Mechanical complications following myocardial infarction, such as pseudoaneurysms, pose unique challenges in terms of diagnosis and management. Despite advances in medical and interventional treatment over the past decades, the post-myocardial infarction (MI) period is associated with potential complications that can lead to severe morbidity and mortality [1].
Although the incidence of mechanical complications post-MI has been reduced due to improvements in reperfusion strategies, it still presents a substantial risk, particularly in the elderly population [2]. These complications include acute mitral regurgitation due to papillary muscle rupture, ventricular septal defects, and pseudoaneurysms. True aneurysms involve all 3 layers of the heart wall and form as a result of chronic changes post-healed MI, generally presenting a lower risk of rupture, and they are not considered direct complications of the initial AMI event [2]. In contrast, pseudoaneurysms occur when there is a rupture of the free wall rupture of the myocardium, and the bleeding is contained by the pericardium, creating a high-risk potential for sudden rupture [2]. Distinguishing between a true aneurysm and a pseudoaneurysm is critical due to the difference in pathophysiology, risk profile, and associated management strategies.
We report a case of a potential inferior ventricular wall aneurysm, resulting in a sequela of myocardial infarction.
A 71-year-old male presented to the hospital with severe dyspnoea on exertion. Ten days earlier, he experienced an excruciating pain in the middle of the chest while walking his dog. He described the pain as “heavy pressure” and “squeezing”, rating it a 7 out of 10. The pain worsened with continued walking, spreading to his jaw and upper abdomen. The pain was not relieved with rest, and it persisted for a couple of hours. The patient experienced unusual shortness of breath the next day while doing simple tasks, which progressed over the next few days until his admission to our hospital. He also reported recent nausea, poor oral intake, diminished urine output, and lightheadedness for the past 10 days.
The patient confirmed a history of hypertension, alcohol use disorder, and 30-pack-years of smoking. He denied any other significant medical history. He has been taking losartan for the past 2 years.
Upon presentation, his vital signs were stable, with a blood pressure of 126/88 mm Hg, heart rate of 97 bpm, and oxygen saturation of 98% on room air. He was afebrile.
The physical examination revealed that the patient was alert and oriented, without acute distress. A loud 3/6 systolic murmur was audible at the left sternal border radiating to the axilla, and jugular venous distension was apparent, extending up to the angle of the jaw. His lungs were clear, but bilateral pedal oedema was noted. The rest of the physical examination showed no significant findings.
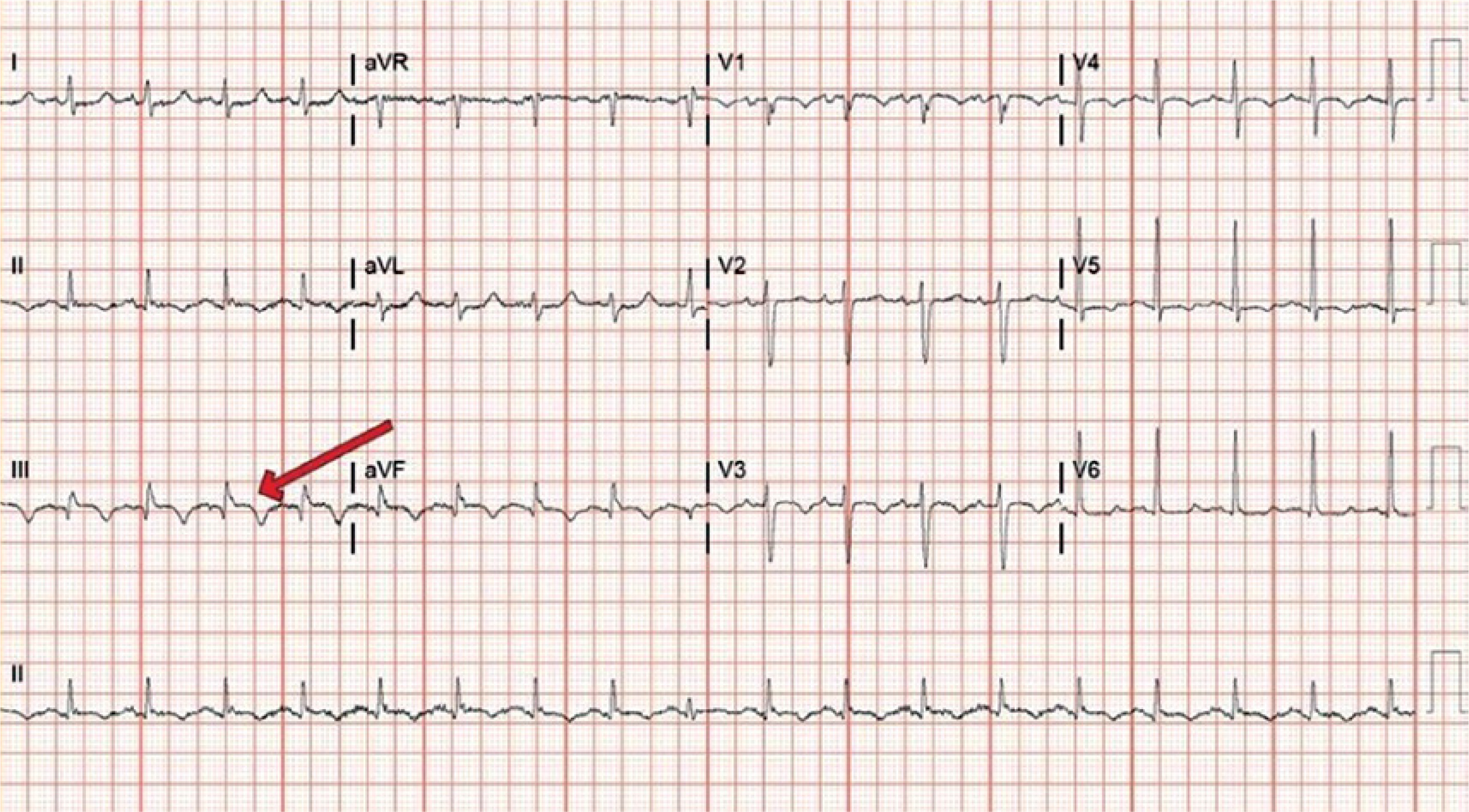
Electrocardiogram indicated sinus tachycardia with persistent ST-segment elevation in leads II, III, and aVF. Chest X-ray identified cardiomegaly, mild pulmonary congestion, small bilateral pleural effusions, and mild left basilar atelectasis. Abdominal ultrasound showed very mild perihepatic ascites but no signs of cholelithiasis or hydronephrosis.
Laboratory findings were within normal limit except an international normalized ratio (INR) of 1.7, sodium of 128 mmol/l, potassium of 5.3 mmol/l, bicarbonate of 16 mmol/l, blood urea nitrogen (BUN) of 35 mg/dl, creatinine of 1.49 mg/dl, bilirubin of 1.9 mg/dl, alanine aminotransferase (ALT) of 866 U/l, asparagine aminotransferase (AST) of 521 U/l, alkaline phosphatase of 115 U/l, lactate of 4.1 mmol/l, BNP of 4270 pg/ml, and initial troponin I of 1.081 µg/ml with a repeat value of 1.020 µg/ml after 3 h. All other screenings were negative.
Upon presentation, an echocardiogram was conducted, revealing a normal-looking left ventricular cavity, but the systolic function was at the lower end of the normal range, with an ejection fraction estimated to be between 50 and 55%. Notably, there was akinesis of the inferior and inferolateral myocardium and dyskinesis of the basal inferoseptal myocardium, consistent with an infarction in the distribution of the right coronary artery. The right ventricle was moderately dilated and demonstrated severely reduced systolic function. Mild dilation was observed in both the left and right atria, as well as mild to moderate tricuspid regurgitation and a trivial pericardial effusion. The estimated pulmonary artery systolic pressure was 36 mm Hg, and the inferior vena cava was dilated, suggesting a right atrial pressure of approximately 15 mm Hg. These findings hinted towards a significant cardiac compromise, necessitating further urgent evaluations and interventions.
A cardiology consultation suggested that the slight elevation in troponins was related to an acute-onset heart failure, and a ventricular aneurysm was highly likely based on the cardiac echo findings showing dyskinesis of the inferoseptal wall and the persistent ST-segment elevation in the inferior leads seen in the ECG findings (Figure 1).
The cardiothoracic surgical team recommended surgical ventricular remodeling; however, given the limitations of the community hospital, procedures to transfer the patient to tertiary care were initiated. The patient remained stable with no chest pain and normal oxygen saturation under room air.
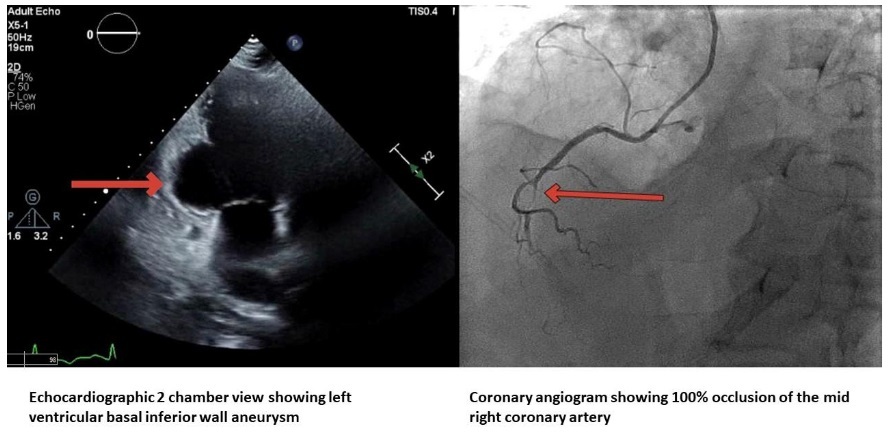
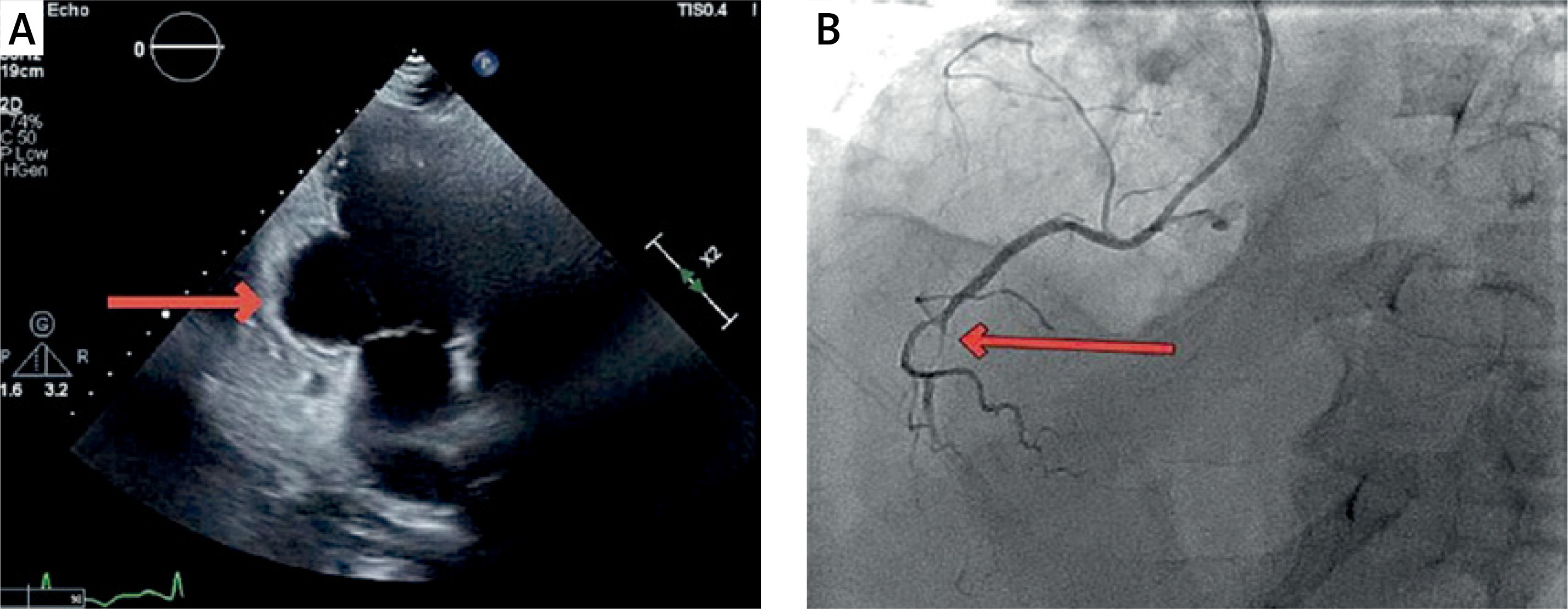
Meanwhile, a Lexiscan test revealed a moderate-sized perfusion defect in the inferior septal wall of the left ventricle, consistent with myocardial infarction and an ejection fraction of approximately 60%. There was no evidence of active myocardial ischaemia. The patient was promptly taken for an angiogram. This procedure revealed a complete occlusion of the mid-right coronary artery (RCA) with right-to-right collaterals and nonobstructive coronary artery disease in the left circumflex artery (LCX) (Figure 2).
Figure 2
A – Echocardiographic 2 chamber view showing left ventricular basal inferior wall aneurysm. B – Coronary angiogram showing 100% occlusion of the mid right coronary artery
Treatment included anticoagulation with heparin, β-blockers, statins, and fluid resuscitation, while Lasix was discontinued. Unexpectedly, the patient collapsed before he could be transferred. Pulseless electrical activity (PEA) indicating a severe cardiac event without effective mechanical heart function was noted. Despite multiple resuscitation attempts, the patient ultimately succumbed to sudden cardiac arrest.
In this case report, we describe a patient with acute myocardial infarction who had a possible aneurysm of the inferior wall that was more suggestive of a true aneurysm, a rare finding in the inferior wall. We, therefore, propose a deeper understanding of pseudoaneurysm and true aneurysm in patients with myocardial infarction.
Pseudoaneurysm: Left ventricular pseudoaneurysms are reported in 0.1% of all patients with myocardial infarction [3]. It may also present secondary to cardiac surgery and trauma [4]. Pseudoaneurysms occur when the ventricular free wall ruptures but is restricted within the surrounding adherent pericardium or scar tissue [3].
While free wall rupture is more common in the anterior wall, pseudoaneurysms are more common in inferior walls due to the dual blood supply to the inferior wall, which limits the extent of damage [5]. Another proposed reason is the higher tendency to form dependent pericardial adhesions in patients who are recovering in a recumbent position following an MI [5].
A cardiac pseudoaneurysm, characterised by its pericardial composition, narrow neck, variable systolic behaviour, and a high rupture risk necessitating more aggressive and emergent intervention due to its instability, is typically diagnosed with echocardiography [6].
True aneurysm: True aneurysms form as a result of chronic changes post-healed myocardial infarction and are not considered direct complications of the initial AMI event [2]. Other rare causes include Chagas disease, cardiac surgery, and hypertrophic cardiomyopathy. True aneurysms are characterized by thinned myocardium that is dyskinetic (bulges outward during systole) and encompass all 3 layers, i.e. the entire thickness of the wall. They have a lower risk of rupture compared to pseudoaneurysms.
Cheng et al. analysed 100 consecutive patients with coronary artery disease, primarily presenting with symptoms such as angina and exacerbations of congestive heart failure, utilising cine ventriculography and coronary arteriography to reveal that 35% of these patients had ventricular aneurysms [7].
The most common pathogenesis of left ventricular aneurysms involves a total thrombotic occlusion of the left anterior descending (LAD) artery [8]. Involvement of the inferior or basal walls secondary to the occlusion of the right coronary artery is much less common [8]. Only 3% of aneurysms are posterior or inferior [9].
The anterior wall is mainly supplied only by the left anterior descending artery, while the inferior wall has a dual blood supply from both the right coronary artery and the circumflex artery, which can mitigate the extent of damage relative to what is typically observed in anterior wall infarctions [2]. Cheng et al. pointed out and deemed that total devascularisation is necessary for the formation of an aneurysm and is thus less likely to involve the inferior wall [7].
A true LV aneurysm is associated with an increased risk of angina pectoris, thrombus formation, worsening heart failure, and haemodynamically significant ventricular tachyarrhythmia [8].
Diagnostic modalities: Distinguishing between a true aneurysm and a pseudoaneurysm is critical due to the distinct pathophysiology, risk profile, and management strategies associated with each.
Contrast ventriculography visualises ventricular chambers with contrast dye, revealing broad or narrow connections. Radionuclide ventriculography uses radiolabelled substances to evaluate cardiac blood flow and function [6].
Transthoracic and transoesophageal echocardiography provide accessible, detailed images of heart structures, identifying myocardial continuity. Doppler echocardiography measures blood flow, detecting turbulent patterns indicative of pseudoaneurysms [5].
Coronary arteriography can assist in differential diagnosis as well. In a true aneurysm, the coronary arteries may lie along the aneurysm’s wall, whereas in a pseudoaneurysm, they do not drape over the paraventricular chamber because the cavity is formed by blood and pericardium disrupting the myocardium [10]. Additionally, coronary angiography can detect coronary artery disease, indicating whether a coronary artery bypass graft (CABG) might be necessary if a procedure is required.
The definitive method for distinguishing the pathological features of an inferior left ventricular aneurysm is direct intraoperative examination, because they can only be reliably identified during surgery [5].
Cardiac MRI: Kumbasar et al. emphasised the role of MRI in differentiating between left ventricular true aneurysms and pseudoaneurysms by visualising myocardial wall structure, utilising delayed gadolinium enhancement to identify scar tissue and assess myocardial viability, and detailing the aneurysmal neck and shape, alongside the localisation and extent of infarction [11].
Zoffoli et al. reported a case where an MRI suggested a pseudoaneurysm, but intraoperative findings revealed a true aneurysm with a thrombus, underscoring the limitations of preoperative diagnostics. The presence of thrombus within the aneurysm cavity can obscure contractility and imaging findings, and mimic the appearance of a pseudoaneurysm [9]. The presence or absence of a mural thrombus in a ventricular aneurysm not only influences haemodynamic characteristics but also requires specific treatments, such as anticoagulation therapy or surgery.
Management of ventricular pseudoaneurysms: In the treatment of post-infarction left ventricular pseudoaneurysms, surgical intervention is generally preferred due to the high risk of rupture.
Sui et al., in their study of 183 patients, found that although not statistically significant, CABG with left ventricular resection was associated with better left ventricular ejection fraction (LVEF) and left ventricular end-diastolic dimension (LVEDD) outcomes compared to percutaneous intervention (PCI) or drug treatment [12].
Employed techniques include primary repair with polytetrafluoroethylene (PTFE) felt-reinforced sutures and closure using either a Gore-Tex patch or an autologous pericardium patch accessed through the left atrium. A double patch technique involving both internal and external Dacron has also been described [13].
Additionally, for high-risk surgical candidates, percutaneous closure presents a viable alternative [14].
Management of LV aneurysms: Asymptomatic LV aneurysms, regardless of size, are monitored with a focus on optimising coronary artery disease risk factors, using medications like angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, and employing anticoagulation to prevent thromboembolism. For symptomatic large LV aneurysms, management includes the same medical strategies plus surgical intervention if indicated [9].
True aneurysms may require medical or surgical therapy, with the surgical risk often being debated and depending on individual patient factors. Indications for surgical intervention in true aneurysms are well-established and include congestive heart failure, angina pectoris secondary to associated coronary artery disease, ventricular tachyarrhythmias, and, less frequently, thromboembolism [5].
The presence of a ventricular aneurysm complicates coronary surgery by involving non-viable scar tissue, posing technical risks like rupture, potentially leading to suboptimal revascularisation if unaddressed, and it may necessitate the sacrifice of coronary branches, thus requiring thorough preoperative assessment to optimise outcomes [7].
When surgery is indicated, it is not only therapeutic but also provides the opportunity for a definitive diagnosis, which can inform postoperative management and long-term care strategies [5].
Issues with the inferior wall: True aneurysms of the inferior wall are rare, as we have previously mentioned. Additionally, Zoffoli et al. noted in their study that the more posterior the aneurysm in the heart, the more difficult it is to detect [9].
The surgical treatment of inferior wall left ventricular aneurysms is notably complex and demanding, primarily due to the higher prevalence of false aneurysms, which increases the risk of rupture and requires a cautious yet aggressive surgical approach. Additionally, these aneurysms are often accompanied by clinical complications such as mitral valve dysfunction and issues related to previous myocardial infarctions, further complicating the surgery. The aneurysms’ location not only hinders surgical access and visibility but also demands exceptional surgical expertise and meticulous planning [5].
Our case had a large inferior wall aneurysm without any mitral regurgitation. The patient collapsed suddenly in the ward while he was being worked up before he could be taken up for a cardiac MRI or surgery. The echocardiogram findings of dyskinetic basal inferoseptal myocardium point towards a true aneurysm. However, given the location on the inferior wall and sudden PEA arrest, a rupture of pseudoaneurysm is also possible. As we have illustrated, the distinction between the two is often difficult, and it requires either extensive imaging studies or direct visualisation intraoperatively.
This emphasises the urgent need for specialised, multidisciplinary management of ventricular aneurysms, especially those found on the posterior and inferior walls.
In conclusion, distinct and rapid diagnosis of true aneurysms and pseudoaneurysms through appropriate techniques and imaging will help improve the short- and long-term prognosis and complications. Thus, it is vital for physicians to appropriately rule out such events in post-myocardial infarction cases.