Introduction
Vasopressor therapy is foundational in the management of circulatory shock when fluids alone are insufficient, with norepinephrine recommended as the first-line agent in adults with septic shock [1].
Although uncommon, acral ischaemia and necrosis are among the most devastating complications associated with high-dose or prolonged vasoconstrictor use, sometimes culminating in amputation and prolonged disability. In a contemporary cohort, the incidence of vasopressor-associated limb necrosis was approximately 0.25%, with higher cumulative dose and longer duration of therapy associated with risk [2].
Case reports and small series show that digital necrosis can occur without large-artery occlusion, implicating extreme microcirculatory dysfunction and vasoconstriction. Examples include bilateral digital necrosis after high-dose norepinephrine in mixed shock and symmetrical peripheral gangrene necessitating amputations in the setting of sepsis and vasopressor support [3, 4].
Mechanistically, several pathways likely converge: intense α-adrenergic vasoconstriction reducing nutritive capillary flow, endothelial injury and glycocalyx disruption, and disseminated microthrombi that shunt or block distal perfusion; these changes are amplified by the microcirculatory derangements intrinsic to shock states [5, 6].
Against this backdrop, we present two cases of severe acral necrosis after prolonged high-dose vasoconstrictor therapy, highlighting early recognition, risk mitigation, and the medico-legal implications of limb loss in critically ill patients.
Case reports
Case 1
A 54-year-old male with a history of long-term tobacco and alcohol abuse and arterial hypertension was admitted to a regional hospital after being found unconscious. On arrival, he was in cardiopulmonary collapse and required repeated defibrillation, endotracheal intubation, and invasive mechanical ventilation. Transthoracic echocardiography revealed severely depressed left-ventricular systolic function with a left ventricular ejection fraction (LVEF) of approximately 15–20% and right-ventricular dilatation. Because pulmonary embolism was suspected, systemic thrombolysis was initiated but failed to improve his hemodynamic or respiratory status.
The patient developed refractory cardiogenic shock requiring very high doses of catecholamines, including norepinephrine and adrenaline, to maintain blood pressure. Progressive respiratory failure necessitated escalation of support with veno-arterial extracorporeal life support (ECLS), which was established percutaneously in the right femoral vessels by a mobile cardiac-surgical retrieval team from our hospital. Following initial stabilisation on ECLS, the patient was transferred to our tertiary cardiac centre.
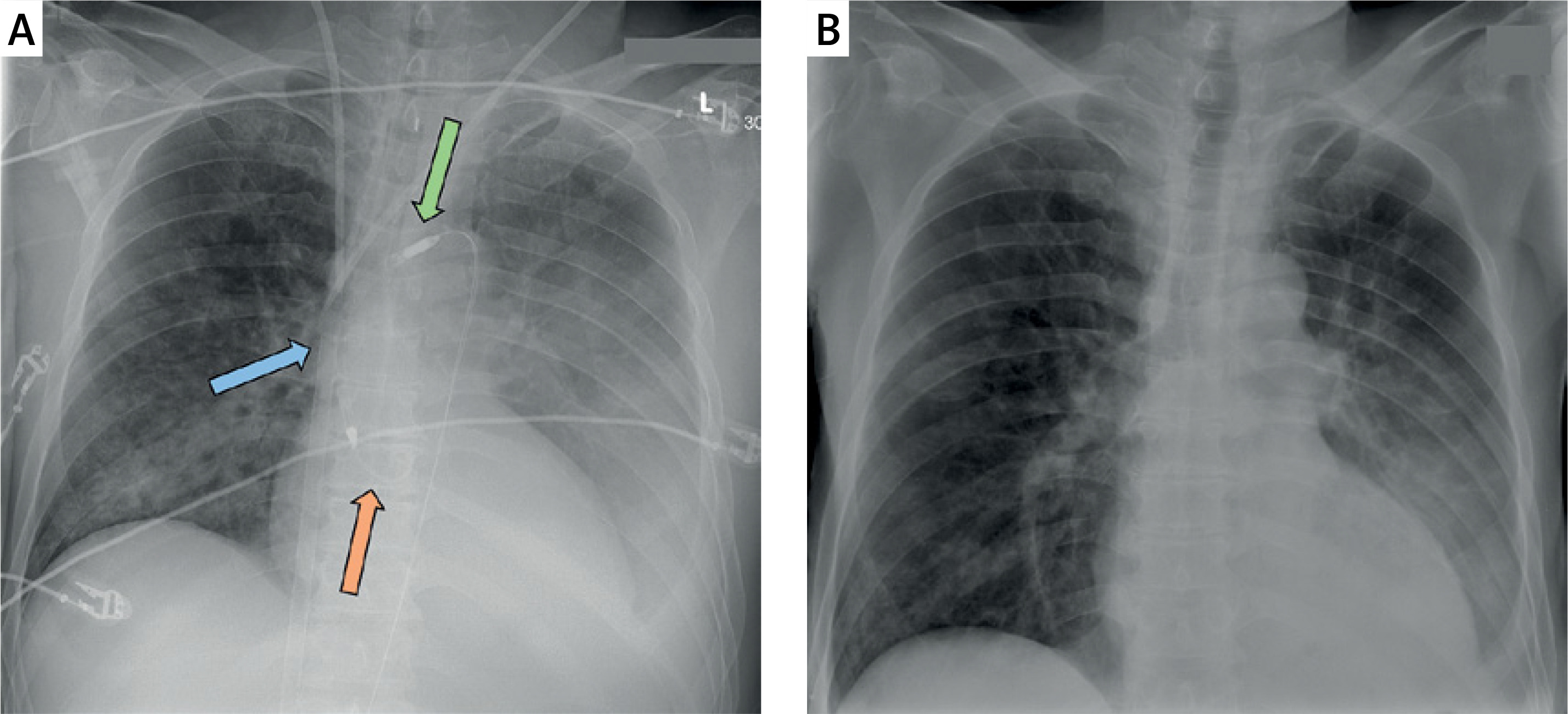
Coronary angiography demonstrated no obstructive coronary artery disease but confirmed a severely dilated and hypocontractile left ventricle, raising a strong suspicion of fulminant myocarditis. To achieve additional left-ventricular unloading, a transfemoral Impella CP® axial-flow pump was inserted via the left femoral artery (Figure 1). A good unloading effect was achieved initially. Computed tomography of the chest and abdomen excluded pulmonary embolism but showed bilateral pulmonary infiltrates consistent with acute respiratory distress syndrome (ARDS) and left-lower-lobe atelectasis. The patient’s coagulation profile was profoundly deranged in the context of suspected severe Gram-negative sepsis, leading to the decision to defer endomyocardial biopsy.
Figure 1
Chest radiographs of case 1. A – Post-implantation chest X-ray showing veno-atrial ECMO cannulation: the blue arrow indicates the tip of the venous cannula in the superior vena cava, the red arrow marks the ventricular end of the Impella® pump, and the green arrow denotes the aortic outflow end of the Impella® device. B – Chest X-ray obtained before discharge, demonstrating marked resolution of pulmonary oedema and pleural effusions following recovery
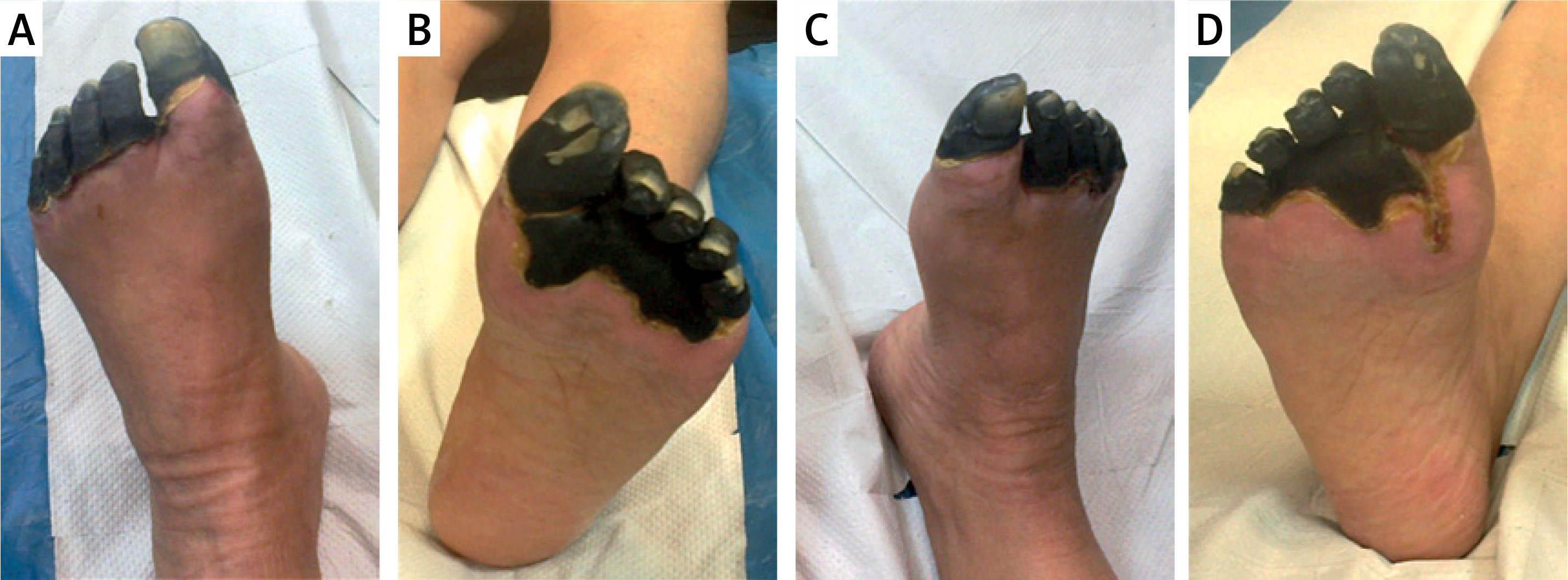
On the second hospital day, the Impella catheter was surgically removed because of device migration, and the left common femoral artery was reconstructed. Despite ongoing ECLS support, further vasopressor treatment was required for persistent distributive shock; however, in moderate and significantly reduced doses. During the subsequent days, the patient developed dry acral necroses of all four extremities, attributed to profound microcirculatory compromise during prolonged high-dose catecholamine therapy. The necroses remained demarcated and non-infected but ultimately required consideration of amputation and plastic soft-tissue coverage (Figures 2 and 3).
Figure 2
Lower limb involvement in case 1: ischaemic acral lesions of both feet. A – Dorsal view, left foot; B – plantar view, left foot; C – dorsal view, right foot; D – plantar view, right foot. The sharply demarcated black gangrene indicates advanced, irreversible necrosis

Figure 3
Upper limb involvement in case 1: digital ischaemia of both hands. A – Dorsal view, left hand; B – palmar view, left hand; C – dorsal view, right hand; D – palmar view, right hand. Note the dry gangrene affecting the fingertips despite preserved proximal perfusion

The patient’s pulmonary function gradually improved; a percutaneous dilatational tracheostomy was performed on day 11 to facilitate weaning from prolonged mechanical ventilation. Both the ECMO and tracheostomy cannula were successfully removed on day 11 once haemodynamic and respiratory stabilisation had been achieved. Subsequent transthoracic echocardiography revealed partial recovery of left-ventricular function (LVEF increased from 15% to approximately 30%).
At the time of discharge after a seven-week hospital stay, the patient was awake, mobilised on the ward, free of infection, and haemodynamically stable, with well-demarcated acral necroses awaiting planned staged amputation and reconstructive procedures.
Case 2
A 70-year-old woman with no documented history of diabetes mellitus was admitted to the intensive care unit (ICU) of a regional hospital for the management of severe community-acquired pneumonia complicated by respiratory failure. She required invasive mechanical ventilation and haemodynamic support due to persistent cardiovascular instability. To maintain adequate perfusion pressure during septic shock, she received high-dose vasoconstrictors, including norepinephrine and adrenaline (epinephrine), over a prolonged period.
During her ICU stay, the patient developed progressive discoloration of the toes on both feet, which evolved into sharply demarcated dry gangrene affecting all toes bilaterally. There was no clinical or laboratory evidence of superimposed infection (Figure 4). Vascular imaging was not performed at the time because her condition remained too unstable for transfer, but the lesions were attributed to microcirculatory compromise caused by prolonged high-dose vasopressor therapy.
Figure 4
Lower limb changes in case 2: bilateral acral gangrene of the toes following prolonged vasopressor therapy. A – Dorsal view, left foot; B – plantar view, left foot; C – dorsal view, right foot; D – plantar view, right foot. The lesions remained dry and well-demarcated, ultimately progressing to auto-amputation
Following gradual recovery of her pulmonary and haemodynamic status, she was weaned off vasopressors and mechanical ventilation and was eventually discharged from the ICU to the medical ward. Given the absence of infection and the dry nature of the gangrene, a conservative management strategy was adopted. The patient received local antiseptic dressings and restricted weight-bearing and mobilisation to avoid mechanical trauma. Over the following 6 months, the affected toes remained dry, mummified, and well demarcated without signs of cellulitis or systemic infection.
After this prolonged conservative phase, auto-amputation of the gangrenous toes occurred. The toes detached easily because the necrotic bones were brittle and fractured with minimal manual traction. A vascular surgeon gently removed the nonviable segments at the bedside. The wounds were left to heal by secondary intention under daily dressing changes.
Complete epithelialisation of the wounds was achieved within 2 months after auto-amputation. The patient remained free from local infection throughout the entire course of treatment. At her final follow-up, she had fully healed amputation sites with preserved mobility and no further vascular complications.
Discussion
In this report, we have described 2 cases of acral ischaemia and necrosis following prolonged high-dose vasoconstrictor therapy – an uncommon but devastating complication in critically ill patients. These cases highlight the importance of early recognition and a clear understanding of the multifactorial pathogenesis, the severe medical consequences, and the significant legal implications.
Pathophysiological mechanisms
The development of vasopressor-induced acral necrosis reflects the interplay of haemodynamic, microcirculatory, endothelial, and coagulative disturbances.
Excessive a-adrenergic vasoconstriction from high-dose norepinephrine/epinephrine reduces nutritive capillary flow and promotes distal ischaemia; this is seen in observational series and case reports of digital necrosis during extreme vasoactive support [2, 3, 5, 7].
Endothelial injury and glycocalyx disruption, typical of sepsis and shock, blunt autoregulation and render acral tissues especially vulnerable to vasoconstrictive stress [6, 8].
Microthrombi and coagulopathy further curtail perfusion; disseminated intravascular coagulation frequently accompanies symmetrical peripheral gangrene (SPG) in these settings [4, 7, 8].
The severity of shock and cumulative vasoactive load amplify risk; patients needing prolonged or very high doses are particularly susceptible [2, 3, 9].
Local factors, including catheter-associated arterial injury or localised flow disturbance, may additionally compromise downstream microcirculation [2, 3, 10].
Clinical consequences
Clinically, patients often develop sharply demarcated dry gangrene of toes or fingers that may remain non-infected yet ultimately require amputation or progress to auto-amputation [3, 4, 11, 12]. Even when infection is avoided, wounds may heal slowly and need prolonged antiseptic care or staged debridement [12, 13]. Beyond the tissue loss itself, there is a substantial functional and psychosocial burden. Patients can face prolonged ICU stays and delayed recovery, with lasting deficits in mobility or dexterity. Reconstructive surgery can improve function but often entails multiple procedures and cannot always preserve length or fine motor capacity, as shown by Deldar et al. and Henn et al. [13, 14].
Legal and ethical implications
When limb loss follows life-saving vasopressor therapy, medico-legal questions inevitably arise regarding the standard of care (dose selection/escalation, timing of de-escalation), documentation of indications and monitoring, and the anticipation/mitigation of risk. Informed consent for this rare but catastrophic complication is rarely feasible in emergencies; nonetheless, documenting family discussions when possible is prudent. Failure to monitor for early ischaemic changes – mottling, delayed capillary refill, acral cyanosis – may be construed as a breach of duty. A COVID-19–related case of vasopressor-induced peripheral gangrene illustrates how such outcomes may precipitate litigation or compensation claims [15]. Broader reviews of SPG in critical illness likewise emphasise diagnostic vigilance, early documentation, and system-level protocols to reduce both clinical harm and legal exposure [16].
Prevention and management
Prevention centres on minimising vasopressor exposure and vigilant bedside assessment. Following contemporary shock guidelines – using norepinephrine as first-line therapy with individualised MAP targets and frequent reassessment – may help limit cumulative vasoactive burden [1]. Clinicians should titrate to the lowest effective dose and shortest feasible duration and avoid combining multiple potent vasoconstrictors when possible. A matched analysis identified the cumulative, weight-adjusted peak dose as an independent risk factor for SPG [9]. Continuous monitoring of peripheral perfusion – skin colour/temperature, capillary refill, mottling scores, Doppler flow – and serial photography can support earlier recognition and improve clinical and legal transparency.
When ischaemia is detected, prompt re-evaluation and tapering of vasopressors are crucial if haemodynamically safe. Reported adjuncts include topical nitroglycerin, local vasodilators or sympatholytics, extremity warming, and (selectively) anticoagulation [3, 11, 13, 17]. If irreversible necrosis develops, most authors advise delaying amputation until clear demarcation to preserve maximal viable tissue [4, 11, 12, 13]. Early involvement of vascular, orthopaedic, and plastic surgery optimises timing of debridement, limb-salvage attempts, and reconstruction; staged approaches and thoughtful stump design can enhance later prosthetic rehabilitation [13, 14].
Outlook and future directions
Despite accumulating case reports and small series, vasopressor-induced acral necrosis remains insufficiently characterised, and no formal guidelines exist. Comprehensive reviews of SPG in critical illness underline the need for prospective registries and risk-prediction models (e.g. integrating cumulative vasoactive load and microcirculatory metrics) to identify at-risk patients earlier [16]. Protocolised monitoring, escalation thresholds, and early surgical consultation can improve outcomes and institutional defensibility. Finally, pragmatic management frameworks – such as structured pathways for vasopressor-induced acute limb ischaemia – and ongoing ICU observational data on SPG–vasopressor associations will continue to refine prevention and treatment strategies [17, 18].
Learning points
Acral ischaemia and necrosis are rare but serious complications of prolonged or high-dose vasopressor therapy, even in the presence of palpable peripheral pulses.
The pathogenesis is multifactorial, involving severe a-adrenergic vasoconstriction, endothelial injury, microthrombosis, and the haemodynamic compromise of shock itself.
Early recognition of mottling, cyanosis, and delayed capillary refill – alongside judicious vasopressor titration and close bedside monitoring – can prevent progression to irreversible gangrene.
Delayed amputation until clear demarcation, combined with multidisciplinary surgical management, optimises tissue preservation and functional outcomes.
Clear documentation, communication with families, and adherence to protocols reduce not only clinical harm but also medico-legal exposure.
Conclusions
Vasopressor-induced acral ischemia and necrosis represent a rare but devastating complication of life-saving therapy in critically ill patients. Our 2 cases demonstrate the interplay of profound shock, cumulative vasopressor burden, microcirculatory failure, and coagulopathy that can lead to irreversible tissue loss despite intact large-vessel pulses. Beyond the immediate clinical consequences – limb loss, prolonged hospitalisation, reconstructive procedures – this complication carries long-term functional, psychological, and socio-legal repercussions. Heightened clinical vigilance, strict adherence to guideline-directed vasopressor use, routine bedside monitoring of peripheral perfusion, and early multidisciplinary involvement are crucial to prevent progression to necrosis. Clear communication with families, timely documentation of decision-making, and institutional protocols for escalation and de-escalation can not only improve outcomes but also mitigate legal challenges. Continued reporting of such cases and development of standardised registries may help identify high-risk patients earlier and guide evidence-based preventive and therapeutic strategies.