Introduction
Ischaemic heart disease (IHD), affecting approximately 200 million people globally, remains one of the most prevalent cardiovascular conditions and a leading cause of morbidity and mortality [1, 2]. In the United States alone, more than 600,000 percutaneous coronary intervention (PCI) procedures are performed annually for IHD [3]. PCI with drug-eluting stent (DES) implantation significantly reduces the risk of restenosis but carries a risk of stent thrombosis. To prevent ST, current guidelines recommend 6 to 12 months of dual antiplatelet therapy (DAPT) with a P2Y12 inhibitor and aspirin, following PCI with DES [4, 5]. Upon completion of DAPT, indefinite single antiplatelet therapy (SAPT), generally aspirin, is recommended for secondary prevention [4, 6].
While aspirin has traditionally been the standard agent for SAPT, many studies suggest that P2Y12 inhibitors may provide superior protection against recurrent ischaemic events in the post-DAPT setting, without increasing the risk of major bleeding [7–10]. The HOST-EXAM Extended study, with over 5 years of follow-up, demonstrated that clopidogrel monotherapy after PCI with DES was associated with lower rates of the composite net clinical events, including all-cause death, nonfatal myocardial infarction (MI), stroke, and major bleeding [11]. Most recently, the SMART-CHOICE 3, a large randomized trial, showed that clopidogrel significantly reduced the risk of major adverse cardiac and cerebrovascular events compared to aspirin monotherapy in high-risk patients who completed a standard duration of DAPT after PCI [12]. Moreover, this benefit is not limited to clopidogrel alone. A secondary analysis of the GLOBAL-LEADERS trial reported that ticagrelor monotherapy was associated with a lower risk of ischaemic events compared to aspirin monotherapy [13].
A prior meta-analysis by Gao et al. further substantiated these findings, showing that P2Y12 inhibitor monotherapy following DAPT was associated with a lower risk of major adverse cardiovascular events (MACE) compared to aspirin monotherapy [9]. Given the emergence of new data, an updated meta-analysis is essential to consolidate the latest findings and provide the most comprehensive and current evaluation. This systematic review and meta-analysis aims to evaluate the efficacy and safety of P2Y12 inhibitor monotherapy versus aspirin monotherapy following DAPT in the post-PCI population. By synthesising these findings, we aim to provide robust evidence to inform clinical decision-making and guide future treatment guidelines. This is the largest meta-analysis on this subject because we pooled the SMART-CHOICE 3 trial in our analysis, which was not included in prior studies.
Methods
This systematic review and meta-analysis adhered to the guidelines provided by Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [14]. Ethical approval was not required for this study.
Data sources and search strategy
Two researchers (EZ and MA) independently searched PubMed, Google Scholar, and the Cochrane Library, from inception until April 2025. The detailed search strategies are reported in Supplementary Table SI. We also thoroughly reviewed the reference lists of the retrieved articles, past review articles, and previous meta-analyses, to identify any relevant studies that may have been missed in the initial search.
Study selection and eligibility criteria
All articles retrieved from the electronic search were imported into Rayyan software (https://www.rayyan.ai), where duplicates were sought and removed. The remaining studies were independently reviewed by two investigators (NK and PS) based on titles and abstracts, followed by a review of the full texts of the articles. A third author (EZ) was consulted in the event of any disagreements.
Studies were deemed eligible for inclusion in our meta-analysis if they met the following criteria: (1) enrolled patients who had completed dual antiplatelet therapy following PCI; (2) compared monotherapy with either a P2Y12 inhibitor or aspirin; and (3) reported at least one of the following outcomes: major adverse cardiovascular events (MACE), all-cause mortality, cardiac death, MI, major bleeding, stent thrombosis, repeat revascularisation, or any stroke. Exclusion criteria were as follows: (1) studies comparing DAPT directly with SAPT; (2) investigations involving antithrombotic agents other than aspirin or P2Y12 inhibitors; and (3) abstracts, narrative reviews, or pharmacological overviews.
Data extraction, outcomes, and quality assessment
Two investigators (TK and UT) autonomously extracted data from the selected studies, including patient demographics, procedural characteristics, and outcome information. Demographic data encompassed sample size, patient age, sex, and history of smoking, dyslipidaemia, hypertension, and prior cardiovascular or cerebrovascular events. Procedural characteristics included angiographic disease extent, maximum stent diameter, total stent length, and the number of treated lesions per stent.
The primary outcome was MACE. The secondary outcomes included all-cause death, cardiac death, major bleeding, myocardial infarction (MI), repeat revascularisation, stent thrombosis, and any stroke. The criteria used for reporting MACE in each study are mentioned in Supplementary Table SII.
To assess the quality of the included studies, randomized controlled trials were assessed using the Cochrane Risk of Bias tool (RoB 2.0), which assesses bias across five domains [15]. Studies were rated as having low risk, some concerns, or high risk of bias in each domain. For non-randomized studies, the Cochrane Risk of Bias in Nonrandomized Studies – of Interventions (ROBINS-I) tool was used, which evaluates bias across seven domains [16]. Studies were classified as having low, moderate, serious, or critical risk of bias. Two reviewers independently performed the assessments. Visual summaries were generated using the Robvis tool [17].
Statistical analysis
Statistical analysis was performed using RevMan, Version 5.4 (Nordic Cochrane Centre, Copenhagen, Denmark). Odds ratios (ORs) were pooled along with their corresponding 95% CIs for each clinical outcome. The DerSimonian–Laird random effects model was used to account for inter-study heterogeneity [18]. Forest plots were created to visualise the results. Heterogeneity across studies was evaluated using Higgins I2, and a value of I2 = 25–50% was considered mild, 50–75% as moderate, and I2 > 75% as severe [19]. Leave-one-out sensitivity analysis was conducted to identify the influential studies affecting heterogeneity. The total number of included studies was less than 10; hence, the publication bias could not be assessed using funnel plots. A p-value of < 0.05 was considered statistically significant in all cases except for subgroup analysis, where a p-value of < 0.1 was considered significant.
Results
Study selection
A total of 1776 records were identified from various databases. After removing 451 duplicates, 1325 unique records were subjected to title and abstract screening. This process identified 1207 articles that were excluded, and full texts of 118 articles were retrieved for screening. The review of full texts determined 7 reports that met our inclusion criteria [11–13, 20–23]. The PRISMA flowchart Supplementary Figure S1 summarises the screening and study selection process.
Study and patient characteristics
Among the seven studies analysed, three were randomised controlled trials (RCTs) [11–13] and four were observational in design [20–23]. The pooled analysis included 29,756 patients, with 13,523 receiving P2Y12 inhibitor monotherapy and 16,233 receiving aspirin. With the exception of the GLOBAL-LEADERS trial [13, 24], which assessed ticagrelor monotherapy, all other studies focused on clopidogrel monotherapy following DAPT in the post-PCI population. The mean age of patients was 65.1 ±10.4 years in the P2Y12 inhibitors group and 64.7 ±10.6 years in the aspirin group. Detailed baseline characteristics are provided in Table I.
Table I
Baseline characteristics of the included studies
Results of quality assessment
Risk of bias assessment using the RoB 2.0 tool indicated a low risk in two RCTs, while one trial raised some concerns. Among the observational studies evaluated with the ROBINS-I tool, three were found to have a moderate risk of bias and one was assessed as low risk. The details of bias assessment are provided in Supplementary Figures S2 and S3.
Clinical outcomes
Major adverse cardiovascular events (MACE)
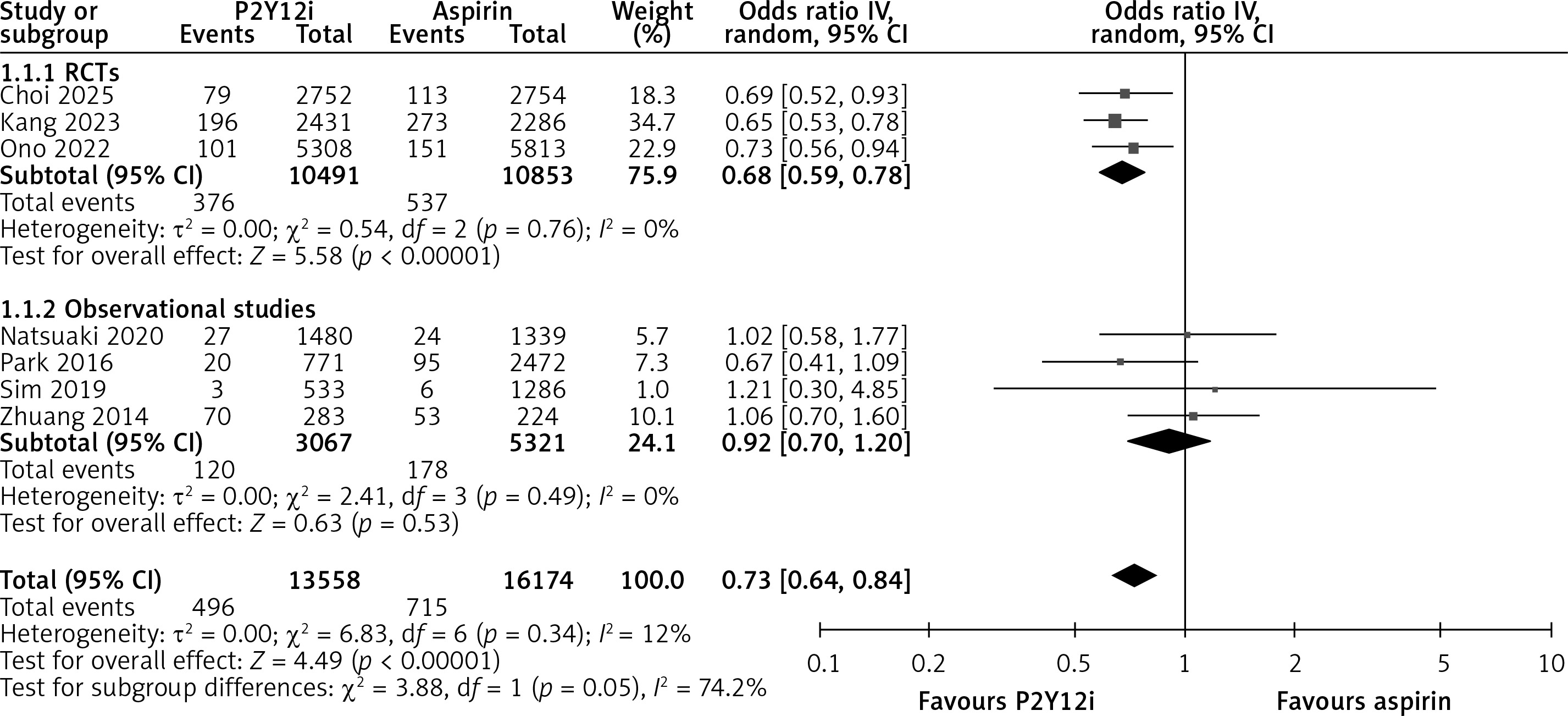
The primary outcome of MACE was reported in all studies. Treatment with P2Y12 inhibitors was associated with a significantly lower risk of MACE compared to aspirin (OR = 0.73, 95% CI: 0.64–0.84, I² = 12%, p < 0.0001, seven studies, Figure 1). Subgroup analysis based on study design revealed that this effect was primarily observed in RCTs (OR = 0.68, 95% CI: 0.59–0.78, I² = 0%, p < 0.00001, three studies), while no significant difference was noted among observational studies (OR = 0.92, 95% CI: 0.70–1.20, I² = 0%, p = 0.53, four studies). The difference between the two subgroups was not statistically significant (p = 0.05). Subgroup analysis by the type of P2Y12 inhibitor showed a comparable reduction in MACE with both clopidogrel (OR = 0.75, 95% CI: 0.62 to 0.90, I² = 27%, p = 0.002, six studies) and ticagrelor (OR = 0.73, 95% CI: 0.56 to 0.94, p = 0.01, one study). There was no significant difference between the two P2Y12 inhibitor subgroups (p = 0.85, Supplementary Figure S4).
All-cause death
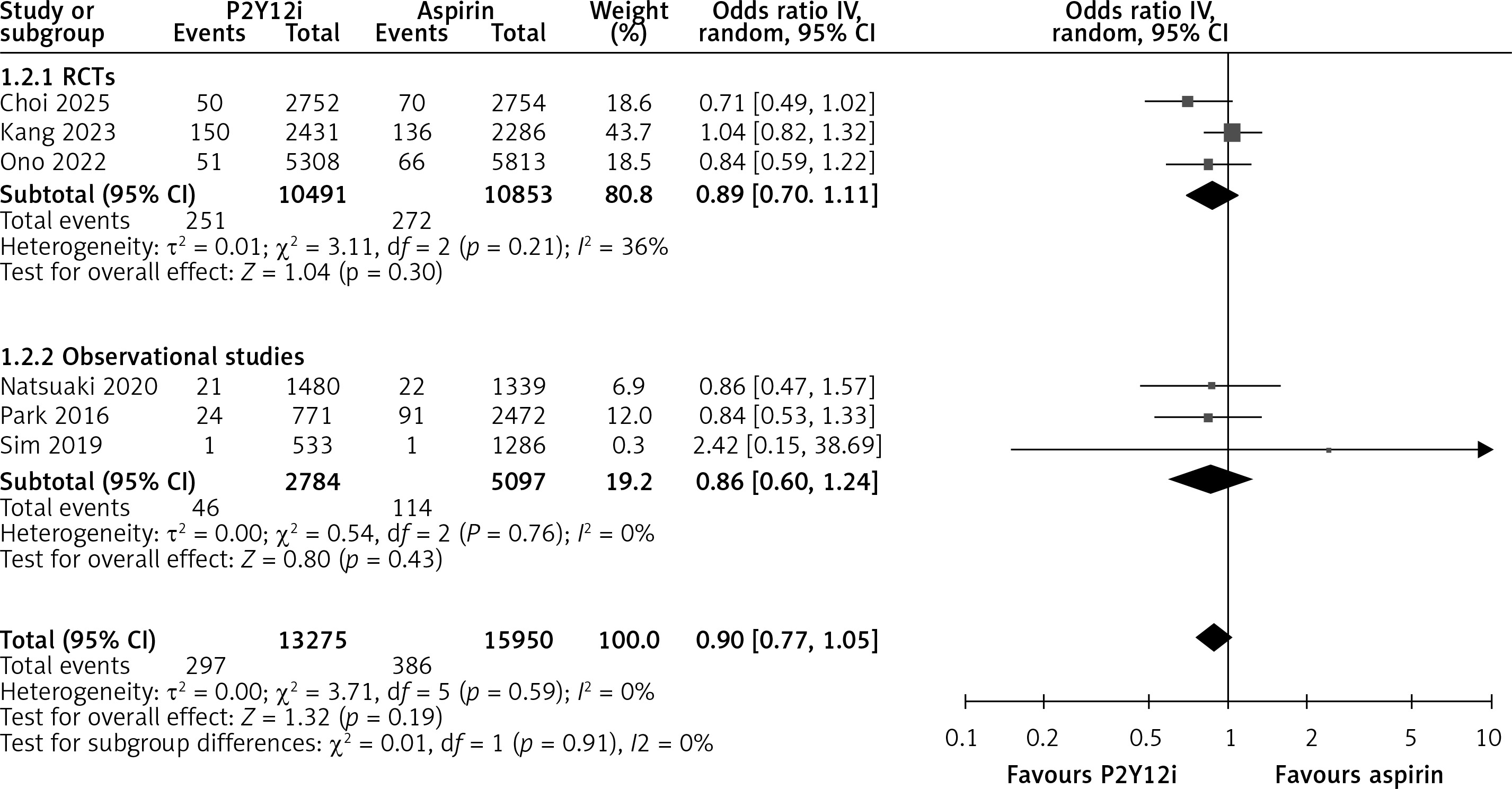
No significant association was observed between P2Y12 inhibitors and aspirin in reducing all-cause mortality (OR = 0.90, 95% CI: 0.77–1.05, I² = 0%, p = 0.19; six studies, Figure 2). Subgroup analysis based on study design showed no significant difference in either RCTs (OR = 0.89, 95% CI: 0.70–1.11, I² = 36%, p = 0.30; three studies) or observational studies (OR = 0.86, 95% CI: 0.60–1.24, I² = 0%, p = 0.43; three studies). No significant difference was detected between the subgroups (p = 0.91). Subgroup analysis by the type of P2Y12 inhibitor showed no significant difference in all-cause mortality with clopidogrel (OR = 0.91, 95% CI: 0.77 to 1.09, I² = 0%, p = 0.30; five studies) or ticagrelor (OR = 0.84, 95% CI: 0.59 to 1.22, p = 0.37; one study). No significant difference was observed between the clopidogrel and ticagrelor subgroups (p = 0.71; Supplementary Figure S5).
Cardiac death
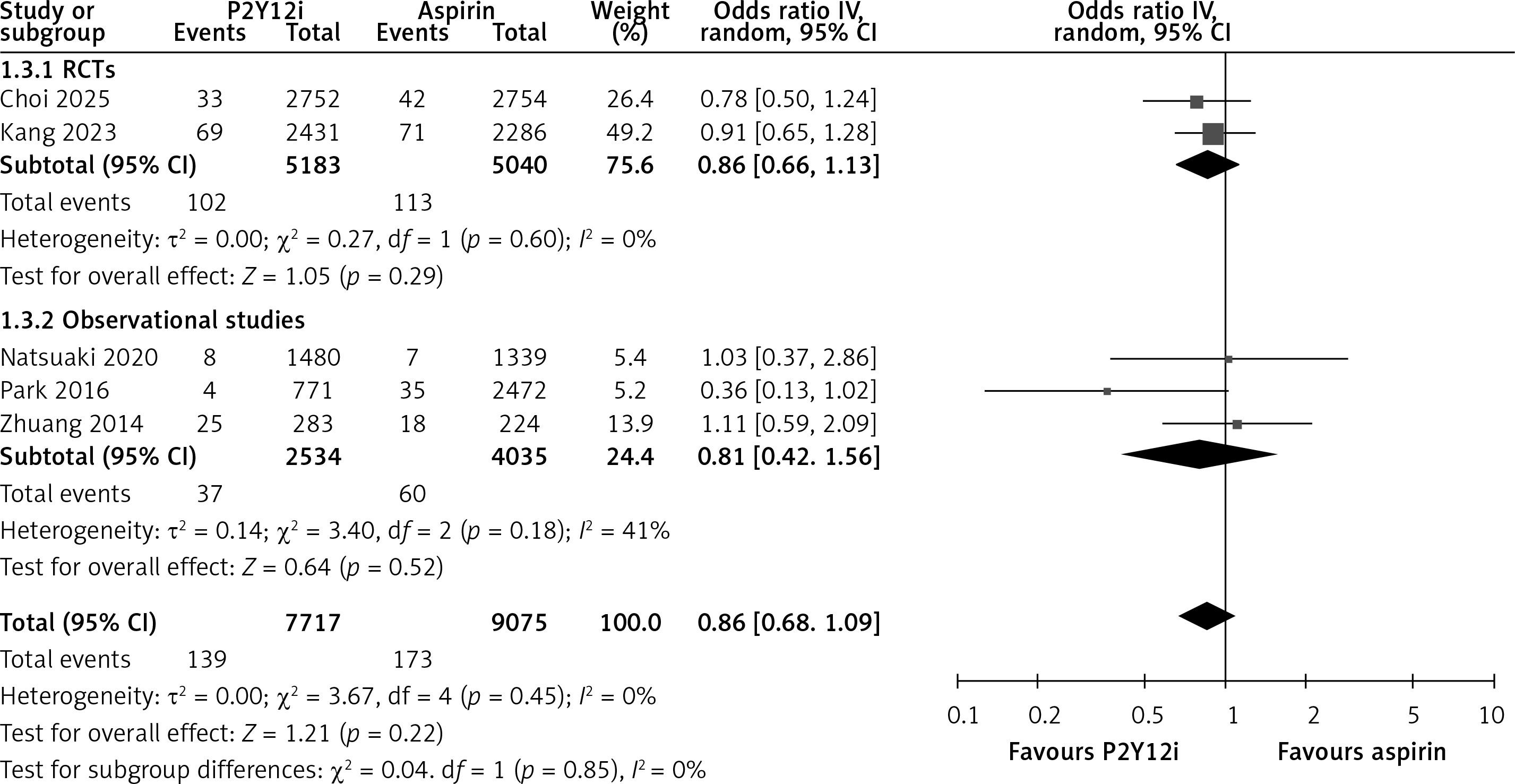
No significant association was observed between P2Y12 inhibitors and aspirin in reducing cardiac death (OR = 0.86, 95% CI: 0.68–1.09, I² = 0%, p = 0.22, five studies, Figure 3). Subgroup analysis based on study design showed consistent findings, with no significant difference observed in RCTs (OR = 0.86, 95% CI: 0.66–1.13, I² = 0%, p = 0.29, two studies) or observational studies (OR = 0.81, 95% CI: 0.42–1.56, I² = 41%, p = 0.52, three studies). No significant subgroup difference was detected (p = 0.85).
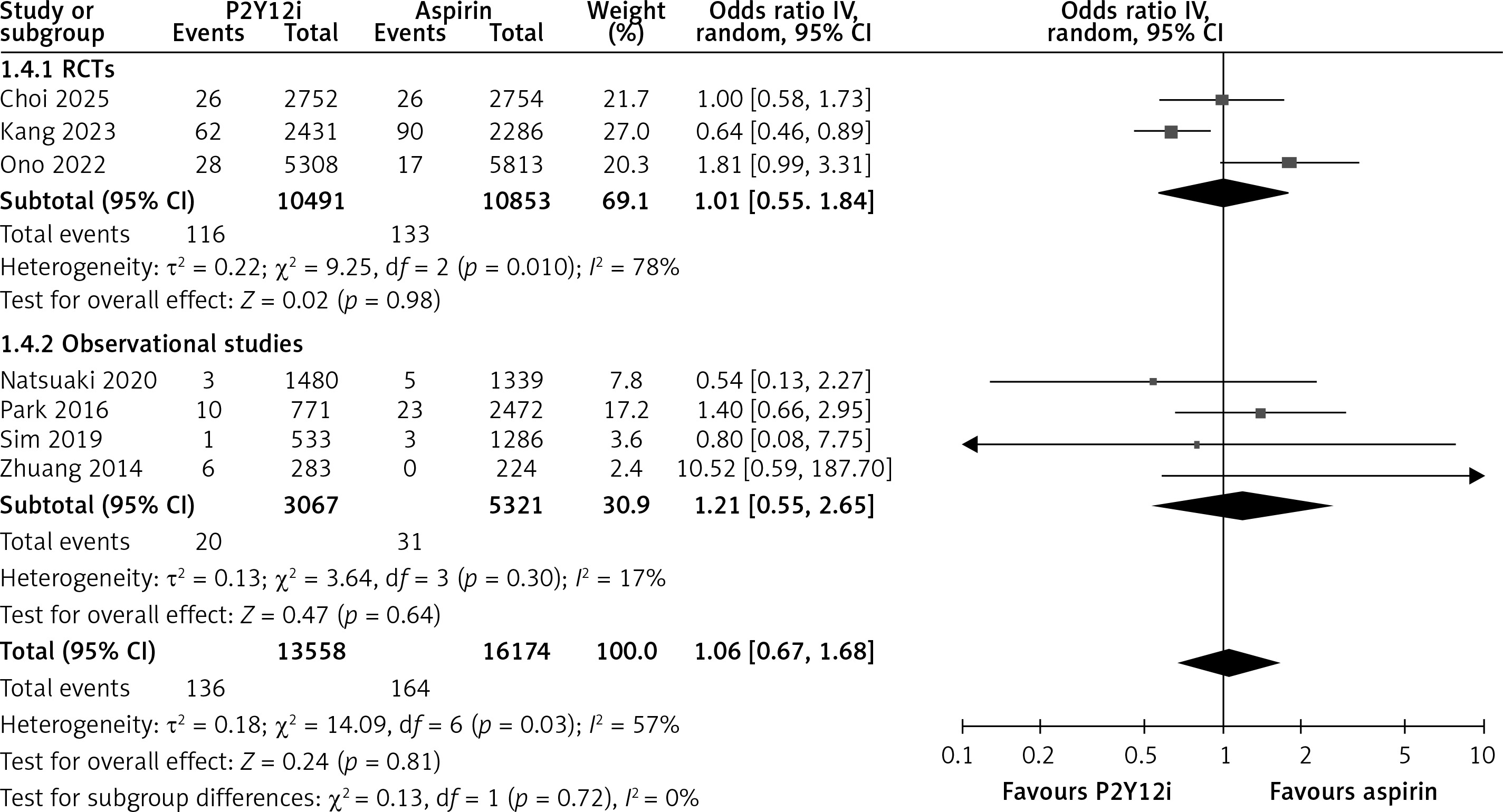
Major bleeding
No significant association was observed between P2Y12 inhibitors and aspirin in the risk of major bleeding (OR = 1.06, 95% CI: 0.67–1.68, I² = 57%, p = 0.81, seven studies, Figure 4). Subgroup analysis based on study design showed no significant difference in either RCTs (OR = 1.01, 95% CI: 0.55–1.84, I² = 78%, p = 0.98, three studies) or observational studies (OR = 1.21, 95% CI: 0.55–2.65, I² = 17%, p = 0.64, four studies). No significant subgroup difference was observed by study design (p = 0.72). Subgroup analysis based on the type of P2Y12 inhibitor showed no significant increase in major bleeding with clopidogrel (OR = 0.89, 95% CI: 0.58–1.36, I² = 37%, p = 0.59, six studies), while ticagrelor showed a borderline statistically significant increase (OR = 1.81, 95% CI: 0.99–3.31, p = 0.05, one study), with no significant difference between the subgroups (p = 0.06, Supplementary Figure S6). Upon performing leave-one-out sensitivity analysis, the heterogeneity was reduced from 57% to 37% on the exclusion of Ono et al. and to 12% after excluding Kang et al. In both analyses, the results remained non-significant (Supplementary Figures S8, S9).
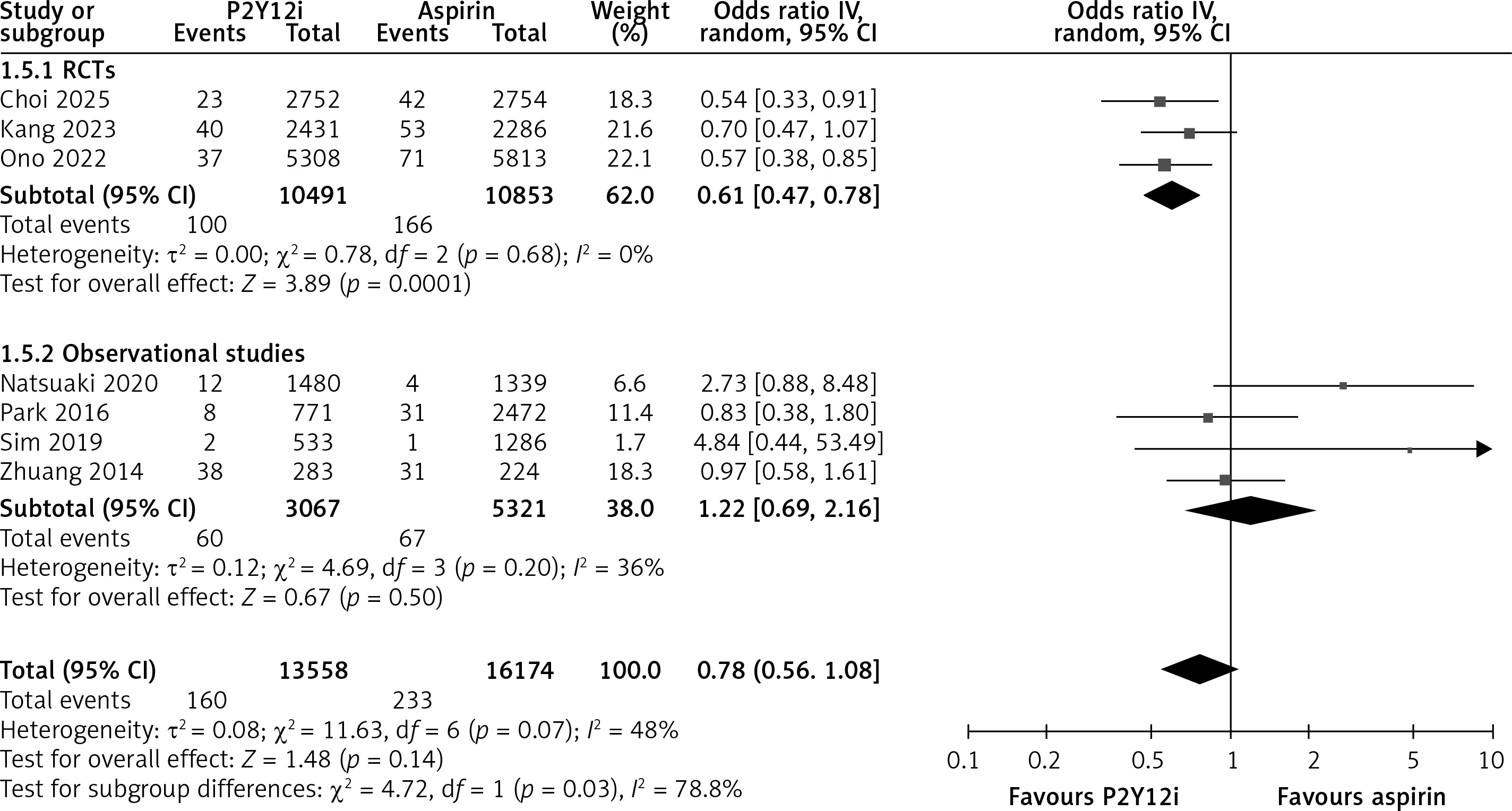
Myocardial infarction (MI)
No significant association was observed between P2Y12 inhibitors and aspirin in reducing the risk of MI (OR = 0.78, 95% CI: 0.56–1.08, I² = 48%, p = 0.14, seven studies, Figure 5). While RCTs showed a significant reduction in MI risk with P2Y12 inhibitors (OR = 0.61, 95% CI: 0.47–0.78, I² = 0%, p < 0.0001, three studies), observational studies did not demonstrate a significant difference (OR = 1.22, 95% CI: 0.69–2.16, I² = 36%, p = 0.50, four studies). A significant subgroup difference was detected based on study design (p = 0.03). Subgroup analysis by P2Y12 inhibitor type showed that clopidogrel was not associated with a significant reduction in MI (OR = 0.87, 95% CI: 0.59–1.28, I² = 49%, p = 0.47, six studies), while ticagrelor demonstrated a significant reduction (OR = 0.57, 95% CI: 0.38–0.85, p = 0.005, one study). However, the difference between P2Y12 inhibitor subgroups was not statistically significant (p = 0.14, Supplementary Figure S7).
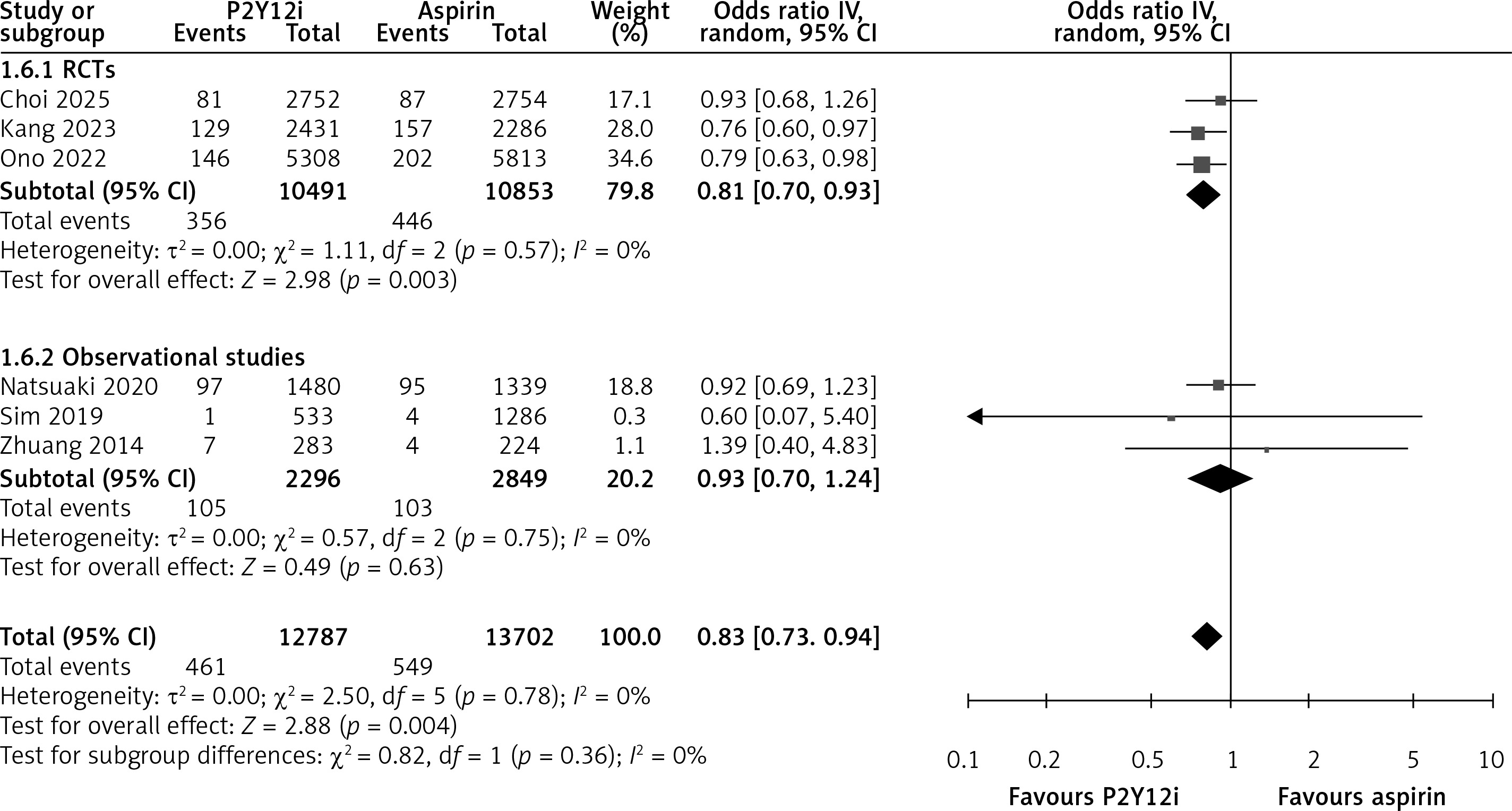
Repeat revascularisation
P2Y12 inhibitor monotherapy was associated with a significantly reduced risk of repeat revascularisation compared with aspirin (OR = 0.83, 95% CI: 0.73–0.94, I² = 0%, p = 0.004, six studies, Figure 6). While RCTs demonstrated a significant reduction in revascularisation risk with P2Y12 inhibitors (OR = 0.81, 95% CI: 0.70–0.93, I² = 0%, p = 0.003, three studies), observational studies did not show a significant difference (OR = 0.93, 95% CI: 0.70–1.24, I² = 0%, p = 0.63, three studies). No significant subgroup difference was detected.
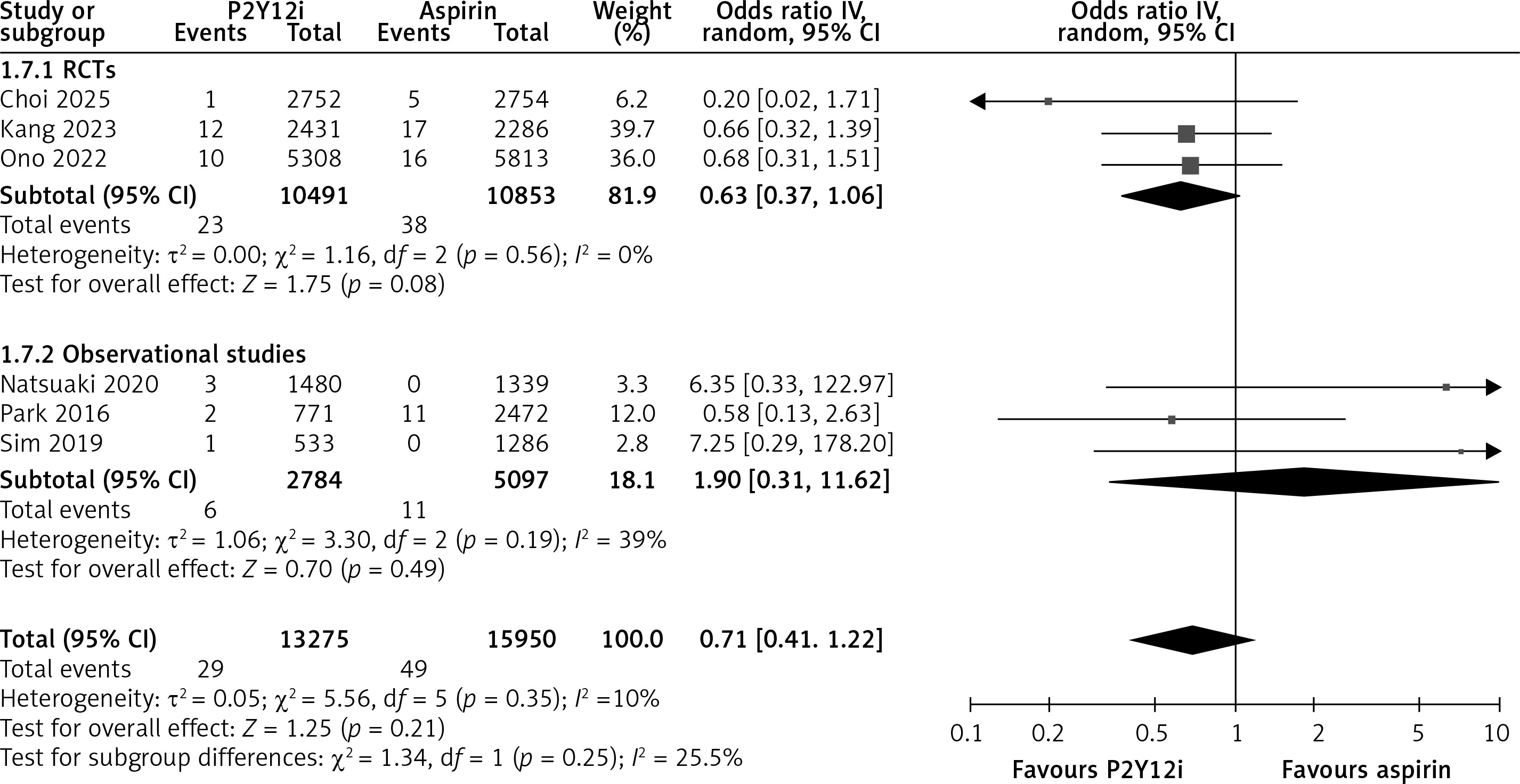
Stent thrombosis
No significant association was observed between P2Y12 inhibitors and aspirin in reducing the risk of stent thrombosis (OR = 0.71, 95% CI: 0.41–1.22, I² = 10%, p = 0.21, six studies, Figure 7). While RCTs showed a non-significant trend toward reduced risk with P2Y12 inhibitors (OR = 0.63, 95% CI: 0.37–1.06, I² = 0%, p = 0.08, three studies), observational studies did not demonstrate a significant difference (OR = 1.90, 95% CI: 0.31–11.62, I² = 39%, p = 0.49, three studies). No significant subgroup difference was detected.
Any stroke
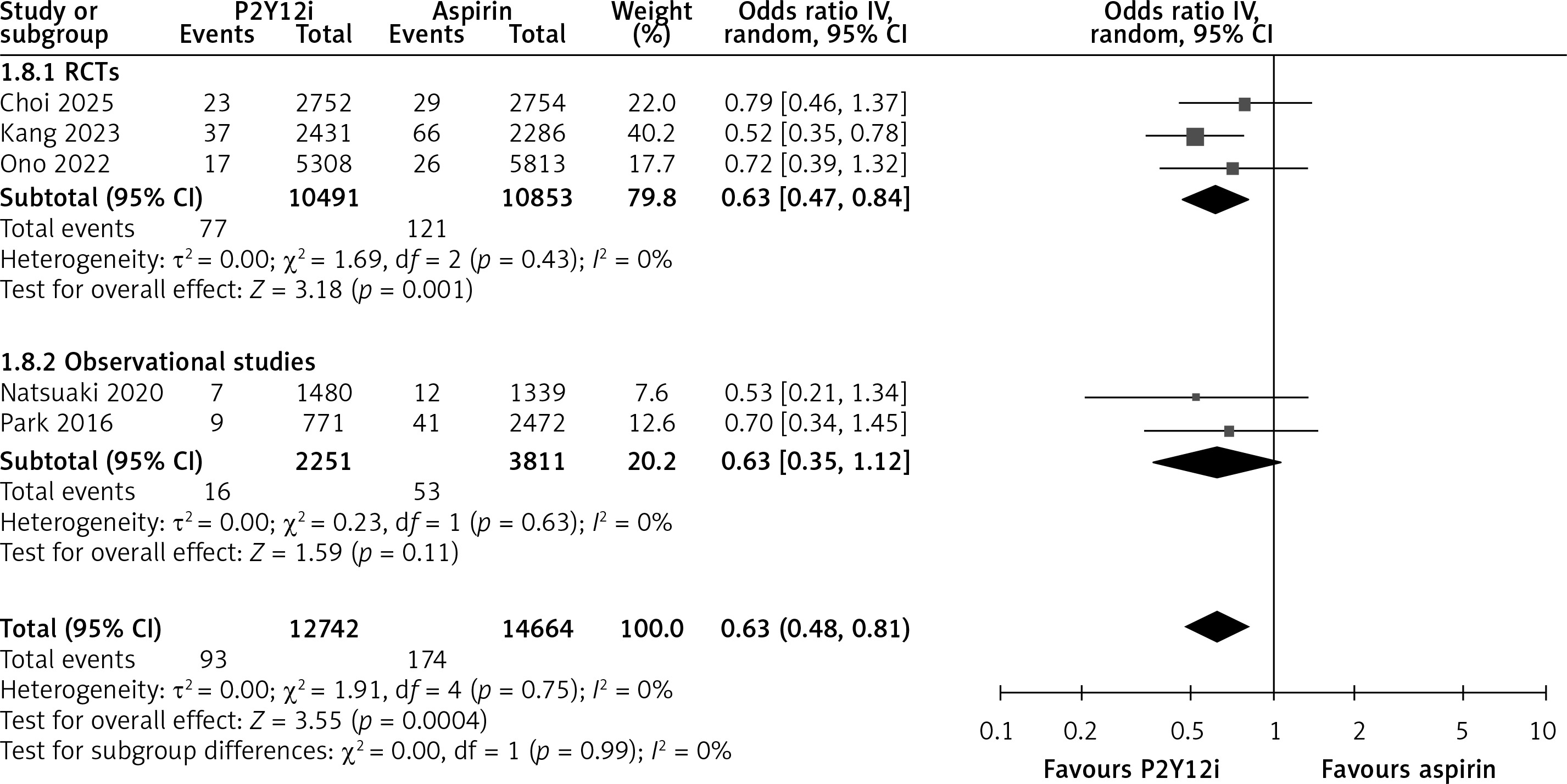
P2Y12 inhibitor monotherapy was associated with a significantly lower risk of any stroke compared with aspirin (OR = 0.63, 95% CI: 0.48–0.81, I² = 0%, p = 0.0004, five studies, Figure 8). This reduction was driven primarily by the RCT subgroup (OR = 0.63, 95% CI: 0.47–0.84, I2 = 0%, p = 0.001), while the effect in observational studies was not statistically significant (OR = 0.63, 95% CI: 0.35–1.12, I2 = 0%, p = 0.11). There was no significant difference between subgroups.
Discussion
In this comprehensive meta-analysis of seven studies, including a total of 29,756 patients, we compared P2Y12 inhibitor monotherapy with aspirin for secondary prevention of cardiovascular events following DAPT in the post-PCI setting. Our findings demonstrated that P2Y12 inhibitor monotherapy was associated with a significantly lower risk of MACE, repeat revascularisation, and any stroke compared to aspirin. There were no significant differences between the two groups in terms of all-cause mortality, cardiac death, major bleeding, MI, or stent thrombosis, although ticagrelor showed a potential benefit in reducing MI risk.
Following PCI, patients remain at risk for thrombotic complications, including MI and stent thrombosis [25–28]. Secondary prevention with antiplatelet therapy is essential to reduce these risks and improve long-term cardiovascular outcomes. While extended DAPT has been shown to lower the incidence of ischaemic events, its use is accompanied by an increased risk of major bleeding [29, 30]. Consequently, there has been increasing interest in shortening DAPT regimens followed by antiplatelet monotherapy to maintain ischaemic protection while minimising bleeding complications [31]. The choice of monotherapy following DAPT completion is an important clinical decision. Traditionally, aspirin has been the preferred agent for long-term secondary prevention, with P2Y12 inhibitors reserved for individuals with aspirin intolerance or contraindications [4, 5, 32]. Although the number of randomised trials directly comparing long-term P2Y12 inhibitor monotherapy with aspirin monotherapy in this setting remains limited, existing evidence suggests that P2Y12 inhibitors may offer superior protection against certain ischaemic outcomes, with a comparable safety profile. These findings emphasise the need to reconsider the conventional strategy of defaulting to aspirin monotherapy after completion of DAPT.
Aspirin inhibits platelet aggregation by blocking thromboxane A2 production via cyclooxygenase-1 (COX-1). P2Y12 inhibitors block the P2Y12 receptor on platelets, preventing ADP-mediated platelet activation, which is a key pathway in arterial thrombosis, especially after stent placement. The P2Y12 pathway is particularly important in the context of PCI, where stent-induced platelet activation is ADP-dependent, making P2Y12 inhibitors more effective at preventing stent thrombosis and recurrent ischaemic events than aspirin alone [33, 34]. Moreover, clopidogrel has demonstrated anti-inflammatory effects by reducing leukocyte activation and inhibiting platelet–leukocyte interactions [35]. These additional properties may contribute to the reduction in MACE observed with clopidogrel monotherapy. The CAPRIE trial [36], in patients with atherosclerotic vascular disease, was the first and the largest trial which demonstrated that clopidogrel monotherapy was more effective than aspirin in reducing the composite risk of vascular death, MI, or ischaemic stroke. However, this trial was not dedicated to a PCI population, as it included patients with a history of recent ischaemic stroke, MI, or symptomatic peripheral artery disease, many of whom had not received prior DAPT or stabilisation. Moreover, the aspirin dose used in CAPRIE (300 mg) far exceeded the currently recommended dose, and the trial was conducted in the early 1990s, before the advent of modern PCI techniques, drug-eluting stents, and contemporary pharmacotherapy. As such, while CAPRIE provides valuable insights, its applicability to current PCI populations is limited.
The findings of this meta-analysis extend the literature considerably. In a previous meta-analysis of five studies, Gao et al. demonstrated that P2Y12 inhibitor monotherapy was associated with a significantly lower risk of MACE compared to aspirin monotherapy [9]. Consistent with our results, this reduction in MACE was primarily driven by decreases in repeat revascularisation and stroke events. Similarly, a more recent meta-analysis also found that P2Y12 inhibitors markedly reduced recurrent MI and haemorrhagic stroke without increasing bleeding risks when compared to aspirin alone [37]. This corroborates our findings that P2Y12 inhibitor monotherapy provides effective prevention; however, it is important to note that their study included a broader population with stable CAD, not necessarily those undergoing PCI. Interestingly, we observed no significant reduction in MI risk. In contrast, the updated network meta-analysis by Andò et al. reported P2Y12 inhibitor monotherapy to be associated with a 39% significantly lower risk of MI [38]. When stratified by study design, RCTs demonstrated a significant reduction in MI events favouring P2Y12 inhibitor monotherapy, suggesting that higher-quality evidence supports a potential cardioprotective effect in this regard. Moreover, when analysed by the type of P2Y12 inhibitor used, ticagrelor monotherapy was associated with a notably lower risk of MI compared to aspirin. This aligns with prior data indicating that ticagrelor, due to its more potent and reversible inhibition of the P2Y12 receptor, may offer superior efficacy in reducing ischaemic events, particularly in higher-risk populations such as those with ACS [39, 40]. In contrast, clopidogrel has shown more variable results across studies, which may reflect differences in genetic responsiveness and pharmacodynamic variability. For instance in East Asian populations, resistance to clopidogrel has been associated with polymorphisms in the CYP2C19 gene, which can impair the conversion of clopidogrel to its active form and reduce its antiplatelet efficacy [41, 42]. Although our meta-analysis did not assess genetic factors, these variations may influence treatment response and warrant further investigation in future studies.
Recent evidence further underscores the relevance and novelty of our analysis. A large individual patient data (IPD) meta-analysis pooled randomised trial data comparing aspirin with P2Y12 inhibitor monotherapy for long-term secondary prevention after coronary revascularisation [43]. Although IPD analyses provide valuable patient-level granularity, their scope was primarily limited to RCTs and did not specifically isolate patients transitioning to monotherapy after completing DAPT in the post-PCI phase, a clinically distinct period characterised by stent-related thrombotic risk not fully captured in chronic secondary-prevention cohorts. In contrast, our meta-analysis focuses exclusively on the post-DAPT PCI setting and integrates both randomized and real-world observational data, reflecting a broader and more pragmatic clinical context. This distinction enhances the applicability of our findings to real-world practice, where treatment decisions after DAPT are influenced by heterogeneous risk profiles and comorbidities that may not be represented in RCT-only analyses.
A very recent meta-analysis by Laudani et al. evaluated short DAPT strategies in ACS patients and compared outcomes based on the monotherapy used afterward [44]. In 23 trials including over 45,000 patients, P2Y12 inhibitor monotherapy after short DAPT significantly reduced net adverse clinical events and bleeding events, while aspirin monotherapy showed neutral effects. However, their analysis primarily assessed DAPT duration strategies, with monotherapy effects influenced by differing lengths of preceding DAPT. In contrast, our meta-analysis focuses specifically on the post-DAPT monotherapy phase, independent of whether DAPT was short or standard, providing a clearer comparison of long-term aspirin vs. P2Y12 inhibitor monotherapy in contemporary PCI practice.
It is also critical to acknowledge the heterogeneity in endpoint definitions and patient populations across the trials included in our analysis. For instance, the definition of MACE differed among studies. The HOST-EXAM trial utilised a broader MACE endpoint, incorporating readmissions due to acute coronary syndrome, which may have influenced the overall event rates compared to trials with narrower definitions [11, 45]. Furthermore, the most recent SMART-CHOICE 3 trial specifically enrolled high-risk patients with a history of recurrent ischaemic events, in contrast to the HOST-EXAM trial, which included patients without restrictions on risk profile or lesion complexity, potentially making the findings from SMART CHOICE 3 more applicable to high-risk subsets [11, 12, 45].
In our meta-analysis, no significant difference was observed in the incidence of major bleeding between P2Y12 inhibitor and aspirin monotherapy, suggesting that P2Y12 inhibitors do not confer an excess bleeding risk in this context. Specifically, clopidogrel appeared to maintain a favourable bleeding profile across studies. In contrast, ticagrelor was associated with a borderline increase in bleeding risk in the limited data available. Ticagrelor exerts a more potent and direct antiplatelet effect than clopidogrel by providing faster, more consistent P2Y12 receptor inhibition [46, 47]. While this pharmacologic strength enhances its efficacy in reducing ischaemic events, it also increases the risk of bleeding. Ticagrelor is consistently linked to a higher risk of major bleeding than clopidogrel, particularly in high bleeding risk (HBR) patients and the elderly [48, 49], making careful patient selection and monitoring essential when using ticagrelor. Importantly, our observations align with findings from prior meta-analyses, which have similarly reported no significant difference in major bleeding between P2Y12 inhibitor and aspirin monotherapy following DAPT [7, 9]. Both monotherapy strategies have demonstrated a reduction in bleeding risk when compared to extended DAPT regimens, supporting the current trend toward shorter DAPT duration followed by SAPT to enhance overall safety without compromising efficacy [31, 50]. Moderate heterogeneity was observed in the analysis of major bleeding. Leave-one-out sensitivity analysis revealed that the HOST-EXAM extended study contributed substantially to this heterogeneity, as its exclusion led to a marked reduction. This may be explained by the study’s inclusion of a relatively low-risk patient population and the longest follow-up duration among included trials, both of which could influence bleeding event rates and accentuate differences in study outcomes. Variability in bleeding definitions, treatment adherence, and event adjudication may also have contributed to the observed heterogeneity.
In addition to efficacy and bleeding risk, practical considerations such as patient adherence and non-bleeding adverse events are important when selecting long-term antiplatelet therapy. Aspirin is generally well-tolerated, inexpensive, and associated with high adherence in routine practice. P2Y12 inhibitors, particularly ticagrelor, may be linked to higher rates of non-bleeding adverse events, including dyspnoea, gastrointestinal discomfort, or minor reversible side effects, which can affect adherence [51]. These factors should be considered alongside clinical efficacy and bleeding risk when individualising post-DAPT therapy, as they may influence both patient experience and real-world effectiveness.
We also observed no significant difference in all-cause death and cardiac death between patients receiving P2Y12 inhibitor monotherapy and those on aspirin monotherapy. This is in line with the findings from previous studies, including the meta-analysis by Al-Abdouh et al. [52], which pooled data from seven RCTs, encompassing 56,982 patients with established atherosclerotic cardiovascular disease (ASCVD). Their analysis revealed no significant difference in all-cause mortality or cardiovascular mortality between long-term P2Y12 inhibitor monotherapy and aspirin monotherapy. Similarly, multiple systematic reviews and meta-analyses consistently report similar findings [7, 9]. These results suggest that while P2Y12 inhibitors may reduce nonfatal ischaemic events, such as MI and stroke, this does not necessarily translate into a reduction in the risk of mortality. This may be explained by the multifactorial nature of mortality in cardiovascular disease, where non-thrombotic factors such as heart failure, arrhythmias, and comorbidities limit the impact of antiplatelet therapy on survival.
From a health-economic perspective, aspirin remains the least costly and most widely accessible antiplatelet agent, supporting its role in long-term secondary prevention. Early models suggested that clopidogrel was not consistently cost-effective relative to aspirin unless prices were substantially lower. More recent analyses, including data from the HOST-EXAM trial, indicate that the economic profile of clopidogrel versus aspirin varies by healthcare system: in some settings, clopidogrel may increase costs slightly, while in others (e.g. the UK and US) it can reduce overall healthcare expenditures without compromising quality-adjusted life years (QALYs) [53]. These findings indicate that while aspirin remains more affordable, generic clopidogrel may be a financially viable option, depending on the healthcare context.
Our analysis has several limitations. First, it combines data from heterogeneous studies, including both randomised trials and observational studies. While observational studies can introduce selection bias and residual confounding that may affect event rates, we included them intentionally to capture real-world practice and patient populations underrepresented in RCTs, enhancing the generalisability of our findings. Randomised trials in this setting remain limited in number, and restricting the analysis to RCTs alone would have reduced statistical power for several outcomes. Second, definitions of endpoints (especially MACE components) and follow-up durations varied among studies, which could contribute to heterogeneity. Third, most data pertain to clopidogrel; only a single trial (or small cohort) evaluated ticagrelor monotherapy [13], and none addressed prasugrel. Therefore, our conclusions apply primarily to clopidogrel-based regimens. Fourth, although the pooled sample is large, some outcomes (e.g. MI, stent thrombosis) were relatively infrequent, potentially limiting power to detect small differences. The trend toward fewer MIs on P2Y12 therapy, seen in RCTs, did not reach statistical significance overall; larger trials or individual-patient data meta-analyses may be needed to clarify this. Finally, as a study-level meta-analysis, we could not account for patient-level factors (such as concomitant medications, stent type, or compliance) that influence outcomes. Finally, we were unable to perform subgroup analyses based on the indication for PCI (elective vs. emergent/ACS) because most included studies did not report outcomes separately by indication. As a result, differences in risk profiles and treatment response between elective and ACS populations could not be specifically assessed, which may influence the generalisability of our findings. Despite these limitations, the consistency of our findings across multiple endpoints and studies strengthens the inference that P2Y12 monotherapy is at least as effective as aspirin, and in some respects superior, for long-term post-PCI therapy.
In conclusion, this meta-analysis demonstrates that P2Y12 inhibitor monotherapy is a safe and effective alternative to aspirin monotherapy for secondary prevention in patients who have completed a course of dual antiplatelet therapy following PCI. P2Y12 inhibitor monotherapy was associated with a significantly lower risk of MACE, repeat revascularisation, and any stroke compared to aspirin. However, there were no significant differences between the two groups in terms of all-cause mortality, cardiac death, major bleeding, MI, or stent thrombosis. Notably, ticagrelor showed potential benefit in reducing the risk of MI. These results suggest that P2Y12 inhibitor monotherapy may offer superior outcomes for certain cardiovascular events while maintaining comparable safety to aspirin. Future large-scale randomized controlled trials are needed to better assess the long-term clinical outcomes of P2Y12 inhibitor monotherapy in post-PCI patients for secondary prevention of cardiovascular events.