonstrated mortality benefits in patients receiving torsemide [25]. However, the meta-analysis included multiple observational studies with high clinical heterogeneity. Notably, there was no difference in all-cause or cardiac mortality between torsemide and furosemide in the sensitivity analysis of only RCTs, which was explained by the RCTs’ smaller patient populations and, hence, weaker ability to determine mortality results.
Furthermore, our analysis found no difference between torsemide and furosemide regarding recurrent hospitalization due to heart failure. This finding is consistent with observational studies. A study by Rahhal et al. assessed the impact of switching furosemide to torsemide versus optimizing the furosemide dose in patients with heart failure [26]. The 1-month and 6-month heart failure hospitalization rates did not differ between the two approaches. In a study by Murray et al., torsemide was significantly associated with fewer hospitalizations due to heart failure [17]. However, there were some limitations. First, the study’s ability to evaluate recurrent hospitalization was limited by the study’s small sample size. Additionally, there was an allocation bias where patients receiving the torsemide intervention had considerably more prior admissions for heart failure than those receiving the furosemide intervention, which likely overstated the benefit of torsemide. Similarly, our study found no difference between furosemide and torsemide regarding the impact on weight change. The included studies on weight change have significant heterogeneity in their results, probably due to the various diuretic dosages used by the groups.
Although our meta-analysis focused on outcomes such as all-cause mortality, heart failure related hospitalizations, and weight changes, we recognize that cardiac-specific mortality remains an area of interest. A more recent study by Yasmin et al. (JACC 2024; 83) suggested that torsemide may offer a mortality advantage in terms of cardiac deaths. However, most of the studies included in out meta-analysis did not clearly differentiate between cardiac and non-cardiac mortality in terms of assessed outcomes. This has limited our ability to conduct a focused analysis on cardiac mortality. We recognize this as an important gap in the literature, and we suggest that future investigations are needed to examine this endpoint more closely.
Although our analysis included only RCTs with a high level of evidence, recent trials have been conducted with patients already on guideline-directed medical therapies – including β-blockers, SGLT-2 inhibitors, mineralocorticoid receptor antagonists (MRAs), and angiotensin receptor-neprilysin inhibitor (ARNIs) – which might have confounded clinical outcomes and potentially affected diuretic requirements in both groups. Moreover, high cross-over rates were also observed in multiple trials, particularly in the torsemide group. This could be related to agent cost differences, patient and clinician preference, and perceived side effects. Diuretic and convergence doses were left to the clinician’s discretion, which may have also influenced the results. Our analysis did not sub-stratify patients based on ejection fraction, which might have confounded the results. Another limitation is that cardiac specific mortality was not consistently reported across the studies, making it difficult to investigate differences between furosemide and torsemide with regards to cardiac mortality.
In conclusion, our analysis indicates no significant differences between furosemide and torsemide in terms of mortality, hospitalization due to heart failure, or weight change.