Introduction
3D printing is an additive manufacturing technology. The methodology involves designing the object in a digital environment, in a computer-aided design (CAD) computer program, which then converts the 3D image file into an standard triangulation language (STL) file to be loaded and read by the printer. The development of 3D printing technology, as stereolithography and the conversion of digital models into physical objects were pioneered in the early 1980s by Charles Hull and others. 3D printers became commercially available in the 1980s, with the market growing exponentially in the 1990s and 2000s [1–4]. Medical applications for 3D printing have been reported since 1990. Stereolithographic modeling of cardiac structures was described by Binder in 2000 for better diagnostic access and surgical planning. In improving healthcare, 3D printing, i.e., the conversion of digital models into physical objects, plays an important and multiple/multifaceted role. It creates bioprosthetic materials, improves surgical planning with a direct impact on the better outcome of surgical procedures, but mainly it is used as an effective educational tool for students and healthcare professionals [3]. 3D printing technology can be used preoperatively for diagnosis and treatment planning, and intraoperatively, with the simultaneous construction of 3D anatomical models for intraoperative use, 3D printing of congenital heart disease models, and digital mixed reality imaging of cardiac anomalies act as valuable complementary tools, providing beneficial information not only in the diagnostic evaluation of young patients with congenital heart disease, but also in their holistic treatment [2, 3]. 3D printing was also useful in the recent pandemic, where the resilience and adequacy of all health systems in developed and developing countries were tested. In recent years, the application of 3D modeling in urology has emerged as an exciting and effective tool in improving the training of novice surgeons, with value in training them in basic techniques in a safe environment. 3D modeling in urology offers excellent preoperative planning services, particularly effective in robot-assisted partial nephrectomy and radical prostatectomy, perfecting the anatomical approach and reducing the time of procedures and the duration of anesthesia for patients [1–3].
This study aims to explore how 3D printing contributes to medical education, surgical planning, and the refinement of surgical techniques in specialties including cardiac surgery, neurosurgery, urology, gastroenterology, and vascular surgery. Particular focus is given to its educational value, its role in improving surgical safety, and its potential for more personalized treatment strategies.
3D printing in medical and anatomy education
In modern medical education, many medical schools, because access to human tissues is not always easy, and with time constraints due to the legal requirement in many countries for cremation of the body within a maximum of 8 years, resort to rapid prototyping techniques with the help of 3D printing. It is known that in the anatomy laboratories of medical schools, medical images, anatomical and organ models, cadavers, and human bones are used.
In the teaching of osteology, anatomical bone models and donated bones do not fully fulfill the teaching purposes, and this is because they do not cover the anatomical variations, different human populations, and the range of bone variation observed in them. Macquarie University and Western Sydney University are using the Artec Spider 3D portable surface scanner and printing 3D bone replicas with Objet Connex and MakerBot Replicator 3D printers [1]. Osteometric analysis of the printed prototypes found that there were no differences in the shape and dimensions compared to real bones.
3D printing in cardiac medicine and surgery
In improving healthcare, 3D printing, i.e., the conversion of digital models into physical objects, plays an important and multifaceted role. It creates bioprosthetic materials, improves surgical planning with a direct impact on the better outcome of surgical procedures, but is mainly used as an effective educational tool for students and healthcare professionals.
In congenital heart disease, congenital heart defects are a major cause of morbidity in pediatric patients. The pathophysiology and anatomy of congenital heart disease and a full understanding of the effects of cardiac dysfunction are an integral and important part of medical education [2]. Representations of congenital defects are critical for understanding, diagnosis, initial management, and better treatment of the underlying disease [3].
3D printing technology can be used preoperatively for diagnosis and treatment planning and intraoperatively with the simultaneous construction of 3D anatomical models for intraoperative use. 3D printing technology is not limited to clinical applications but appears to have a primary role in undergraduate and postgraduate training of healthcare professionals [4]. Aortic stenosis is a congenital disease that accounts for 6–8% of all cases of congenital heart disease and occurs with a frequency of 3–4 cases per 10,000 births. Understanding the disease, education in it, and the breadth of therapeutic options make additive manufacturing technology necessary for the practical training of cardiac surgeons. Thoracic aortic stenosis is mainly located near the entrance to the ductus arteriosus [5].
Training with 3D printed models for congenital heart disease
The study by Barabas et al. used a 3D model of the aorta obtained from a computed tomography (CT) angiography scan of a 3-year-old child diagnosed with congenital aortic isthmic stenosis. Inexperienced medical students were asked to implement four corrective treatment options. The aim of the study was to investigate the effectiveness of 3D printed models in the practical training of students. According to the results of the study, the knowledge and understanding of the participants demonstrated that the 3D printed model is indeed an effective practical training tool in the surgical treatment of aortic isthmic stenosis [6]. The creation of a 3D printed heart model starts from the digital image. The image is obtained from whole heart computed tomography or magnetic resonance imaging (MRI) data sets. Here, each slice is continuous with the previous one with a fixed relationship. The imaging technique chosen depends on the preference of the center, the anatomical structure of interest, and the age of the patient. In young patients, radiation exposure is undesirable, so MRI is preferred. Computed tomography is the imaging technique of choice because it is the easiest way to create a representative model for 3D printing, while echocardiography more clearly segments the heart valves. Once the image is acquired, it is fed into a segmentation software, where the anatomy of interest is delineated and the surrounding tissues are separated. After image segmentation is complete, the resulting stereolithography file is sent to computer-aided design software, where the anatomy is refined [7]. The rapid prototyping of medical devices is facilitated by fused deposition modeling, Polyjet printing, stereolithography, and selective laser sintering [8]. Many materials with previously different properties have been used to print cardiovascular structures, and hard materials depict the anatomy of the heart and great vessels in greater detail. However, models printed with rubber-like materials more accurately and realistically represent the anatomy of the patient’s heart and congenital anomalies such as transposition of the great vessels, tetralogy of Fallot, pulmonary atresia, and hypoplastic left ventricular syndrome. Studies have shown that 3D models of congenital heart disease have improved the initial management and surgical approach to these conditions [9].
Applications in interventional cardiology and valve surgery
3D printing of the aortic root and aortic valve accurately reproduces the patient’s anatomy and helps predict paravalvular aortic regurgitation during transcatheter aortic valve replacement. Medical 3D printing holds significant potential for advancing medical care, particularly in the context of stent implementation. However, the utilization of this technology in the medical field is still in its early stages. Consequently, while some have high hopes for its capabilities, and others remain skeptical, the current state can be best characterized as the “innovation trigger” phase [10].
Educational and surgical training with 3D models
Biglino et al. documented the usefulness of using 3D models to teach nurses in the field of congenital heart disease across a wide spectrum of CHD [11]. 3D visualization of cardiac anatomy and congenital heart disease will be standard practice in a few years, facilitating the adoption of correct intraoperative decisions and conservative interventional therapeutic solutions. In complex congenital heart diseases involving anatomical abnormalities of the heart cavity and great vessels, cardiac magnetic resonance, computed tomography, and 3D echocardiography are crucial in understanding the image. However, imaging with these conventional techniques is limited when the variations in cardiac anatomy are complex.
In these cases, the recent development of the creation of a 3D cardiac model promises a clearer description of the congenital heart disease of each patient [12]. The first application of 3D cardiac printing was aimed at the design of the repair of congenital anomalies [13]. In addition, 3D printed models have the potential to serve as unique educational tools for health professionals [14]. Parents develop a better understanding of the condition of young patients, improve communication with cardiologists, and have a positive effect on the psychological adaptation to their children’s disease [15]. The most important limitation of 3D printing is the immobility of the printed model. No information is obtained about dynamic circulation. The printing materials do not reflect the range of elasticity of the heart muscle. 3D printing of the anatomy of congenital heart disease is limited and has disadvantages. However, it aspires, although limited, to be useful in the preparation and success of percutaneous therapeutic invasive interventions [16]. 3D printers became commercially available in the 1980s, with the market growing exponentially in the 1990s and 2000s. Medical applications for 3D printing were reported at least as early as 1990 [17]. Stereolithographic modeling of cardiac structures was described by Binder in 2000 for improved diagnostic access and surgical planning [18]. Data sets derived from computed tomography and magnetic resonance imaging were subsequently used to investigate 3D printing of heart and other organ models.
Advances in printing materials have facilitated the production of flexible photopolymerizable resin materials with textures and physical properties that mimic human tissue. This development has spurred the development of new complex models of cardiac chambers and associated vessels for surgical learning and practical training. Pioneering visionaries such as Pedro del Nido, Erle Austin, Shi-Joon Yoo, and Glen Van Arsdell have encouraged and created sophisticated models of hypoplastic left heart syndrome, transposition of great vessels, and tetralogy of Fallot [19, 20]. Training with 3D models improves the ability to learn surgical timing and steps, the correct and efficient positioning of the surgeon’s body, the refinement of skills in the fabrication of custom-made grafts, and the skill and accuracy of anastomoses. Training with 3D models probably nullifies the value of learning curves [21].
Van Arsdell et al. liken surgical training to a musician’s rehearsal before a performance. No professional musical performance is successful if the music is not performed flawlessly in the correct rhythm. Similarly, the technique of surgical access and reconstruction must be excellent and efficient [22]. Hussein et al. at the University of Ontario, Canada, included twelve 3D printed surgical heart models in the annual internship program for young congenital heart surgeons. Trainees demonstrated a 25% improvement in all assessed procedures, demonstrating the value of training on 3D printed cardiac models [23].
Digital archiving and interactive 3D atlases
The anatomy and pathology of postmortem cardiac specimens with congenital anomalies are useful in practice and education. However, such specimens are rarely obtained, and those that are obtained are not fully utilized due to deterioration during preservation by the effects of formalin. Toba et al. at Boston Children’s Hospital digitally archived the specimens with microfocus computed tomography and then reproduced them using a 3D printer [24]. With the printed models, they created an interactive 3D online atlas that was archived and available to any interested surgeon on the Internet (https://www.sketchfab.com/heartmodels/collections).
Certification and evaluation of cardiac surgeons using 3D models
Obtaining the specialty of cardiac surgery in the United States of America requires passing an examination (American Board of Thoracic Surgery – ABTS). Passing a written (Part I) and oral (Part II) examination is required. Oral examinations test candidates on their decision-making skills. But would the candidates’ examinations be more complete if they also included a practical examination? The work by Hussein et al. utilizes a three-dimensional model of transposition of the great vessels and trains young congenital heart surgeons in the repair of this anomaly [25]. Candidates’ performance is assessed and scored accordingly. The model is easily adapted to the practical examination for obtaining the specialty title.
Case study: tetralogy of Fallot and 3D educational models
Tetralogy of Fallot is the most common cyanotic congenital heart disease. Tetralogy of Fallot consists of three individual structural defects: right ventricular outflow tract stenosis and possibly pulmonary valve stenosis, a large hole in the ventricular septum and ventricular septal defect, right aortic displacement above both ventricles, and a fourth, right ventricular hypertrophy resulting from the other three. Zhao et al. studied the effect of 3D printing of the congenital cyanotic heart disease, tetralogy of Fallot, on teaching students [26]. The printing of the 3D model of tetralogy of Fallot was based on a typical case with computed angiography imaging data processed with special software (Mimics Research 20.0) and exported as stereolithography (STL) files. Experienced cardiac surgeons validated the anatomical and morphological accuracy of the digital model. The STL files were then imported into a 3D printer (J401Pro; Sailner 3D Technology) for printing color models. Four models were created, two with rigid and two with flexible materials. Two groups of 30 undergraduate students were taught from the printed models of the tetralogy of Fallot. An excellent understanding of the anatomy and pathophysiology of the congenital anomaly was found. The study concludes that the integration of 3D printed models is feasible and effective. The success of the method justifies its widespread application in medical education on complex congenital heart defects. It is now common knowledge that a thorough understanding of the detailed anatomy and morphology of congenital heart defects is crucial for their successful management. Imaging studies such as CT and MRI fail to capture the depth of the organ. 3D printing represents a significant advance in imaging the intracardiac structures and extracardiac anatomy in detail [27].
Virtual and mixed reality in cardiac education
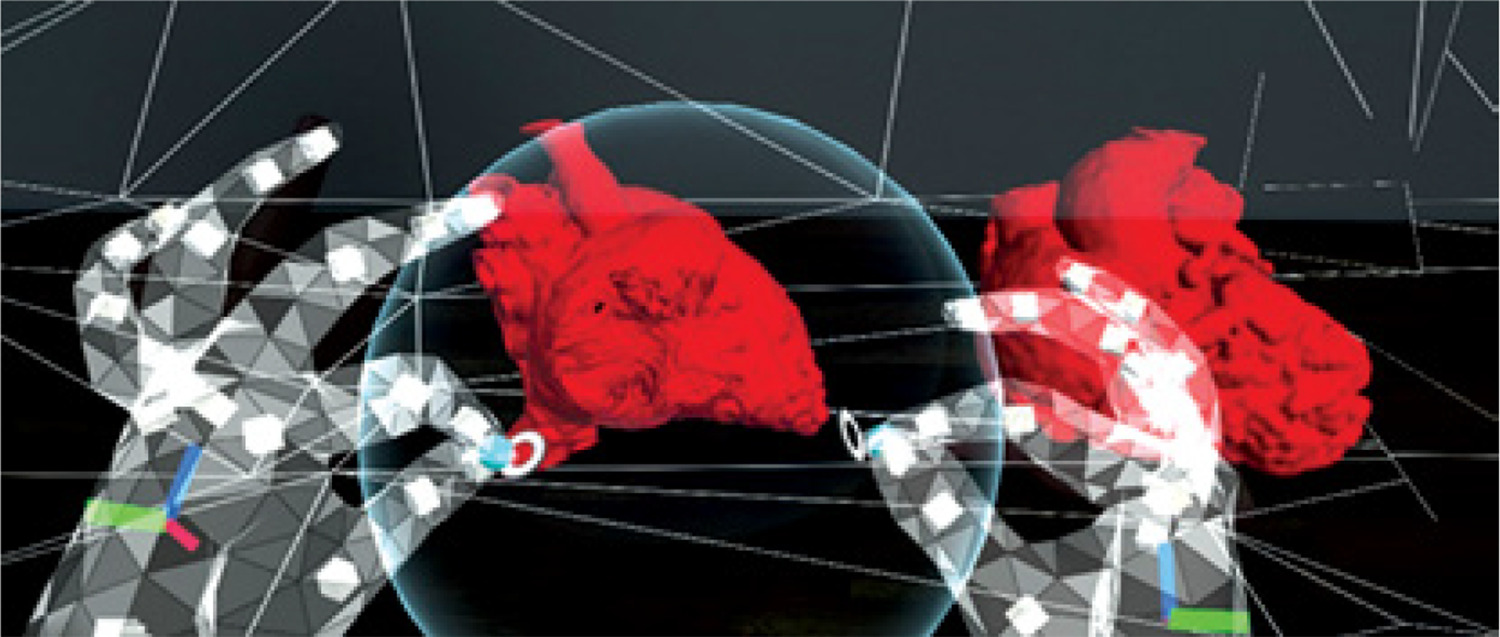
Virtual Reality (VR) captures 3D models of the heart and vessels and allows cardiologists and cardiac surgeons to explore the unique anatomical complexity of each congenital defect beyond conventional methods [28]. Applied VR facilitates anatomical diagnosis, detailed visualization, training, simulation, and design of cardiac reconstruction [29, 30]. Virtual reality facilitates intuitive understanding of anatomical relationships and surgical reconstruction, improving learning, educational, and technical outcomes in congenital heart disease. The Stanford Virtual Heart is a virtual reality training tool. The complex anatomy and pathophysiology of the heart are presented in all its obvious and hidden details by this immersive technology [31] (Figure 1).
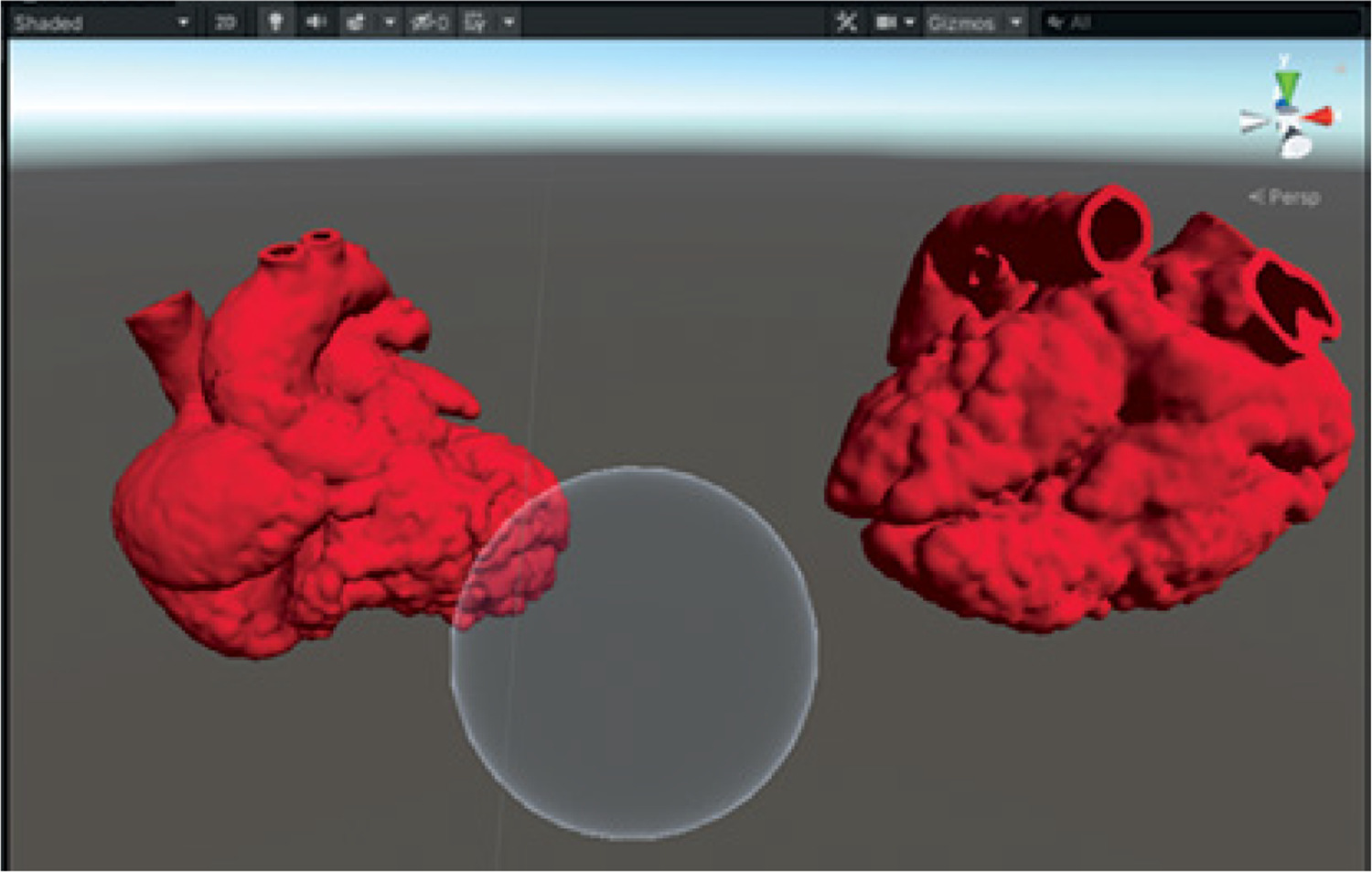
Understanding the complex anatomy and morphology of congenital heart disease requires spatial orientation and perception. Brun et al. compared the experience and retention of knowledge of students who were taught the anatomy of congenital heart defects using 3D printed models, mixed reality visualization, and 2D CT angiography images. Students performed better with the holographic visualization model [32]. In a similar study, Lau et al. from the University of Perth, Australia, recruited 34 cardiologists to evaluate 3D and mixed reality models of cardiac chambers with congenital heart disease for optimal anatomical and morphological learning and preoperative planning [33]. Starting from standard DICOM images and creating mixed reality renderings, the digital heart models were transferred to the Blender Foundation, Amsterdam, the Netherlands, for optimization of holographic rendering. The Blender Foundation is an independent non-profit organization that aims to provide complete and free 3D creation applications. The Mixed Reality application was developed with the help of the Unity engine, a real-time 3D development engine that allows artists, designers, and programmers to collaborate on Windows, Mac, and Linux programs to create stunning immersive and interactive experiences. From the Unity application, the two optimized models were loaded onto the screen. The intense color of the models gives a more realistic appearance. A sphere was then added as a segmentation tool to the models to visualize the internal cavities. Figure 2 shows two-colored heart models and the sphere (Figure 2).
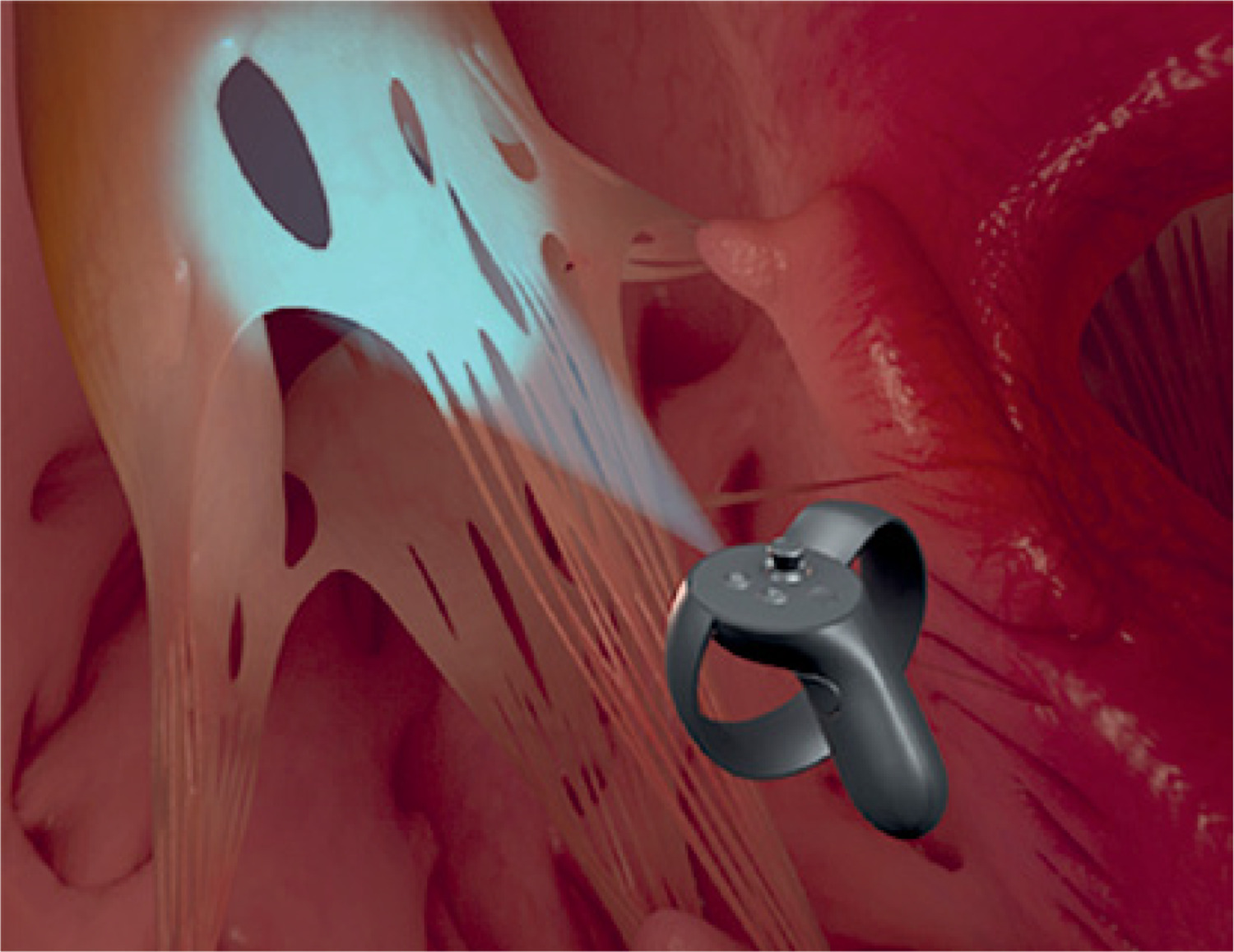
The sphere, with the assistance of Microsoft HoloLens 2, the first fully autonomous, reliable holographic computer, cuts out the models at different sizes to visualize the endocardial structures, valves, orifices, papillary muscles, and congenital anomalies (Figure 3).
The authors demonstrated that ultimately, 3D printing of congenital heart disease models and mixed reality digital imaging of cardiac anomalies act as valuable complementary tools, providing very useful and beneficial information not only in the diagnostic evaluation of young patients with congenital heart disease but also in their holistic management.
Patient education and communication improvement
Cardiac surgeries cause uncertainty and significant anxiety in patients, who expect comprehensive information from surgeons about the type of surgery, postoperative care, and overall hospital stay. Excellent communication between doctors and the patient environment – and especially with the patients themselves – ensures better care [34].
However, despite the briefings and presentations with pre-printed brochures and instructions, approximately 60% of patients are unable to recall all the information due to anxiety [8].
Studies suggest that visualized information yields better results. Therefore, informing patients with 3D printed cardiac models or visualizing pathology and surgical repair on virtual reality screens has the potential to provide convincing information and patient participation [35].
A study by Grab et al. involving 34 3D models and 32 virtual reality models that helped in the education and information of patients undergoing cardiac surgery demonstrated that while they did not offer significant benefits in reducing patient anxiety, they nevertheless recorded significant satisfaction with the information provided – 86% for 3D printing and 92% for virtual reality [36].
3D printing in cardiac tumors and vascular interventions
Cardiac tumors are rare, occurring at a frequency of 0.02%, and most of them are benign (75%). They are mainly myxomas (50%), sarcomas, rhabdomyomas, schwannomas, fibromas, and metastatic tumors. The size, shape, location, and relationship of cardiac tumors to surrounding tissues significantly affect the hemodynamics of the heart. Surgical resection is considered the treatment of choice. Preoperative imaging with transthoracic echocardiography, computed tomography, cardiac magnetic resonance imaging (MRI), PET/CT, and coronary angiography significantly guides the management [37]. However, compared to traditional diagnostic imaging techniques, 3D printing technology creates customized models capable of facilitating the correct selection of therapeutic strategies. 3D printed models are valuable teaching tools for students and physicians. Therefore, the technology of 3D printing of the heart and its pathology is considered essential in the clinical diagnosis and planning of surgical treatment of patients with cardiac tumors [38]. The placement of the first self-expanding stents in the coronary arteries by Puel and Sigwart in 1986 brought about a revolution in the treatment of heart disease [39, 40]. In recent years, reasonable concerns have been expressed about the possible effects of permanent metal structures within the coronary arteries. Thus, fully bioresorbable stents (BRS) were developed, which provide mechanical structural support of the coronary vessels and local drug release like classic metal stents during the first year, but are then absorbed, restoring the normal size of the coronary lumen and allowing surgical revascularization if required. Many authors have developed 3D printed coronary artery stents with bioresorbable polymer materials [41]. 3D printing technology offers precision, personalized treatment for each patient, training for interventional cardiologists in models with complex coronary pathologies, and breakthrough solutions for revascularization and maintaining a smooth vascular lumen [42, 43].
3D printing in reoperations and surgical simulation
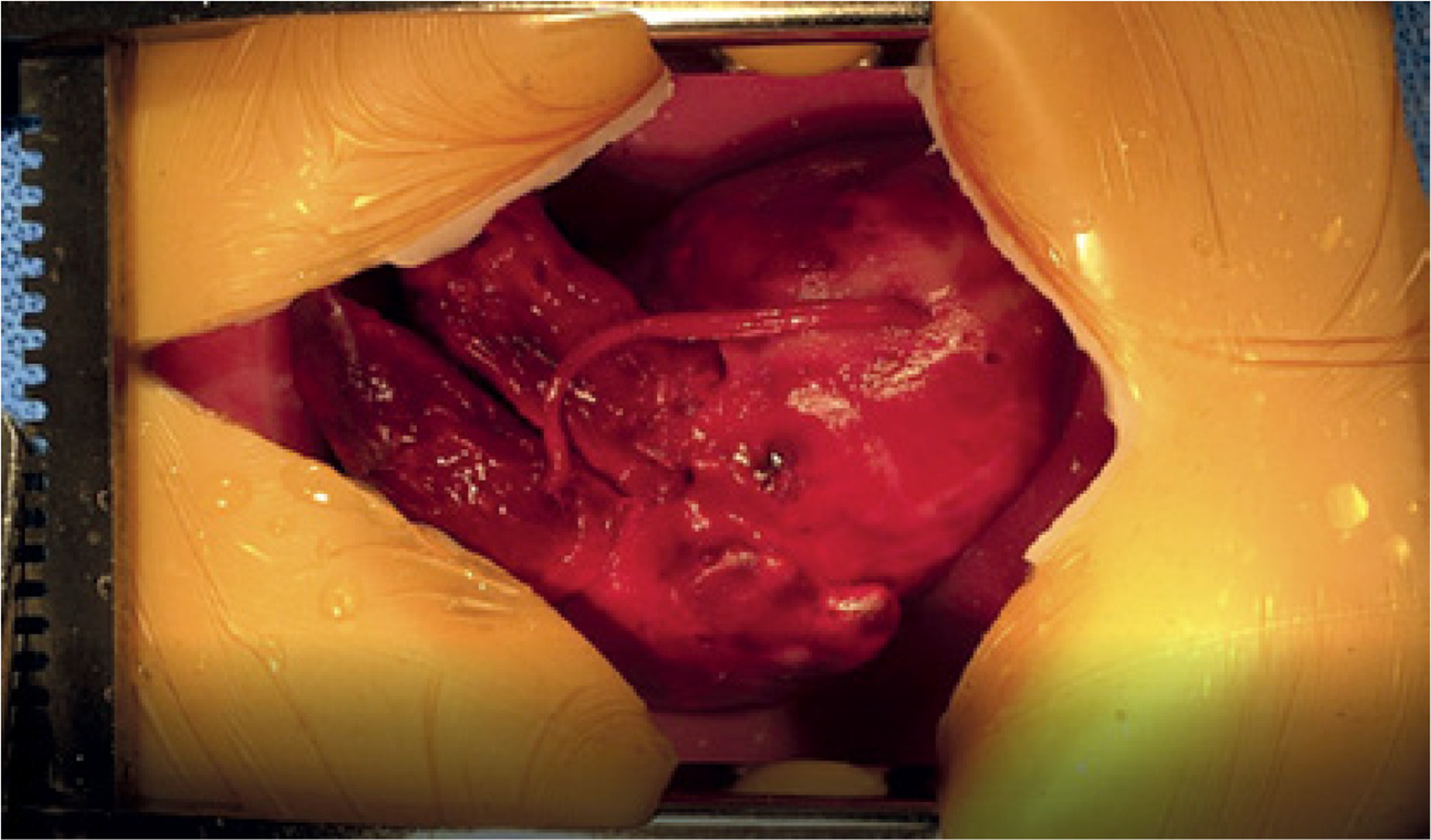
Reoperations in cardiac surgery are complex and high-risk, since the development of scar tissue, strong and stable adhesions, and altered anatomy of the area due to the previous operation increases mortality from 2% in the first operation to 6% in the repeat intervention [44]. 3D printing is a valuable guide for understanding the anatomy of the visual and tactile representation of the operated heart and a great guide for surgeons in planning reoperation and in training residents in complex cardiac surgeries [45]. Saba et al., to provide educational competence to resident cardiac surgeons, developed a technique that uses 3D printed hydrogel models and created a platform for simulating coronary vessel anastomoses. Trainees were trained in the application of peripheral anastomosis in the left anterior descending branch of the coronary artery and central anastomosis of the hydrogel graft in the ascending aorta. Participants noted an improvement in technical skills and agreed to the inclusion of this educational tool in their curriculum [46] (Figure 4).
Figure 4
Educational application of peripheral anastomosis in the left anterior descending branch of the coronary artery and central anastomosis of the hydrogel vascular graft in the ascending aorta
Endovascular surgery and vascular surgery require excellent anatomical knowledge, meticulous skills, precision, and appropriate planning to ensure optimal benefits for vascular patients [47]. The incorporation of 3D printed vascular surgical models is used in the study of vascular anatomy and its variations, in understanding the pathology of vascular diseases, in planning complex vascular surgical procedures, in the practical training of young surgeons, and the education of undergraduate and postgraduate students [48].
Thoracic wall reconstruction and chest deformities
In a major systematic review on the application of 3D printed models in education, design, practice and simulation in vascular surgery, carotid, aortic, aortoiliac bypass, thoracic and abdominal aortic aneurysms, Catasta et al. analyzed 24 studies out of 934, regarding diagnostic imaging technique, image processing software, 3D printing technologies and materials, application of 3D printing technology in vascular surgery, 3D printed models in vascular education and 3D printed models in surgical vascular planning [49]. Training on 3D models of aortic aneurysms repaired with endografts boosted surgeons’ confidence by 40% [50]. While planning vascular surgeries using 3D models of abdominal vessels applied by a robot showed satisfactory results [51]. Vascular surgeries based on printed 3D models were completed accurately without complications [52]. Chest wall malformations – pectus carinatum, pectus excavatum, pectus arcuatum, Poland syndrome – extensive injuries that cause bone defects, and radical removal of tumors and other neoplasms, require rehabilitation with complex prostheses during surgical procedures. Therefore, they must be personalized and adapted to the respective pathology. 3D printing of chest wall prostheses promotes the understanding of the anatomy and physiology during respiratory movements of the chest, contributes to the surgical training of new surgeons, improves the form and function of structures, facilitates the planning of operations, and restores respiratory function. 3D technology offers an interesting alternative by printing an ideal prosthetic model that integrates into the thoracic defect with the appropriate motor function [53–58]. In 2021, Martinez-Ferro et al. published cases with complex chest wall deformities (pectus arcuatum, Poland syndrome) that were restored with 3D printed models. The restoration included preoperative planning, printing of implants with polylactic acid and titanium, simulation of the placement of thoracic and retrosternal implants to ensure the stability of the rib cage, and finally, complete and functional remodeling of the thoracic cavity [59]. Tan et al. applied 3D technology to chest wall and rib cage tumors in 2020 and found the value of accurate R0 resection, less blood loss, reduced surgery time, reduced recovery time, and shorter hospital stay [60]. Also, 3D technology using titanium alloy as the material of the sternum reconstruction model proved to be a successful and effective method with satisfactory histocompatibility, remarkable stability, and improved respiratory function after chest wall reconstruction. Wang et al. in 2024 treated seven patients with neoplastic sternal tumors (mainly fibrosarcoma and carcinosarcoma) with tumor removal over healthy margins and reconstruction of the defect with a titanium alloy prosthetic model printed on an electron beam melting (EBM) Q10 3D printer [61].
Applications for pulmonary and airway surgery
The authors conclude that 3D printing facilitates learning to repair sternal defects, contributes to accurate preoperative planning of the procedure, facilitates complete resection of sternal tumors, and offers safe and effective chest wall reconstruction. In Spain, Zabaleta et al. consider it both feasible and necessary to develop and operate a 3D printing laboratory involving an interdisciplinary team of biomedical engineers, physicians, thoracic surgeons, anatomists, and radiologists working in effective cooperation to produce anatomical and personalized educational and applied pathological pulmonary models [62]. In patients with benign tracheal stenosis with a lumen diameter of less than 5 mm who require urgent endoscopic treatment with stent application, the 3D model proves useful for selecting the appropriate length, diameter, and shape of the stent and for determining the exact distance of its proximal end from the vocal cords. Furthermore, in the case of airway stenosis, the 3D printed and customized model is an enlightening tool for training and consolidating endoscopic manipulations and skills for young doctors [63]. Miao et al. believe that the use of colorful 3D printed high-precision lung section specimens in the experimental teaching of respiratory system anatomy can improve the effectiveness of teaching performance and therefore deserves to be adopted and promoted in clinical and experimental anatomy courses [64]. Liu et al., using 3D printing technology, developed a bronchial tree model with high-fidelity simulator characteristics designed for educational endoscopic navigation in the bronchial “pathways”. In total, 160 h were required for the final assembly of the bronchial simulator (Figure 5).
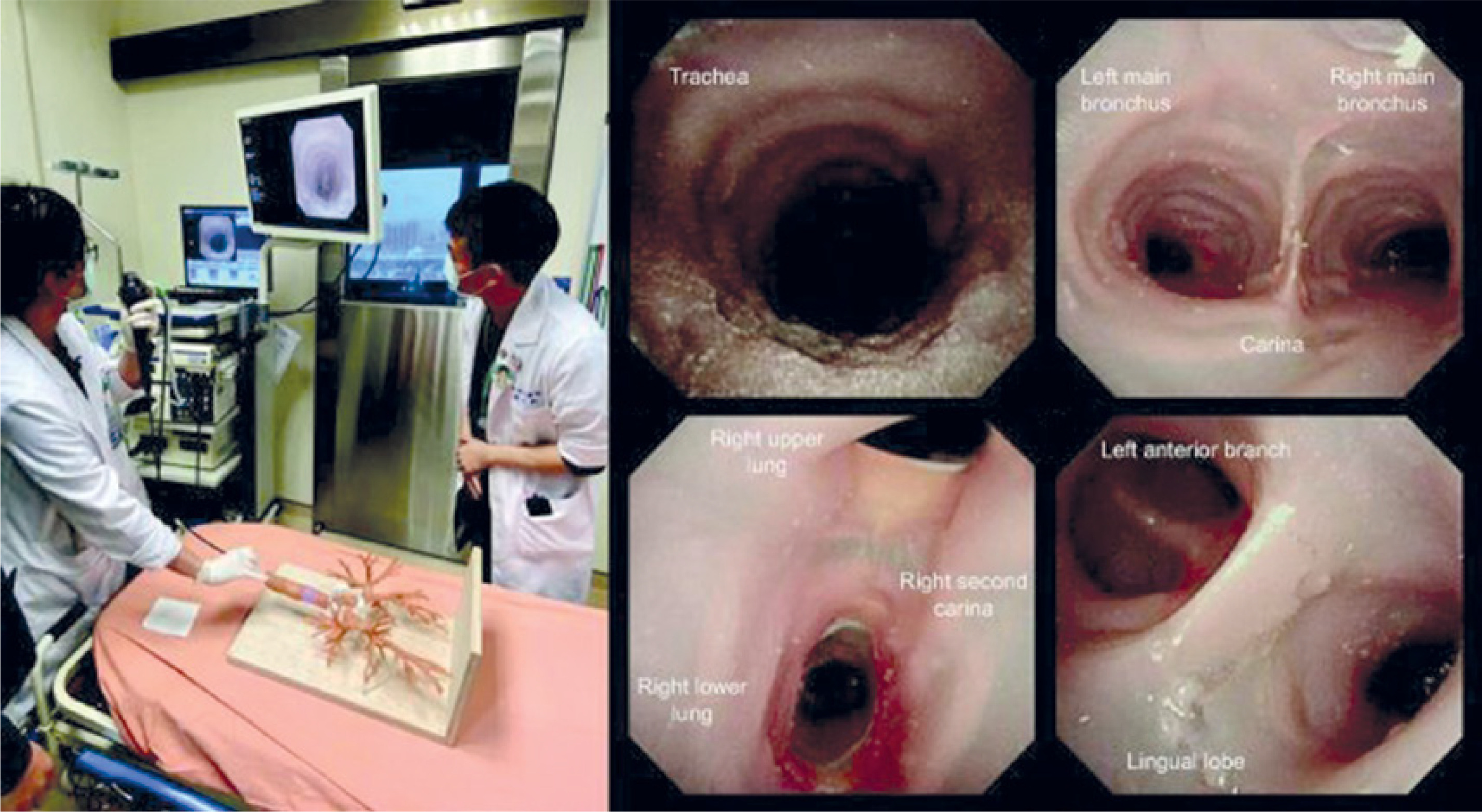
The authors argue that high-fidelity 3D bronchial tree simulators contribute to the learning and clinical training of even inexperienced trainees in a safe and controlled environment [65].
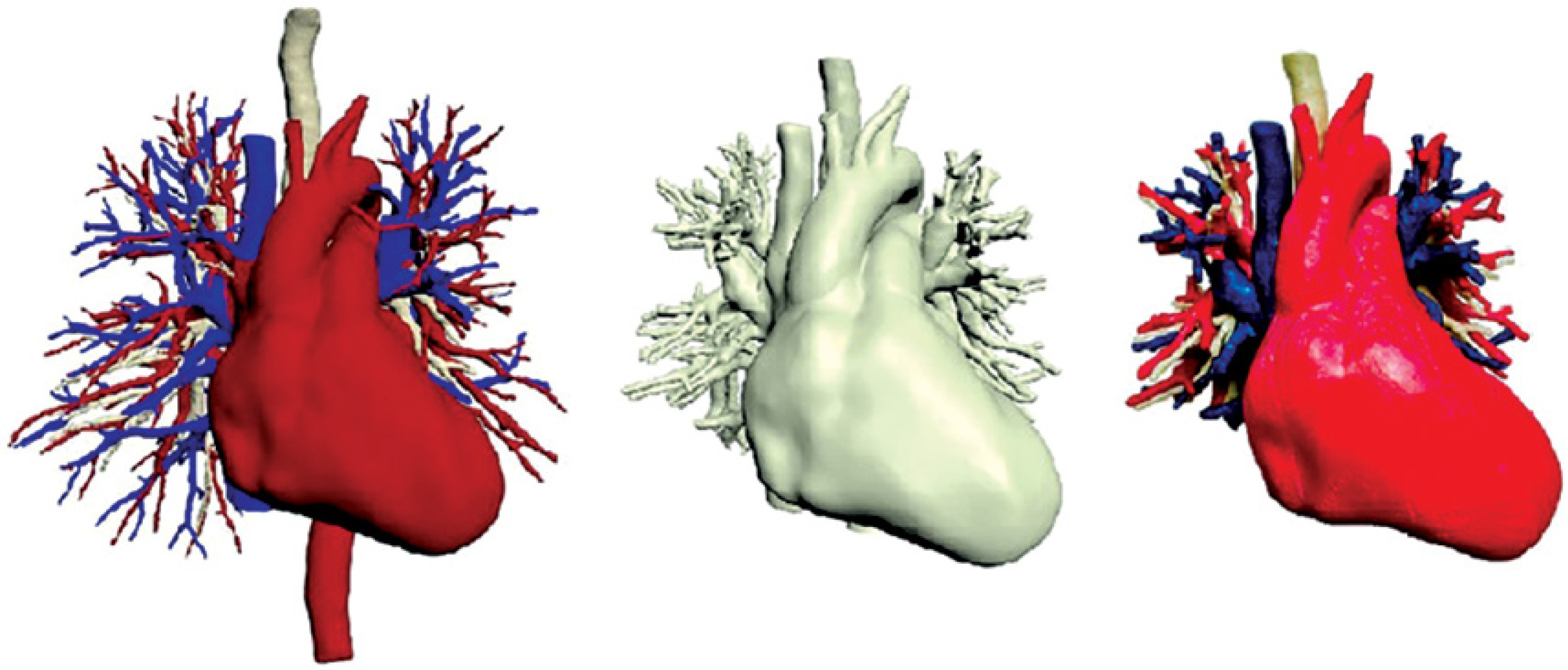
Lung anatomy is taught in medical schools mainly from 2D anatomy textbooks. However, the complexity of the anatomical structures of the tracheobronchial tree, which runs parallel to the branches of the pulmonary artery, which originate from the right ventricle, and the branches of the pulmonary veins, which empty into the left atrium, and their subdivisions into the corresponding bronchopulmonary segments, constitutes a 3D labyrinthine network of bronchi, arteries, and veins. Also, the practical training of thoracic surgeons from the open method to thoracoscopic and robotic surgery encounters limitations in intraoperative tissue mobility and tactile feedback of anatomical structures. In addition, the ever-increasing trend of treating lung diseases with smaller resections (segmentectomies), which spare lung parenchyma and therefore preserve equivalent postoperative respiratory function, requires detailed anatomical preoperative study of lesion localization and precise planning of intraoperative timing of the operation. Considering these data, Dutch researchers led by Meershoek developed, based on CT images, separate three-dimensional models of the pulmonary arteries, pulmonary veins, trachea, heart, and bronchi [66]. The 3D models were then combined into the final 3D anatomical model, which was printed in Utrecht at a 1 : 1 scale with an Ultimaker S5 printer (Figure 6).
Figure 6
The 3D models combined into the final 3D anatomical model of the heart, bronchi, arteries, and pulmonary veins
The model was tested in three groups of ten surgeons of increasing experience who decided to surgically treat patients with peripheral nodules of less than 20 mm. The authors found that in surgeons with medium and less experience, the 3D model improved the accuracy of anatomical localization by 46% and reduced the time by 85 s. The study confirms that 3D printing is beneficial for thoracic surgeons in understanding the anatomical relationships in the complex anatomy of the lung and more accurate preoperative planning of these extremely demanding surgical procedures of segmentectomies and/or lobectomies.
Hepatic and biliary applications
The complex anatomy of the liver, pancreas, and biliary tree and the anatomical relationships between them, as well as the complexity of the pathology of this region, led Chedid et al. to investigate the possibility of creating and applying 3D printed models in teaching the anatomical relationships of the liver parts. Indeed, they created customized 3D models that were tested in a crossover test by 116 physicians. The authors found that the accuracy in identifying liver parts was higher with the 3D model (77% vs. 69%), which was statistically significant (p = 0.05) [67]. Kong et al., in a similar study with 3D printed models, agree that 3D printing provides tissue tactile properties, facilitating medical students’ learning of complex liver anatomy by making it easier to understand the 3D perspective [68]. According to Valls-Esteve et al., the average cost of materials and labor for 3D printing is estimated at 540 euros [69]. In a review published in 2024, Shi et al. argue that 3D printed models of the liver, pancreas and biliary tree facilitate preoperative informed consent of the patient and his/her relatives for complex surgical procedures with their possible complications, offer improved training to students and surgeons, ensure preoperative planning and intraoperative navigation and contribute to the printing and production of implants (stents) in the biliary tree [70]. Precise laparoscopic resection of liver tumors ensures faster recovery and a more favorable prognosis for patients. However, there are great difficulties in applying minimally invasive techniques due to the complex anatomical structure of the liver and its complex pathology. The liver bleeds easily, and the conversion rate to open surgery exceeds 40% of cases [71]. Therefore, the development of an accurate laparoscopic surgical plan for specific and complex liver and biliary diseases is imperative. The 3D printing technique developed by Yao et al. converts 3D reconstructed images into real objects, allowing clinicians to observe the complex intrahepatic blood vessels and bile ducts directly, thereby improving the understanding of the liver’s complex anatomy and enhancing the accuracy of liver resection. The 3D printed model allows the evaluation of the normal liver volume and contributes to the safe performance of liver surgery [72]. The 3D printed model also helps to improve understanding of lesion morphology and surrounding normal tissue, and provides real-time intraoperative navigation to preserve more normal liver tissue and avoid postoperative failure [73]. The researchers conclude that 3D printed liver models reduce surgical risks and improve the safety, effectiveness of surgical resections [74]. The study by Cheng et al. aimed to investigate the effects of a patient-specific 3D printed liver model in clinical training of hepatocellular carcinoma. A total of 62 trainees were examined on liver tumor locations, associated vessels, and surgical planning. 3D printing was superior in terms of accurate tumor location, vessel identification, anatomical understanding, and intraoperative planning. The authors conclude that clinical teaching in 3D printing significantly improves professional theoretical levels, enhances clinical thinking and ability, and yields remarkable teaching results for trainee surgeons [75].
Simulation-based education in liver and biliary surgery
Simulation-based medical education models and 3D printed models are increasingly used in continuing medical education and clinical training. The study by Bao et al. aimed to evaluate the educational benefits that trainees receive from the use of new 3D liver models [76]. DICOM imaging data were analyzed, and the liver parenchyma with its corresponding artery, hepatic vein, portal vein, gallbladder, and bile duct were calculated and exported as STL files. The digital liver model was printed in 14 h and at a cost of approximately 250 euros using the PolyJet3D technology of the Stratasys J850 printer with a transparent material. The study concludes that education with 3D models facilitates preoperative understanding of liver tumors and surgery and are useful and effective teaching tools in the quiver of continuing medical education. Fifteen general surgeons with no prior experience in laparoscopic choledocholithiasis were trained on a 3D printed model. Those trained on the 3D model were found to complete the anastomosis in a shorter time and showed improved surgical skills [77].
Laparoscopic exploration of the common bile duct for stone removal is not easily mastered by inexperienced surgeons. To better understand this approach, Yang et al. investigated the effectiveness and practical application of a color 3D printed anatomical model based on radiographic images. Twenty trainees were randomly divided into two groups. One group was trained on a 3DP/3D printed model and the other on a traditional laparoscopic simulation. After a 4-week training course, the 3DP/3D printing/3D team demonstrated significant improvement in understanding key points of the surgical procedure, excelled in basic surgical skills, and demonstrated greater intraoperative confidence [78]. Another study on the educational contribution of a 3D printed intra-abdominal-intracorporeal model of laparoendoscopic entero-enteric anastomosis found that the model significantly improved surgeon performance while also reducing hospital stay and healthcare costs [79]. Choledocholithotomy is the surgical decompression of choice for diseases that obstruct the biliary tree. Experience and surgical skills eliminate the possibility of postoperative cholangitis, bile duct stricture, biliary fistula, and choleperitoneum. Xia et al. supervised the construction of a three-dimensional educational model, and fifteen trainee surgeons performed choledochojejunostomy and were evaluated based on tissue respect, duration of anastomosis completion, adequacy of organ manipulation, and anastomotic integrity. The authors concluded that the 3D printed model ensures that trainee surgeons acquire complex surgical skills, shorter learning curve, and reduced risk of complications [80]. Preparation of the hepatic artery is a critical surgical step in the management of tumors of the portal tract, pancreas, and biliary tract. Medical manipulation in the intraoperative field can lead to injury to the hepatic artery. Rapid intraoperative hemostasis and repair of the hepatic artery are skills of experienced surgeons. However, few surgeons are familiar with the laparoscopic repair of the arterial lesion. 3D printed models were tested by inexperienced surgeons simulating hepatic artery hemorrhage. The trials have shown that they significantly improve surgeons’ skills in managing hepatic artery bleeding [81].
Orthopedic and trauma surgery applications
The design and printing of 3D fracture models are useful in visualizing and understanding fractures in the simulation of osteosynthesis and teaching the planning of surgical approaches [82]. In particular, the use of 3D printed bone fractures in the preoperative planning of comminuted intercondylar fractures of the humerus has been shown to reduce the duration of surgery, the volume of blood loss, and the number of intraoperative fluoroscopy images [83]. It is estimated that over 50% of orthopedic surgeons use 3D printed bone fracture models in their surgical training or preoperative stabilization planning [84].
Neurosurgery and skull base applications
In developing countries, neurosurgical cases are difficult to treat due to the limited number of specialized and trained neurosurgeons. To address this issue, there is an urgent need to train more specialized surgeons. However, the traditional method of skill acquisition in neurosurgery is disadvantageous, as it increases the risk of complications and patient mortality. It seems that 3D printing of anatomical regions of the central nervous system improves the level of training of new neurosurgeons while increasing the skills of experienced neurosurgeons in performing complex neurosurgical procedures [85]. Although 3D models for neurovascular and skull base techniques have been validated as useful and functional, those used for epilepsy and brain tumor surgeries are not yet described as highly effective. Therefore, 3D printing technology that simulates detailed anatomical and neurological structures is currently in the development stage [86]. Is every idea conceived by the human mind an achievable goal? The idea of printing 3D objects from digital files with the help of a printer that deposits condensed polymers in a controlled sequence in layers that aggregate to create solid objects is now a breakthrough innovation that borders on the industrial revolution. Although 3D printing technology has contributed to the evolution of manufacturing for many years, it is only recently that the cost of 3D printers has fallen to levels accessible to users. 3D printing is used to produce personalized and fully understandable models of patients’ anatomy, as well as to print customized prostheses and implantable medical devices [87]. In neurosurgery, custom bone grafts are employed to repair cranial defects and anomalies, while anatomical 3D sections of the spine are used both for training and surgical planning of these conditions [88]. According to Ploch et al., advanced techniques based on magnetic resonance imaging (MRI) are used to create deformable human brain models that provide tactile feedback like actual brain tissue [89]. They convincingly demonstrate the usefulness of 3D prototypes in neurosurgical training, mainly in understanding anatomical relationships, in live teaching of students, and in better informing neurosurgeons. The incidence of brain aneurysm rupture is 0.01% annually [90]. It is estimated that 5% of the general population has an unruptured brain aneurysm [91]. The mortality rate of ruptured cerebral aneurysms is 45% [92]. The treatment of a ruptured cerebral aneurysm is the surgical occlusion of the aneurysm neck with clips. This is a surgical procedure that requires a thorough understanding of the aneurysm’s shape, its relationship to adjacent vessels and nerves, and combines experience and knowledge, and tests the surgical skill and acuity of the neurosurgeon. Neurosurgeons are trained for seven years, while specialization in cerebral vessels may require an additional 2 years of training and practice [93]. Young and inexperienced neurosurgeons have better training and practical training/education with the help of a cerebral aneurysm simulator printed by a desktop 3D printer based on radiological and angiographic imaging data, computed tomography of the brain, magnetic resonance imaging of the brain, and a detailed study of cerebral angiography.
An excellent brain aneurysm simulator was developed by Liu et al. with great potential in educational applications, medical evaluation, and surgical planning. The flow of the model was ensured by special techniques [94]. The simulator, which was built using a $600 3D printer, recorded 100% user satisfaction in learning and teaching and 90% in surgical training. The central skull base is an anatomically complex region of the head and neck where neoplasms, vascular diseases, inflammatory diseases, and infections develop. Understanding the structural anatomy of the skull base and performing neurosurgical procedures requires experience, practice, training, and precise orientation to the cranial entry site. The complex anatomy of the nervous system in the region and the proximity of vital and critical structures challenge the skill and stability of neurosurgeons [95]. New technologies enhance surgeons’ skills and student training [96]. 3D printing is widely used in neurosurgical simulation and training and planning procedures [97, 98]. However, 3D technology lags somewhat in applications in epilepsy and detailed sections of certain brain tumors. Moreover, while current 3D models offer high anatomical fidelity, they lack optimal tactile realism, reducing their effectiveness in hands-on simulation [99]. The treatment of spinal disorders requires meticulous preoperative planning and detailed anatomical imaging. 3D spinal models constructed depicting the pathology of each patient offer effective treatment with minimal morbidity and mortality [100]. Izatt et al. demonstrated that 3D spinal models proved useful in 70% of patients in the preparation of preoperative planning and 89% of intraoperative successful implementation [101]. Three-dimensional spinal models also reduce operative times, blood loss, and radiation exposure during fluoroscopy [102, 103].
Gastrointestinal and colorectal surgery
In 1868, Henle first coined the term gastrocolic venous trunk, which is formed by the confluence of the right gastroepiploic vein. Both venous trunks empty into the superior mesenteric vein at the inferior border of the pancreas [104]. In 1912, Descomps discovered that the anterior superior pancreaticoduodenal vein also drains into the same venous system, and thus the gastrocolic venous trunk of Henle consists of three venous trunks: the right gastroepiploic vein, the right superior colic vein, and the anterior superior pancreaticoduodenal vein [105]. More than 10 anatomical variations of the gastrocolic venous trunk of Henle have been described in the literature. To better understand the anatomy and variations of the trunk of Henle, Chen et al. created a 3D printed model of the trunk of Henle that was tested in learning the anatomy of the region. The model proved to be an effective teaching tool, able to help trainees understand the anatomy of the loop of Henle [106]. To facilitate the development of laparoscopic mesenteric resection with vascular ligation in colorectal cancer surgery, Kearns et al. devised preoperative 3D virtual modeling. The researchers reported that the model, created based on mesenteric CT angiography, was acceptable to 90% of surgeons and students in terms of intraoperative utility and ease of learning [107]. In a 2019 systematic review, Kearns et al. concluded that 3D printing of models of patients with rectal cancer, colon cancer, colon cancer with liver metastases, and rectal cancer with planned colostomy contributes to planning the resection of liver metastases, facilitates D3 lymph node dissection, and is useful in understanding pelvic anatomy [108].
Urology applications and personalized surgery
In 1983, Charles Hull first developed stereolithography, a process that uses ultraviolet light to cure and bond photopolymer resins [109]. Since then, the field of 3D printing has experienced rapid and transformative growth. In the last decade, 3D printing and robotic surgery have introduced innovative solutions to diseases of the urinary system. In 2014, Silberstein et al., using specialized software on 3D printers with the stereolithography technique, which uses an ultraviolet laser to cure a photosensitive resin in successive horizontally oriented layers, constructed five physical models of normal renal parenchyma with clear translucent resin and outlined suspicious neoplastic lesions with red translucent resin. The patients underwent successful robotic partial nephrectomy [110]. The researchers found that the models enhanced the perception of the anatomical location of the tumors about the normal renal parenchyma and improved the understanding of the goals of the surgical procedure. Urologist Ghazi at the University of Rochester Medical Center developed a personalized model, a replica of a kidney with five lesions representing the vasculature in a patient with von Hippel-Lindau syndrome (VHL). Von Hippel-Lindau syndrome (VHL) is a rare autosomal dominant disease with a prevalence of 1 : 36,000 births. Clinically, von Hippel-Lindau disease is characterized by retinal hemangiomas (30–60% of patients), clear cell renal cell carcinomas (RCC in 30–50% of patients), cerebellar and spinal cord hemangioblastomas (60–80% of patients), pheochromocytomas (7–20% of patients), and less frequently pancreatic cysts and neuroendocrine tumors. Engen von Hippel first described this type of angioma in the eye. Dr. Arvid Lindau, a Swedish pathologist, described hemangiomas in the cerebellum and spine in detail in 1926. This Ghazi model allowed the patient to undergo well-planned and complex robotic surgery with successful resection, negative surgical margins, and ischemia time of less than 23 min [111]. Manning et al. advocate the practice of practicing/training on 3D printed models that simulate the anatomy and pathology of each patient before surgery, even by experienced urologists, and justify this method by saying “Practice before you play” [112]. Porpiglia et al. tested the impact of 3D virtual printing on surgical performance before robotic-assisted prostatectomy in prostate cancer procedures with positive acceptance [113]. Over the past five years, the application of 3D modeling in urology has emerged as an exciting and effective tool in improving the training of junior surgeons, with value in training them in basic techniques in a safe environment. 3D modeling in urology offers excellent preoperative planning services, particularly effective in robotic-assisted partial nephrectomy and radical prostatectomy, refining the anatomical approach and reducing the time of the procedures and the duration of anesthesia for the patients. It also improves the understanding of the anatomy and pathology of the urinary system for students and nurses [114, 115]. Percutaneous nephrolithotripsy (PCNL) is an effective and safe method for treating nephrolithiasis for stones larger than 2 cm in diameter [116]. Anatomical localization of the stone and knowledge of the precise anatomy of the renal pelvis are prerequisites for successful lithotripsy. The technology of 3D anatomical simulators facilitates the procedure. Atalay et al. used hard, impact-resistant but inexpensive material, acrylonitrile butadiene styrene, in a printer that uses a polymer filament heated in the head and deposited in predetermined positions corresponding to the shaped model. The consumables cost only 100 Euros, and the printing took 2 h. The authors found a 60% understanding of renal anatomy and a 64% understanding of surgical complications. Overall satisfaction with the outcome exceeded 50% [117]. Shin et al. constructed 3D semi-transparent educational models of the prostate to achieve nerve-sparing robotic radical prostatectomy, ultimately with satisfactory results and histological examination with negative surgical margins [118]. Mathews et al. in a 2020 systematic meta-analysis concludes that personalized 3D printed models in lithotripsy, partial nephrectomy, and radical prostatectomy improve patient understanding, reduce procedure time, accurately reproduce complex anatomical pathologies “and provide educational value by simulating surgical procedures”, and promise a decisive contribution to the production of autologous urethral and kidney grafts with mechanical and anatomical properties similar to “normal” tissues [119].
Pandemic-era emergency solutions
3D printing was also useful in the recent pandemic, which tested the resilience and adequacy of all health systems in developed and developing countries. The COVID-19 pandemic in March 2020 was caused by the pathogenic coronavirus that causes fibrosis of the respiratory system and shortness of breath. In severe cases of COVID-19 infection, patients suffer from acute respiratory distress syndrome (ARDS), septic shock, acidosis, and coagulation disorders and require mechanical ventilation. Intensive care units equipped with ventilators are needed during the pandemic. Therefore, the need arises to use one ventilator for more patients by adapting a specially designed separator manufactured with 3D printing technology to the machine’s airway. The 3D printed two-port separator that is adapted to a ventilator, under certain conditions, can be used to ventilate two patients in the Intensive Care Unit [120].
Pharmaceutical and drug delivery applications
Hypertension significantly affects public health. It is estimated that almost 1 billion people in the world have hypertension. We define hypertension as systolic blood pressure values above 140 mm Hg or diastolic blood pressure above 90 mm Hg. A hypertensive crisis is characterized by a systolic blood pressure of > 180 mm Hg or a diastolic blood pressure of > 120 mm Hg. An important drug against a hypertensive crisis is captopril. A therapeutic dose of 12.5–100 mg per os acts within 60 min [121]. 3D printing technology has contributed to the development of rapidly dissolving captopril tablets for personalized use. The study by Hussain et al. confirms the successful manufacture of captopril tablets intended for hypertensive crises that have improved pharmacokinetic properties when combined with hyper-disintegrating/rapid disintegrating agents [122].
Greece is aging. In 2050 it will have fewer than 9 million. Today, 22 out of every 100 inhabitants of Greece are over 65 years old; in 2050, a third will be over 65. Parkinson’s disease is the most common neurodegenerative disease. On average, patients are diagnosed with Parkinson’s disease at the age of about 60 years. Parkinson’s disease requires the administration of many medications. In patients aged < 70 years, the drug of choice is dopamine agonists (pramipexole, ropinirole). In patients > 70 years, levodopa in combination with benserazide is the preferred treatment [123]. Therefore, the treatment of patients with Parkinson’s disease is constantly being adapted and rarely remains as a monotherapy. Windolf et al. developed a 3D printed drug form containing the three substances pramipexole, levodopa, and benserazide in a dosage adapted to the patients’ clinical needs. This approach makes it possible to address the individual needs of patients with Parkinson’s disease by titrating the dose and increasing or decreasing it in small steps, depending on the needs, to respond to ON-OFF phenomena [124]. Yang et al. worked with 3D printing technology to develop famotidine tablets with a more controlled release rate. Indeed, the porous structure of the resulting drug allows rapid disintegration with only a small amount of water, which may help patients with difficulties swallowing tablets [125]. Methotrexate is a potent chemotherapeutic drug and an important therapeutic option for cancer, autoimmune diseases, and osteosarcoma. However, it has poor water solubility, is chemically unstable, and is affected by exposure to light and extreme temperatures. These limitations lead to painful intravenous administration of the drug at high doses, exposing patients to toxicity and associated side effects. Giri et al. considered using 3D technology to produce an orally administered methotrexate formulation that minimizes adverse effects with satisfactory results [126].
Technical aspects and imaging-to-printing process
Personalized three-dimensional (3D) printed anatomical models are considered valuable clinical tools in modern medicine. They visualize anatomical structures and their relationships, facilitate accurate depiction of surgical pathology, contribute to preoperative planning and intraoperative simulation, and result in positive patient outcomes [127]. 3D printed anatomical models are created from computed tomography and magnetic resonance images. The anatomical regions of interest are segmented using Hounsfield units (HU) and converted into file formats suitable for 3D printing (e.g., STL, OBJ, VRML, etc.). STL stands for “stereolithography” and is one of the most common 3D printing file types. OBJ is another common 3D printing file type. Like STL, it contains a 3D model but can also include color and texture information. VRML – Virtual Reality Modeling Language – is a 3D printing file type used primarily in online 3D visualization. It can contain color and texture information, as well as interactive elements [128]. In 2024, Wake et al., combining 3D MRI neurography techniques that provide excellent imaging of nerves and zero echo time MRI (ZTE-MRI) that more accurately visualizes nerves alongside bony anatomy, applied 3D printing to a patient with thoracic outlet syndrome [129]. Thoracic outlet syndrome (TOS) is a condition in which there is compression of nerves, arteries, and/or veins as they exit the neck into the armpit. Three main types have been described: neurogenic, venous, and arterial. The neurogenic type is more common and presents with pain, weakness, and occasionally loss of muscle strength at the base of the thumb. The venous type presents with swelling, pain, and tenderness in the arm. The arterial type results in pain, coldness, and pallor of the arm [130, 131].
Conclusion: clinical and educational impact of 3D printing
3D printing is also playing a critical role in medicine today. It facilitates easier comprehension by physicians of each patient’s anatomy, safer planning of procedures, and more effective implementation of training. Students, surgeons, and patients are all gaining from the real-life models that it creates. Some challenges remain, including cost and access. 3D printing is already proving to be valuable in clinical practice and education. As technology continues to advance, it will play a more prominent role in delivering more specific and focused medical care.