
Aortic stenosis (AS) is a cardiovascular condition caused by the narrowing of the aortic valve. When characterised as severe, increased transvalvular pressure and reduced blood flow can lead to a clinical picture of angina, syncope, and heart failure [1]. Mild to moderate disease is often asymptomatic. However, for severe AS, the 2014 guidelines from the American College of Cardiology and the American Heart Association emphasise a need for constant monitoring and follow-up to manage and delay the progression of AS [2].
Once AS is severe, an aortic valve replacement (AVR) is indicated. Among the various options for AVR, transcatheter aortic valve replacement (TAVR) has become the favoured approach [3]. More specifically, the 2020 ACC/AHA guidelines state that for older adults or individuals considered high surgical risk, TAVR versus surgical aortic valve replacement (SAVR) has demonstrated improved survival rates, and fewer incidences of acute kidney injury, new atrial fibrillation, and major bleeding [4]. Nevertheless, TAVR can lead to intra- and post-operative complications of vascular insults, myocardial infarction, aortic regurgitation, and valve thrombosis [5].
One complication that can occur following cardiac procedures is post-cardiac injury syndrome (PCIS). PCIS is described as inflammation of the pericardium and surrounding pleura, causing chest pain and fever [6]. It is believed to arise from cardiac injury, with ensuing inflammation creating an environment for self-antigen recognition precipitating an autoimmune response [7]. Even though PCIS is well-researched following procedures such as pacemaker implantation and cardiac surgery, it has been reported very few times after TAVR [8].
In this case, we describe a 70-year-old male who developed chest pain, fever, fatigue, and a large pericardial effusion 9 months after TAVR. A pericardiocentesis with the insertion of a pericardial drain was performed due to suspicion that the clinical presentation was because of PCIS. This case highlights the importance of postoperative follow-up in patients who undergo TAVR. Increased awareness and comprehensive work-up are essential to improving patient outcomes and avoiding complications.
The patient is a 70-year-old male with a history of severe aortic stenosis. He was admitted to the hospital for a coronary angiography as a part of a planned TAVR. The possibility of obstructive coronary artery disease was excluded by coronary angiography. The patient was then given the option of either a surgical aortic valve replacement or transcatheter aortic wall replacement. After explaining the advantages and disadvantages, the patient elected to have a TAVR (Figures 1–3).
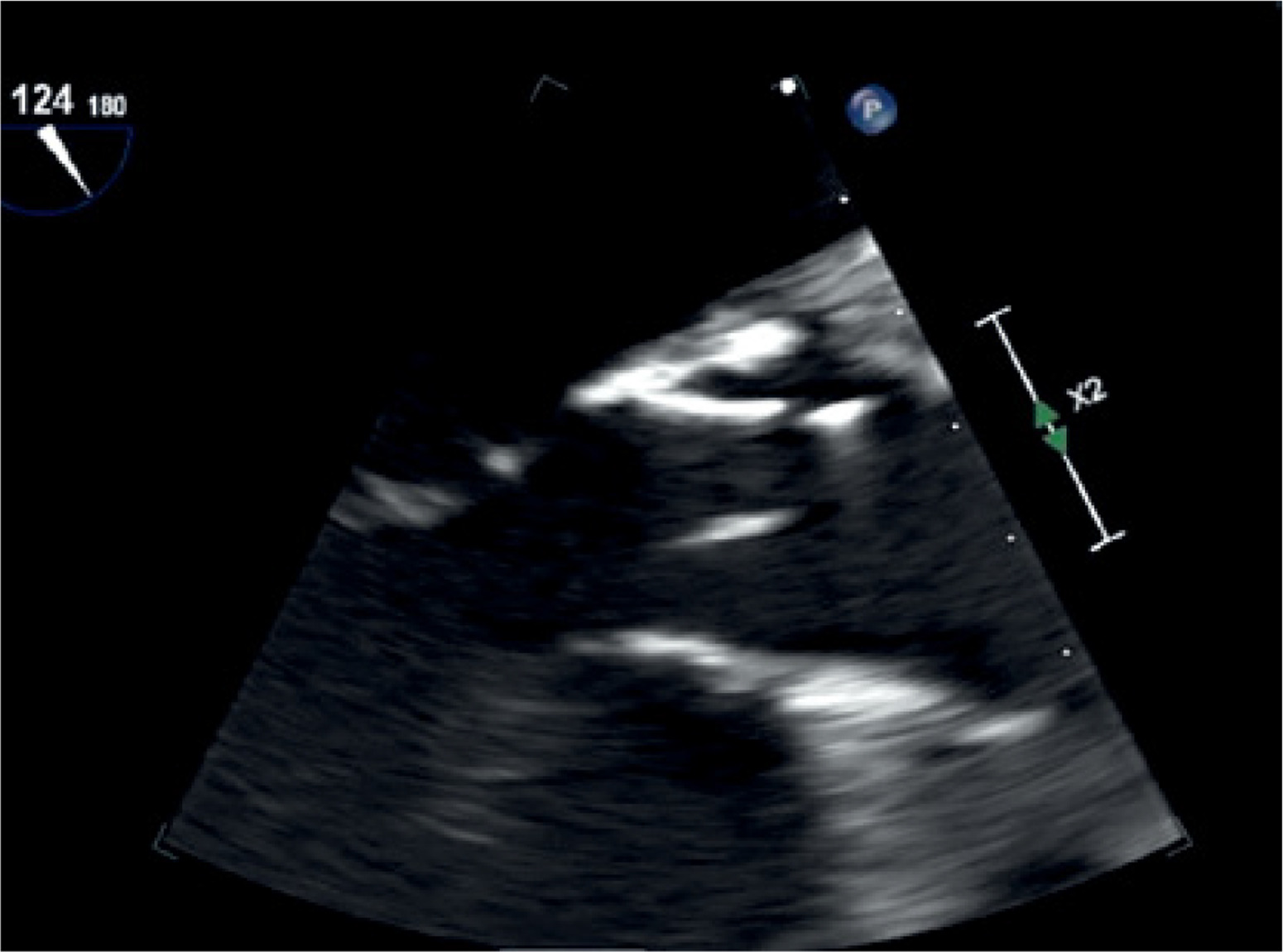
Figure 1
Image taken via transesophageal echocardiogram showing normal position of prosthetic aortic valve

A transcatheter aortic valve insertion using a 23-mm Edwards Sapien 3 Ultra Transcatheter Aortic Valve after balloon valvuloplasty with a Nucleus-X 20 mm × 6 cm valvuloplasty balloon was performed, and the end result was grade 1 paravalvular leak. The patient was later moved to a ward.
He had low haemoglobin levels and a haematoma at the femoral location. A computed tomography (CT) scan was performed, revealing retroperitoneal haemorrhage from the left external iliac artery. As a result, the patient was sent back to the cath lab for a selective left angiography in preparation for percutaneous transluminal intervention of the external iliac artery. A retroperitoneal leak from the left external iliac artery was corrected with the implantation of a 9 mm × 58 mm covered stent, and the patient was transferred to the intensive care unit (ICU).
The patient was discharged from the hospital on aspirin and Plavix while monitoring for haematocrit. The echocardiography after the procedure showed that the valve was securely set in the aortic valve position with the following results: peak velocity 4 m/s, mean gradient 40 mm Hg, valve area 0.93 cm2, and index valve area 0.51.
The patient was followed in the clinic 2 months after discharge for a repeat echocardiogram, which was again normal. Nine months later, the patient came back to the emergency department with complaints of 4/10 pressured chest pain, fatigue, shortness of breath, and rigors. He also reported generalised weakness and decreased appetite.
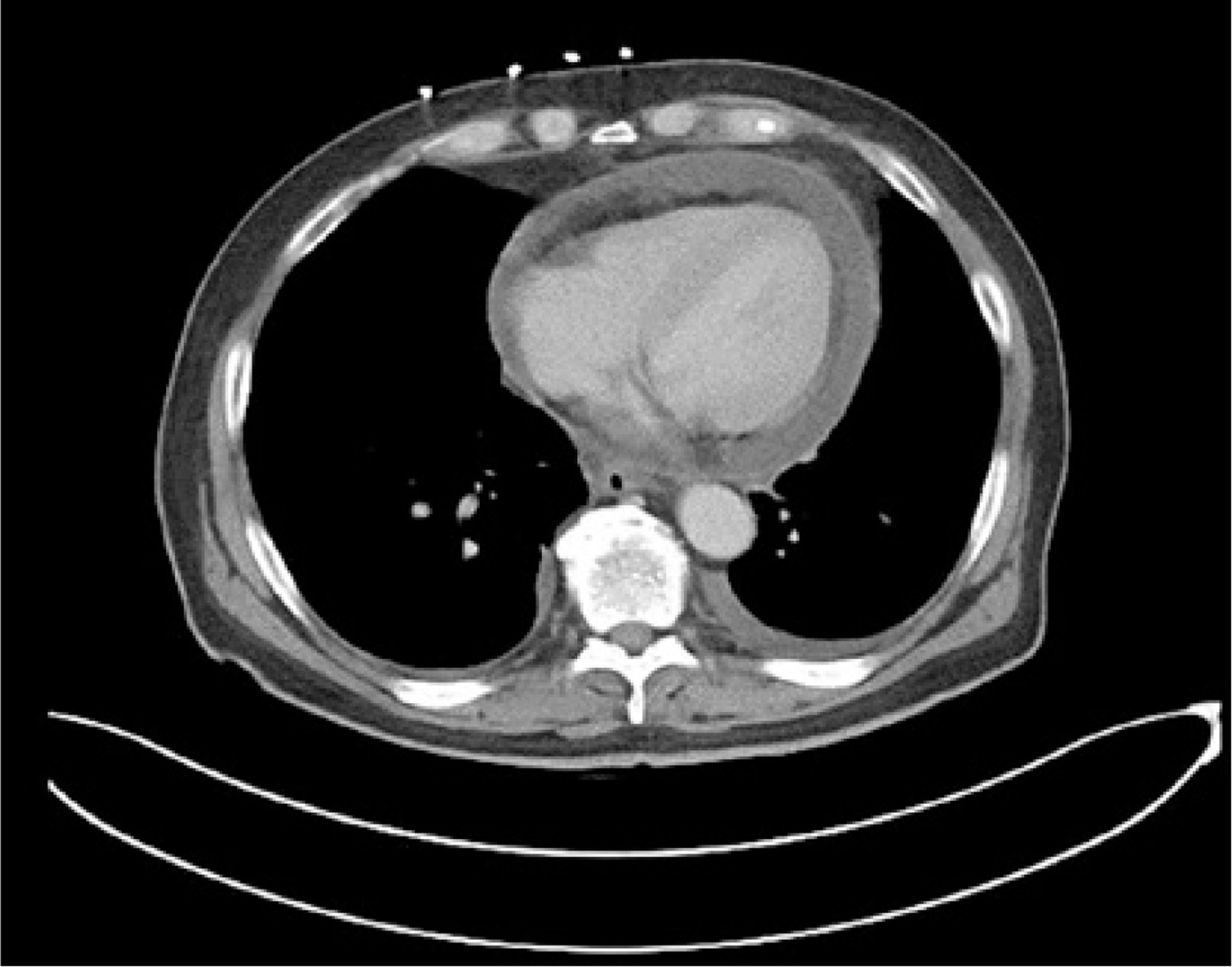
X-ray and ECG results were normal. A complete blood count in the ED showed an elevated white blood cell count of 21,400 per millilitre (count/ml), haemoglobin as 13.3 grams per decilitre (g/dl), and 43% haematocrit. A creatinine level of 2.3 milligrams per decilitre (mg/dl) was seen on renal function test. Liver function tests revealed normal levels of alanine aminotransferase (ALT) at 11 U/l, aspartate aminotransferase (AST) at 18 U/l, and alkaline phosphatase at 53 U/l. The normal values for sodium (Na), potassium (K), and calcium (Ca) were 137 milliequivalents per litre (mEq/l), 4.2 mEq/l, and 10.3 mg/dl, respectively. A chest CT scan was done in the ED, which revealed a massive pericardial effusion as well as a left pleural effusion. On echocardiography, a notable pericardial effusion without tamponade was observed (Figure 1). A thoracentesis was performed in the ward, draining 400 ml of fluid.
Pericardiocentesis was performed, and 250 ml of serosanguinous fluid was drained and sent for culture. The next day, a transoesophageal echo ruled out any vegetation on the prosthetic valve, but it was suggestive of residual fluid. A repeat pericardiocentesis was planned, and this time, a drain was left in the pericardial sac. In the next 24 h, 500 ml was collected through the drain. A repeat ECHO done the next morning, after overnight clamping of the drain, showed no re-accumulation of fluid. A decision was made to withdraw the pericardial drain.
Autoimmune workup with antinuclear antibody and rheumatoid factor was done along with a vasculitis panel and QuantiFERON gold test for tuberculosis. All of them came back within normal limits. Definitive blood cultures and cultures from the pericardial fluid came back negative. The patient was later discharged home on colchicine and aspirin and asked to follow up in the clinic.
The progressive nature of AS and the associated long-term complications have led to various changes in guidelines that encourage serial monitoring and severity stratification for mild/moderate cases, while surgical approaches are recommended for severe AS [1–3]. Patients undergoing such surgical treatment are at risk of complications, including PCIS.
Dressler’s syndrome, which occurs after a myocardial infarction, is a classic example of PCIS. Additionally, this condition can arise following cardiac surgery (known as post-pericardiotomy syndrome) and cardiac trauma (referred to as post-traumatic pericarditis). PCIS has been observed after seemingly minimally invasive procedures like percutaneous coronary angioplasty, radiofrequency catheter ablation, and pacemaker implantation [9].
Among minimally invasive procedures, it has been well-studied in patients undergoing pacemaker implantation. Greene et al. reported a 4.9% incidence of acute symptomatic pericarditis post dual-chamber pacemaker insertion [10]. Similarly, Zeltser et al., in their retrospective study, reported PCIS in 2% of cases out of their total of 443 pacemaker implantation procedures (237 epicardial and 206 transvenous) in 370 patients [11].
Aetiology and pathogenesis: PCIS arises from an immune-mediated response to cardiac injury. Damage to pericardial or pleural mesothelial cells, coupled with the entry of blood into the pericardial space, initiates this syndrome. This is further exacerbated by a systemic release of cardiac antigens and a non-specific activation of the immune system, leading to an adaptive immune response.
Elevated anti-myocardial antibody titres have been correlated with the incidence of PCIS following cardiac surgery, highlighting the autoimmune nature of this syndrome [7].
Pacemaker insertion involves placing one or more leads inside the heart, which can cause direct injury to the heart’s tissue, potentially leading to inflammation of the surrounding pericardial and pleural areas [12].
Prevention and management: The management of PCIS involves the use of non-steroidal anti-inflammatory drugs (NSAIDs) and colchicine, which have been effective in treating acute pericarditis. In severe cases where complications such as cardiac tamponade occur, surgical intervention may be necessary. It is essential to initiate treatment early to avoid complications and ensure a favourable prognosis [9].
In the study by Greene et al., all 6 patients with acute symptomatic pericarditis were successfully treated with NSAIDs, resulting in symptom resolution within 2 weeks [10]. On the other hand, Zeltser et al. successfully treated most patients with NSAIDs and corticosteroids [11].
Corticosteroids should be reserved for severe cases that do not respond to NSAIDs, because steroids can promote chronicity and have numerous side effects [13]. Intravenous human immunoglobulins have also been observed to be efficacious steroid-sparing agents in refractory cases [14]. Pericardiectomy can be considered as a last resort if all medical therapy fails [9].
Preventive measures have mostly been studied in the context of cardiac surgery rather than pacemaker implantation. Perioperative administration of colchicine has been shown to significantly reduce the risk of PCIS, as shown by randomised control trials like COPPS and COPPS-2 [15].
To date, only 2 other cases of PCIS have been reported following TAVR. Llubani et al. documented a case presenting 8 months post-valve placement [16], while a case presented by Ngo et al. developed symptoms the following day [17]. Our case also presented 8 months after the procedure, but while the first 2 cases were successfully treated with conservative measures and responded well to NSAIDs and colchicine, our case required placement of a pericardial drain due to the presence of a large pericardial effusion. These instances underscore the importance of vigilant patient follow-up and awareness of the signs and symptoms of acute pericarditis, which may indicate the presence of this syndrome. Increasing awareness is crucial as the number of TAVI procedures continues to rise.
This diagnosis should be evaluated in patients who have undergone TAVR after excluding infection aetiologies, as well as in patients who present with chest pain, fever, fatigue, and elevated inflammatory markers.
In conclusion, PCIS is a potential complication following several invasive and minimally invasive procedures. With the rise in the use of various procedures, such as TAVR, it is vital for physicians to consider it as part of their differential diagnosis for patients with symptoms such as shortness of breath, pleuritic chest pain, fever, and leukocytosis and a history of such procedures.