Introduction
Peripheral arterial disease (PAD) is a major contributor to cardiovascular morbidity and mortality, which is often underdiagnosed and undertreated. Its worldwide prevalence is estimated at > 200 million, which is rapidly increasing [1]. It is associated with a huge economic burden that amounts to $ 6.3 billion for hospitalizations annually [2]. The lifestyle-limiting symptoms and limb-threatening conditions of critical and acute limb ischemia often require timely revascularization to improve symptoms, wound healing and/or limb salvage [3].
In recent years, many advances have been made in peripheral vascular interventions (PVI) including drug-coated devices that have gained particular attention. Early trials have favored improved outcomes with drug-coated devices (DRUG) with respect to superior lumen patency in comparison to nondrug devices (NONDRUG) [4–6]. However, a recent meta-analysis has raised a concern of increased mortality with DRUG which led the Food and Drug Administration (FDA) to issue a safety warning regarding their use [7]. In the current setting of these contradictory results from various studies, we utilized real-world data from a national registry to compare outcomes from DRUG versus NONDRUG PVIs.
Material and methods
Data source
The Nationwide Readmissions Data (NRD) is a part of the Healthcare Cost and Utilization Project (HCUP) databases that include the largest collection of de-identified longitudinal hospital care data in the United States, with all-payer and encounter-level information. It has safeguards to protect the privacy of individual patients, physicians, and hospitals. It contains more than a hundred clinical and nonclinical variables for each hospital stay, including a verified patient linkage number for linking hospital visits for the same patient across hospitals, International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS) for principal and secondary procedures and diagnoses (including comorbidities and complications), age, gender, length of stay, and others [8, 9].
Study cohort
The ICD-10-CM/PCS codes were used to search discharged patients in the 2016 NRD who had PVI during the index hospitalization; baseline characteristics and comorbidities, in-hospital postprocedural complications, and endpoints of interest were subsequently extracted. PAD was defined based on ICD-10 codes (Supplementary Table SI) as atherosclerosis of the native peripheral (from common iliac to foot) artery disease or history of vein or prosthetic graft bypass with/without claudication and/or critical limb ischemia (including rest pain, ulcer and/or gangrene). PVI was defined as balloon angioplasty (utilizing a nondrug or drug-coated balloon) with/without stent placement (utilizing a bare metal or drug-eluting stent).
To differentiate postprocedural complications from chronic conditions, the 2016 NRD has a present-on-admission indicator for chronic conditions that present on admission. We also utilized the ICD-10-CM codes used in the Elixhauser comorbidity index to identify comorbid conditions and utilized ICD-10-CM codes that are specific for postprocedural complications to identify endpoints of interest (Supplementary Table SI) [9]. The NRD excludes discharges with missing age, missing or questionable linkage numbers, or from hospitals with more than 50% of their discharges excluded because of these criteria, as patients treated in these hospitals may not be reliably tracked over time [8]. All HCUP recommendations and best practices to use the HCUP datasets highlighted by Khera et al. were followed [10].
Study endpoints
The primary study endpoints included in-hospital all-cause mortality, length of hospital stay, acute kidney injury (AKI), amputation, compartment syndrome, vascular complications, bleeding, and blood transfusion. The 2016 NRD reports in-hospital all-cause deaths and mean length of stay. Other endpoints were assessed during the index hospitalization using specific ICD-10 codes for postprocedural complications (Supplementary Table SI). AKI included new postprocedural kidney failure or acute worsening of chronic kidney disease. Vascular complications included accidental vessel injury, perforation, dissection, and/or retroperitoneal hematoma. Bleeding included any circulatory or central nervous system bleeding during or postprocedural, or postprocedural hemorrhage/anemia. Transfusion included post-procedure blood or blood product transfusion.
Statistical analysis
Statistical Analysis System (SAS) software 9.4 (TS1M4, SAS Institute Inc, Cary, North Carolina) was used for data extraction and statistical analysis which was performed on unweighted (i.e. the actual number) discharges. Pearson’s χ2 test of independence and unpaired-sample t-test were used to compare the endpoints and baseline characteristics between the groups. Propensity matching was performed between DRUG and NONDRUG groups using logistic regression to create the propensity score, based on the basic demographics and baseline characteristics (listed in Table I) for a one-to-one parallel, balanced propensity score matching model using a caliper of 0.001. The Mc-Nemar test was used to compare paired categorical variables of the baseline characteristics and endpoints of interest, while the paired-samples t-test was used to compare continuous variables. A two-tailed p-value of < 0.05 was used for statistical significance [11, 12].
Results
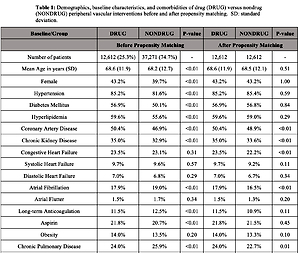
A total of 49,883 discharged patients who underwent lower extremities arterial PVI were identified, 12,612 (25.3%) DRUG and 37,271 (74.7%) NONDRUG PVI; 32.7% had iliac PVIs, 50.7% femoral, 28.5% popliteal, 32.2% infra-popliteal arteries, and 2.3% non-specified site. The mean age was 68.3 years and 40.6% were female. The PVI indication was critical limb ischemia in 33.2%, claudication in 7.6%, and acute limb ischemia in 0.1%. Overall, the DRUG group had a higher percentage of preexisting peripheral arterial disease, diabetes, chronic kidney disease, coronary artery disease, and aspirin use but lower long-term anticoagulation use (Table I).
Table I
Demographics, baseline characteristics, and comorbidities of drug (DRUG) versus nondrug (NONDRUG) peripheral vascular interventions before and after propensity matching
In comparison to the NONDRUG group, the DRUG group was associated with lower in-hospital all-cause mortality (2.2 vs. 2.9%, p < 0.001); shorter hospital stays (8.3 vs. 8.6 days, p = 0.001), bleeding (12.0% vs. 13.5%, p < 0.001), and need for transfusion (10.1% vs. 11.0%, p = 0.004). There was no significant difference in terms of AKI (17.3% vs. 18.0%, p = 0.10), amputation (15.3% vs. 15.4%, p = 0.63), compartment syndrome (0.5% vs. 0.6%, p = 0.07), or vascular complications (0.8% vs. 0.8%, p = 0.50).
In subgroup analysis, the in-hospital all-cause mortality benefit of DRUG PVIs over NONDRUG PVIs was noted in patients with diabetes millets, claudication, critical limb ischemia, acute limb ischemia, and suprapopliteal PVIs but not in infrapopliteal PVIs. After propensity matching, the mortality benefit was no longer present in the matched groups (Table I).
Discussion
Our analysis revealed shorter hospital stay and lower in-hospital, bleeding and all-cause mortality in patients managed with DRUG PVI as compared to NONDRUG PVI; this mortality benefit was seen in subgroups of patients with diabetes, claudication, critical limb ischemia, acute limb ischemia, and suprapopliteal PVIs but not in infrapopliteal PVIs. However, the mortality benefit was no longer present after propensity matching. Our results are in contrast with the meta-analysis by Katsanos et al., which revealed increased mortality with drug-coated devices (specifically devices eluting paclitaxel, which is the only drug coating available in the United States) when used for femoropopliteal interventions [7].
According to their analysis, the mortality increased over time after the first post-procedure year, though the cause of the increased mortality is unclear. Paclitaxel is a chemotherapeutic agent that inhibits the cell cycle, thus preventing neointimal proliferation [13]. It was used in the coronary drug-eluting stents and was not consistently shown to increase mortality up to 5 years of follow-up [14]. Furthermore, it has been shown to improve prognosis in cancer patients who received large dosages of the drug (up to 200 mg/m2) which questions the association between locally released small doses of paclitaxel from DRUG PVIs (up to 8.5 mg) and increased mortality [15, 16]. Moreover, paclitaxel is a short-acting medication with a half-life of 6 h (when used for cancer treatment) and a few weeks to a few months (when used in drug-coated devices) [17], and the mortality signal observed in the meta-analysis was late mortality over years.
This signal of increased mortality cannot be clearly deemed to be device-related, as most individual studies have failed to show a direct causal relation between paclitaxel and death. Furthermore, it is unknown whether this mortality signal is simply because of selection bias because DRUG PVIs were utilized in patients with more advanced disease. The intention-to-treat analysis, which was used to assess the procedural benefit, can give confounding results as crossover or non-compliant patients are often considered in the statistical analysis [18].
Since then, a body of evidence has been accumulating that paclitaxel-coated device-based endovascular interventions do not increase mortality. In the SWEDEPAD (Swedish Drug-elution Trial in Peripheral Arterial Disease) study, the investigators compared all-cause mortality between no drug and drug-coated devices. There was no increase in all-cause mortality at 1- and 4-year follow-up [19]. Dinh et al., in their updated meta-analysis with a larger patient population and time endpoint of 60 months, found that the paclitaxel-coated device group demonstrated no increase in all-cause mortality [20]. More recently, Kumins et al. found that paclitaxel-coated device interventions in critical limb ischemia patients, in fact, improved overall survival and amputation-free survival in their 4-year follow-up study [21]. Adding to the evidence, the patient-level pooled analysis study of Passeo-18 Lux Paclitaxel drug-coated balloon-based interventions versus conventional percutaneous transluminal angioplasty showed no increase in mortality at one-year follow-up [22]. Most recently, Secemsky et al. in conjunction with the FDA demonstrated the non-inferiority of drug-coated balloons or stents to nondrug-coated devices in lower extremity revascularization via a retrospective cohort study on a large patient population of Medicare beneficiaries [23].
The current study, which is based on a large national registry, represents real-world results with a large sample size. It reflects data derived from actual clinical practice in the United States. Furthermore, the reported in-hospital all-cause mortality rate in the current study is comparable to the rates reported in major trials. We believe it adds to and validates the growing evidence of data in favor of the safety of the DRUG PVIs.
This is a retrospective study based on administrative data. Heterogeneity between the two groups is still a concern even after propensity matching. The medical therapy utilized, the lesion anatomy, complexity, severity, length, degree of calcification, types of devices used (such as types, length, drug dose released by the devices, etc.), and other procedural details were not captured by the registry. The drug dose-effect relationship could not be determined. The long-term outcomes were not captured.
In conclusion, this study showed that DRUG PVIs were not associated with higher in-hospital all-cause mortality in comparison to NONDRUG PVIs, which questioned the results of the previously published meta-analysis that showed increased mortality and further supports the newer studies that support the safety of the DRUG PVIs. Further high-quality randomized clinical trials are needed to cover the limitations and the gap in the current literature.