Despite the worldwide expansion of endovascular abdominal aortic aneurysm repair (EVAR) and the ongoing accumulated experience, insidious intraoperative complications may infrequently occur. Suboptimal aneurysm anatomy, infrequently combined with endograft placement outside the manufacturer’s instructions for use (IFU), or endograft malfunction, are the main reasons for these complications [1–6]. In these cases, various rescue techniques may be employed to overcome the problem and avoid open conversion, which carries increased morbidity and mortality [7, 8]. One of these complications is the maldeployment of the contralateral limb (CL), resulting in the inability to cannulate. We present a patient who underwent EVAR with the Alto abdominal stent graft system (Endologix, Irvine, California). Maldeployment of the CL due to a lack of filling of CL polymer-based inflatable rings led to a collapsed CL, making the cannulation gate invisible. The problem was solved using a troubleshooting technique employing a unique feature of this graft: the cross-over lumen [9–12].
The patient agreed to the publishing of their case details and images. Ethics committee approval and informed consent have been obtained. A 79-year-old male patient with an asymptomatic abdominal aortic aneurysm, 5 cm in diameter, underwent EVAR with the Alto endograft (Figures 1, 2). His past medical history included arterial hypertension, dyslipidaemia, and diabetes mellitus type II. Pre-emptive embolisation of the left internal iliac artery (LIIA) was performed due to a concomitant, 3 cm, LIIA aneurysm, 4 days preoperatively (Figures 3 A, B). After general endotracheal anaesthesia, access was gained through a femoral cut-down. The delivery system was inserted through the right side, and the main body of the graft (34 mm) was deployed in a ‘ballerina’ position. Unfortunately, no filling was detected in the inflatable polymer-based rings of the CL. Under these circumstances, normal canulation was impossible because the limb and its gate were invisible due to the lack of an incorporated nitinol stent. Only the suprarenal nitinol stent and the polymer rings of the aortic body (AB) and the ipsilateral limb were visible. We used the crossover lumen, a unique feature of the Alto’s platform, to overcome this issue. A 0.018” × 300 cm wire (Thruway, Boston Scientific) was introduced through the crossover lumen port of Alto’s AB handle. The wire was advanced inside the crossover lumen and came out through the exit hole of the lumen at the level of the second (distal) polymer ring of the CL, which lies slightly inside the gate, at its medial aspect. It is important to use an introducer needle at the crossover handle port when introducing this thin wire to avoid damage to its soft tip. From the left side, a large 3D snare (27–45 mm, 120 cm, Argon Medical) was advanced through an 8 × 45 mm sheath (Cordis). The snare loop was deployed below the expected exit of the CL. Once the snare was in position, the 0.018” wire was pushed to come out of the CL gate, and after 3–4 attempts, we managed to capture it with the snare kit. It was essential, at this point, for the operators to collaborate closely. One was feeding the 0.018” wire from the AB’s handle side, while the other was pulling it carefully out from the other side, together with the snare kit. During this process, we focused on the screen to avoid tension on the AB flow divider. Once the 0.018” wire came out of the 8 × 45 sheath, we secured the handling by using a needle handler and removed the snare kit. We kept pulling it until around 1 m of wire was out. After that, we cut the soft tip with appropriate scissors and loaded the sheath dilator over the wire. Then we pushed the sheath (with the dilator) inside the sac until it met the orifice of the crossover lumen and could not be advanced anymore. At this point, the sheath was advanced over the dilator inside the CL to contact the crossover lumen orifice, with the sheath slightly inside the gate. A 0.035” × 260 cm soft wire was inserted parallel to the 0.018” wire (buddy wire) and moved easily through the AB in the suprarenal aorta (Figures 4 A, B). Angiography confirmed the position of the 8 × 45 sheath inside the CL that remained invisible. This was true because early opacification of the CL and AB lumen was achieved. It was clear that the CL, empty of polymer material, was compressed, so we decided to balloon after changing the soft wire to a stiffer one. A long (100 cm) angiographic catheter was introduced over the soft 0.035” wire and exchanged for a Lunderquist 260 cm wire (Cook Medical). Then, a 12 × 40 semi-compliant balloon (Mustang, Boston Scientific) was used to dilate and reshape the CL. After ballooning and securing the Lunderquist wire to be high enough in the aortic arch, we removed the 0.018” wire from the ipsilateral side again with meticulous collaboration of the two operators. One was feeding, the other was pulling back, ensuring NO tension on the AB flow divider. The rest of the procedure was typical, with loading the contralateral iliac limb first, followed by the ipsilateral. Both limbs (22 mm) were deployed slightly higher to the AB bifurcation, to avoid AB kinking, as was planned preoperatively. It was considered that a sac lump would compress the endograft at this point, due to a “barrel-shaped” neck (Figure 5). Because the stent-supported iliac limbs are resistant to kinking, they were placed a little higher to protect the AB. Kissing ballooning of the limbs was subsequently performed. Completion angiography was normal.
Figure 1
3D Reconstruction of computed tomography angiography depicting the abdominal aortic aneurysm

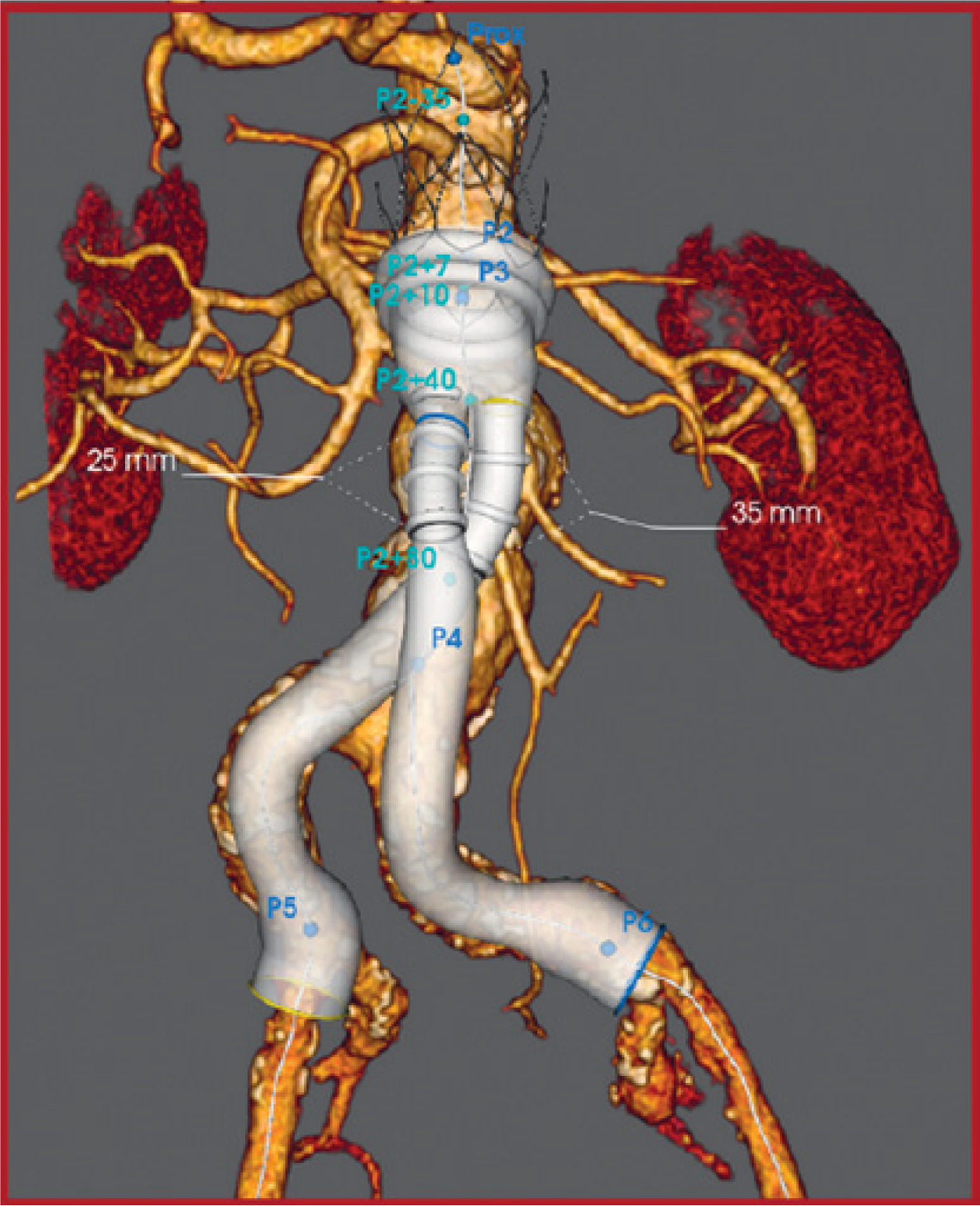
Figure 3
Digital subtraction angiography (A, yellow arrow: left internal iliac artery aneurysm, B, ellow arrow: coil embolisation)
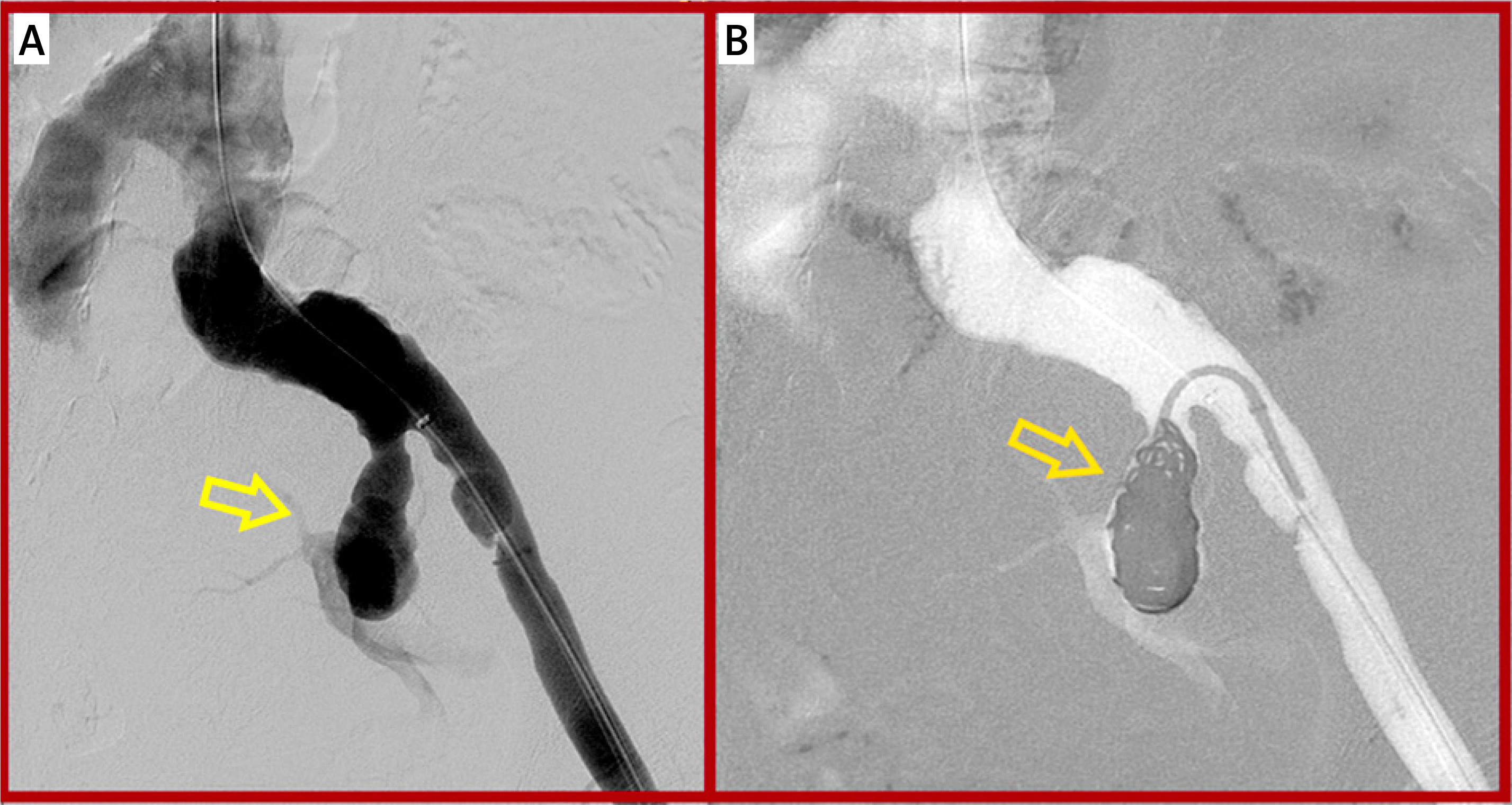
Figure 4
Cannulation in an invisible gate: during insertion, the 8 × 45 sheath essentially stops at the cross-over lumen orifice level, which locates slightly inside the contralateral gate, securing entrance to the limb. Safe advance of a ‘buddy’ soft wire in the gate. A – Intraoperative angiography with the portable C-arm (Philips Endura), B – light-green arrow: assumed external graft compression from neck irregularities leading to obstruction of polymer flow channel (purple arrow), light-blue arrow: the orifice of the cross-over lumen hindering further advance of the 8 × 45 catheter, red arrow: presumed level of the contralateral gate, yellow arrowhead: the cross over wire, orange arrowhead: the ‘buddy’ soft wire after safe cannulation
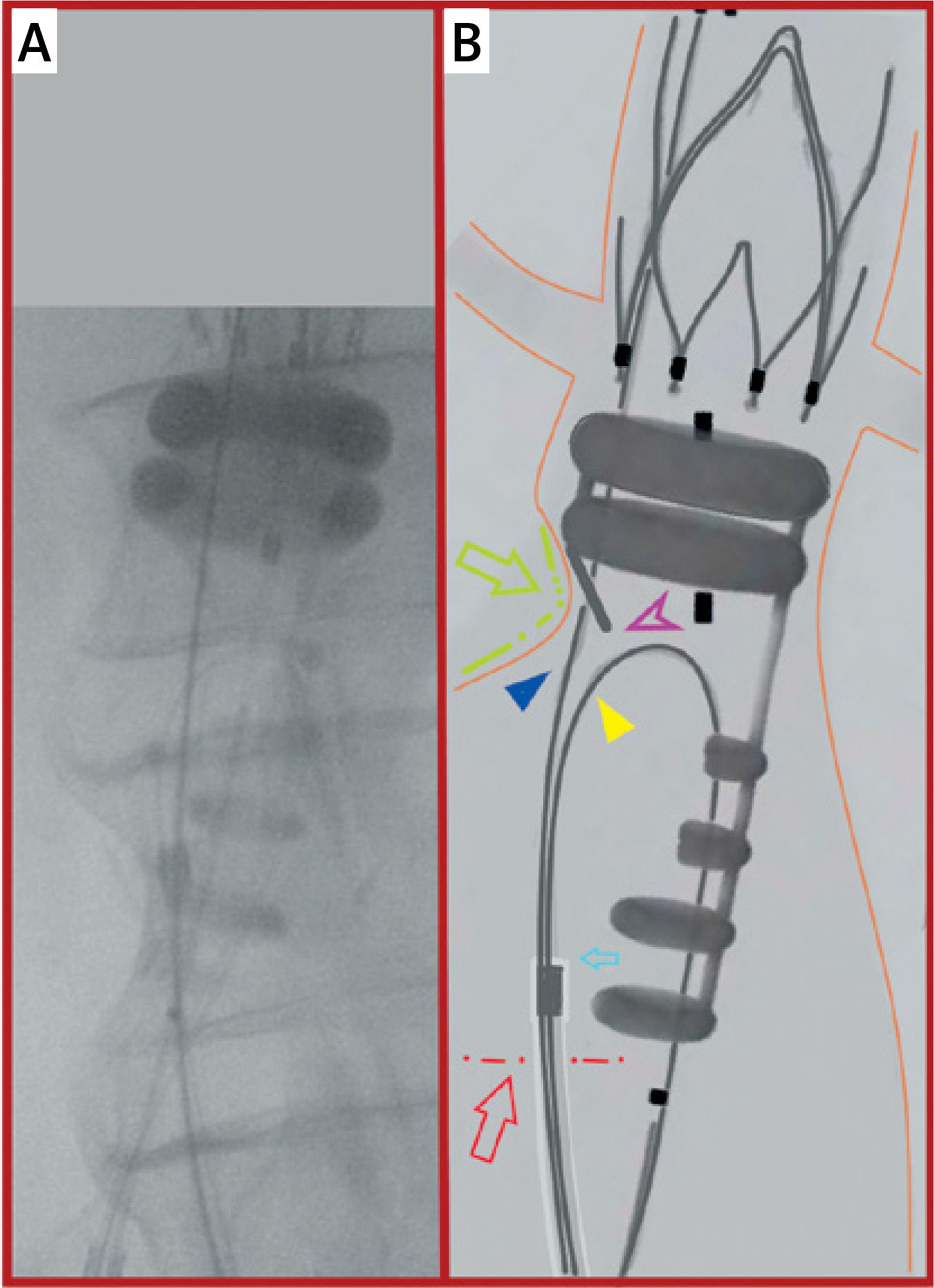
Figure 5
Sagittal plane of computed tomography angiography depicting the sac protrusion (lightgreen arrow) and compression of the endograft’s aortic body. The yellow line delineates the level of the renal arteries

Intraoperative troubleshooting techniques are valuable to treat unexpected problems during the delivery and deployment of endograft devices [13–16]. Unfavourable neck anatomy, small aortic diameter, iliac tortuosity, non-adherence to the specific endograft’s IFU, and inherent device malfunction (including non-meticulous device handling from the operator) are potential risk factors [17–22]. CL gate cannulation difficulties are frequent in modular grafts. The ALTO platform has a unique advantage because it incorporates a cross-over lumen. Through this channel, a tiny wire captured by a snare loop overcomes the inability for normal cannulation. The issue with the Alto platform is that the non-stented AB and its limbs are vulnerable to external compression from neck angulation or sac irregularities. Failure in polymer-based inflatable ring filling may further compromise the ability of the graft and its limbs to expand and remain open. A collapsed, kinked, or twisted CL makes the normal cannulation process impossible [23–26]. In our patient, no filling was detected in the CL, despite the normal filling of the remaining graft. We do not know the exact reason for this malfunction. We hypothesize that a sac wall lump of a barrel-shaped neck compressed the filling channel, obstructing the polymer flow (Figures 6, 7). The CL and the gate remained invisible, as the only gate is the distal CL polymer ring. Troubleshooting salvage techniques regarding the Alto device are scarce in the literature. In one report, radial access and cannulation from above were required in one case with a kinked and twisted CL depicted on intraoperative cone-beam computed tomography. Although the rings were filled (with difficulty), the cross-over lumen was obstructed due to CL kinking. This malfunction was attributed to severe iliac tortuosity, which twisted the CL. The authors considered neck angulation with the verge at the level of the AB flow divider and a small aortic lumen as risk factors for CL collapse [20]. In another report, the iliac limb was mispositioned outside the CL gate after failed cannulation. It was corrected with a repeat accurate cannulation, a balloon to realign the iliac limb, and a bridging stent [19]. This case highlights the need for confirmatory rotational angiography and the rotating pigtail catheter testing even after formal CL cannulation. A bailout strategy using the Alto graft’s integrated cross-over lumen, along with snare-assisted cannulation, can effectively be performed to treat absent CL polymer ring filling. This is an alternative salvage technique that should be employed to avoid open conversion.

Figure 7
Multiplanar reconstruction of the 1 month’s computed tomography angiography. The contralateral limb dilated by the radial force of the iliac limb (yellow arrow)

In conclusion, unexpected difficulties may be encountered during endograft deployment. ALTO endograft’s aortic body is vulnerable to external compression. · Lack of filling of the ALTO limb’s polymer-based inflatable rings may rarely occur. Use of ALTO’s cross-over lumen may overcome this problem.