Introduction
Superficial venous aneurysms (VAs) and pseudoaneurysms (VPAs) are two similar but distinct vascular lesions. Although their natural course is usually benign, they may be complicated with thromboembolism and rupture [1–3]. Despite their rarity in daily clinical practice, they should be acknowledged and included in the differential diagnosis of superficial masses. This rarity is also reflected in the literature; a degree of confusion exists in the terminology, and there is a lack of universal treatment guidelines.
We report a case of a right-hand superficial VA that was successfully treated by excision and ligation of the feeding vessels. We also present a review of the English literature focusing on the incidence, clinical presentation, histopathology, diagnosis, complications, and treatment of these venous aneurysms.
Case presentation
A 62-year-old man with a history of psoriasis presented to the outpatient department complaining of an enlarging mass on the dorsum of his right hand (Figure 1). He first noticed it 6 years previously, after lifting a heavy object. It progressively grew but remained asymptomatic. Upon examination, the mass was soft, easily compressible, non-tender, and non-pulsatile. It disappeared after raising the arm above heart level and reappeared in the dependent position. A superficial VA (1.5 cm × 2 cm in size) was diagnosed with color duplex ultrasound (CDU) examination (Figure 2). Magnetic resonance angiography (MRA) confirmed the diagnosis (Figure 3). The patient underwent total excision of the mass under local anesthesia with ligation of the feeding vessels, performed on an outpatient basis (Figure 4). He was satisfied with the medical and cosmetic results at 3-month follow-up. All three layers of the venous wall were present in the histopathology. Therefore, the diagnosis of a true venous aneurysm was made despite our suspicion of a VPA based on operative findings (considered saccular and not fusiform) and the history (suspected venous trauma during lifting a heavy object).
Figure 1
A superficial venous aneurysm about 2 cm in size lying in the dorsal aspect of the right hand (the skin was scrubbed before the operation)
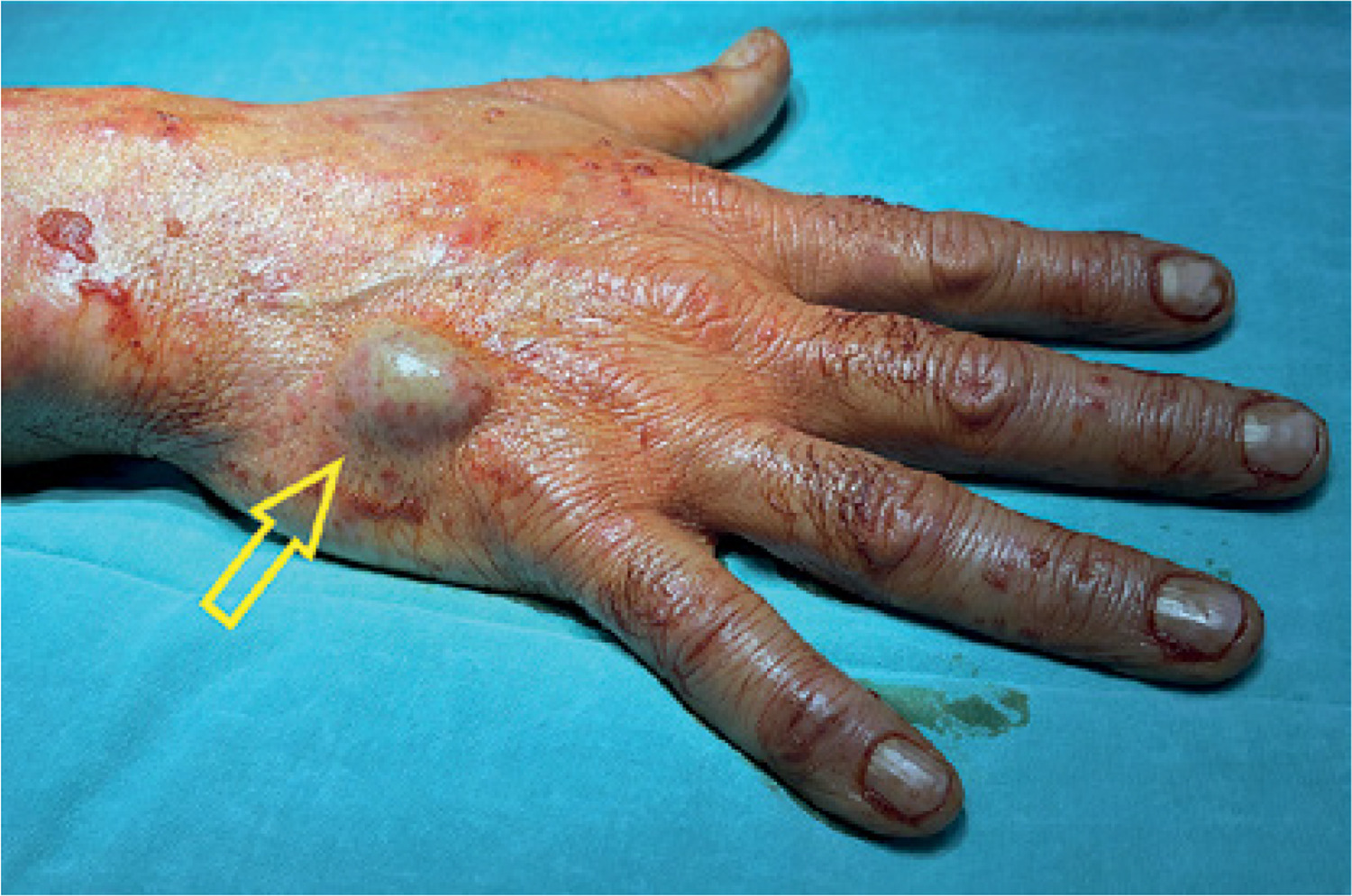
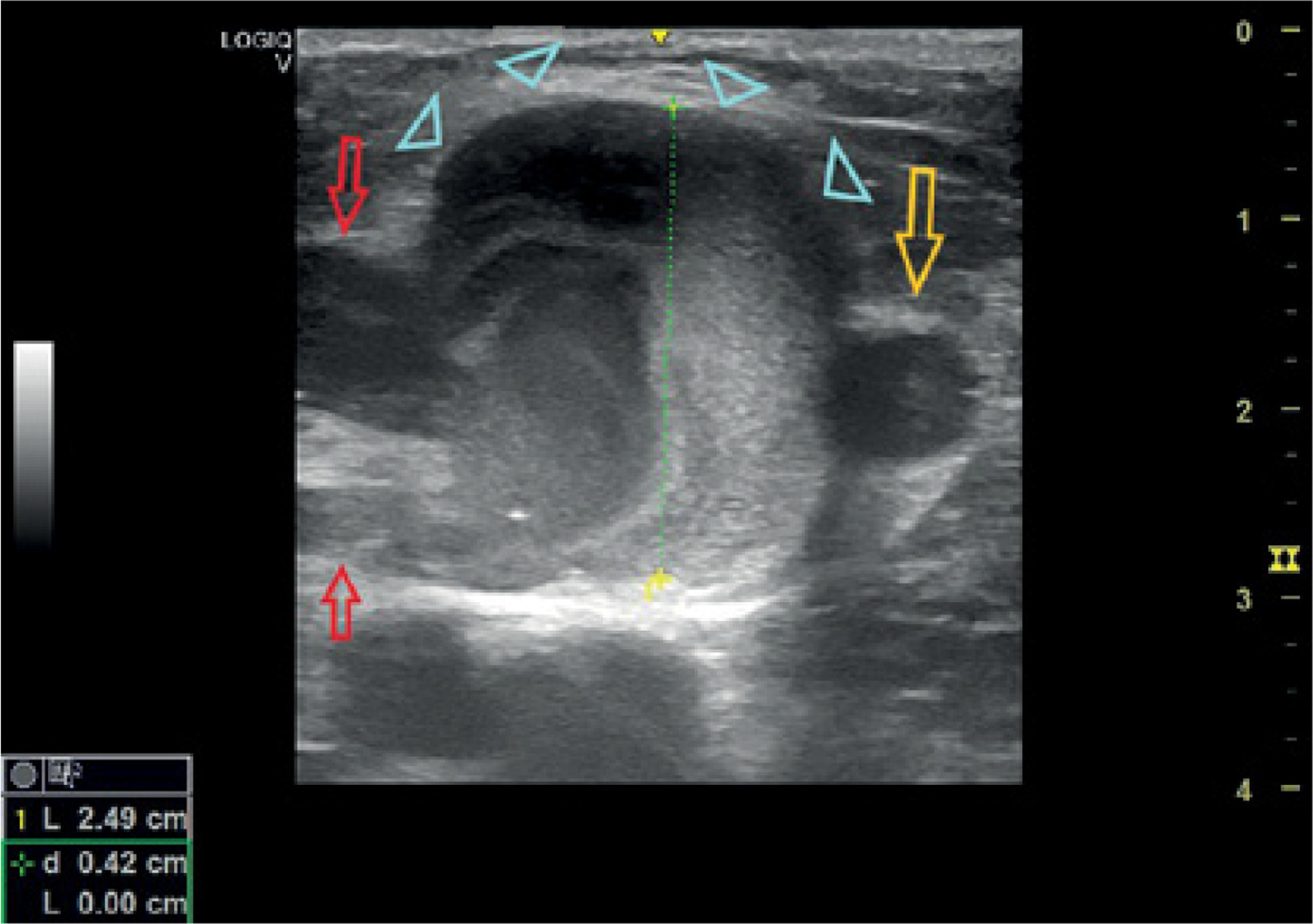
Figure 2
Color duplex ultrasound examination depicting the venous aneurysm with the “yin and yang sign” sign resulting from turbulent flow (arrow). This sign is usually seen in arterial aneurysms but may also be seen in venous aneurysms sporadically or during compression
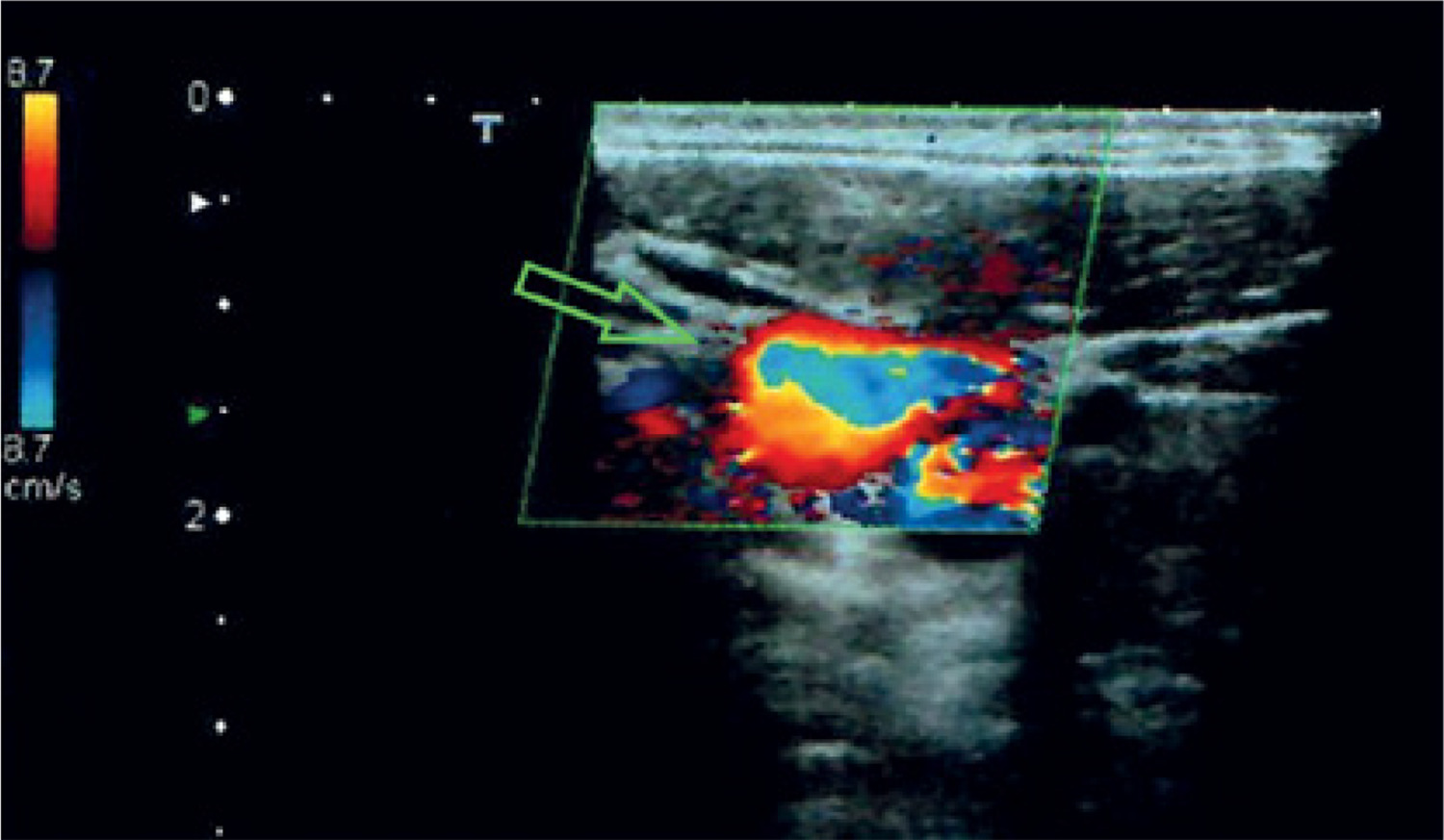
Figure 3
Magnetic resonance angiography (MRA) depicting the venous aneurysm (arrows). A – Coronal view. B – Oblique view depicting the feeding vessels. This saccular anatomy is usually seen in pseudoaneurysms, although it proved to be a true aneurysm in this patient. C – 3-D reconstruction. No connections with the arterial system were observed
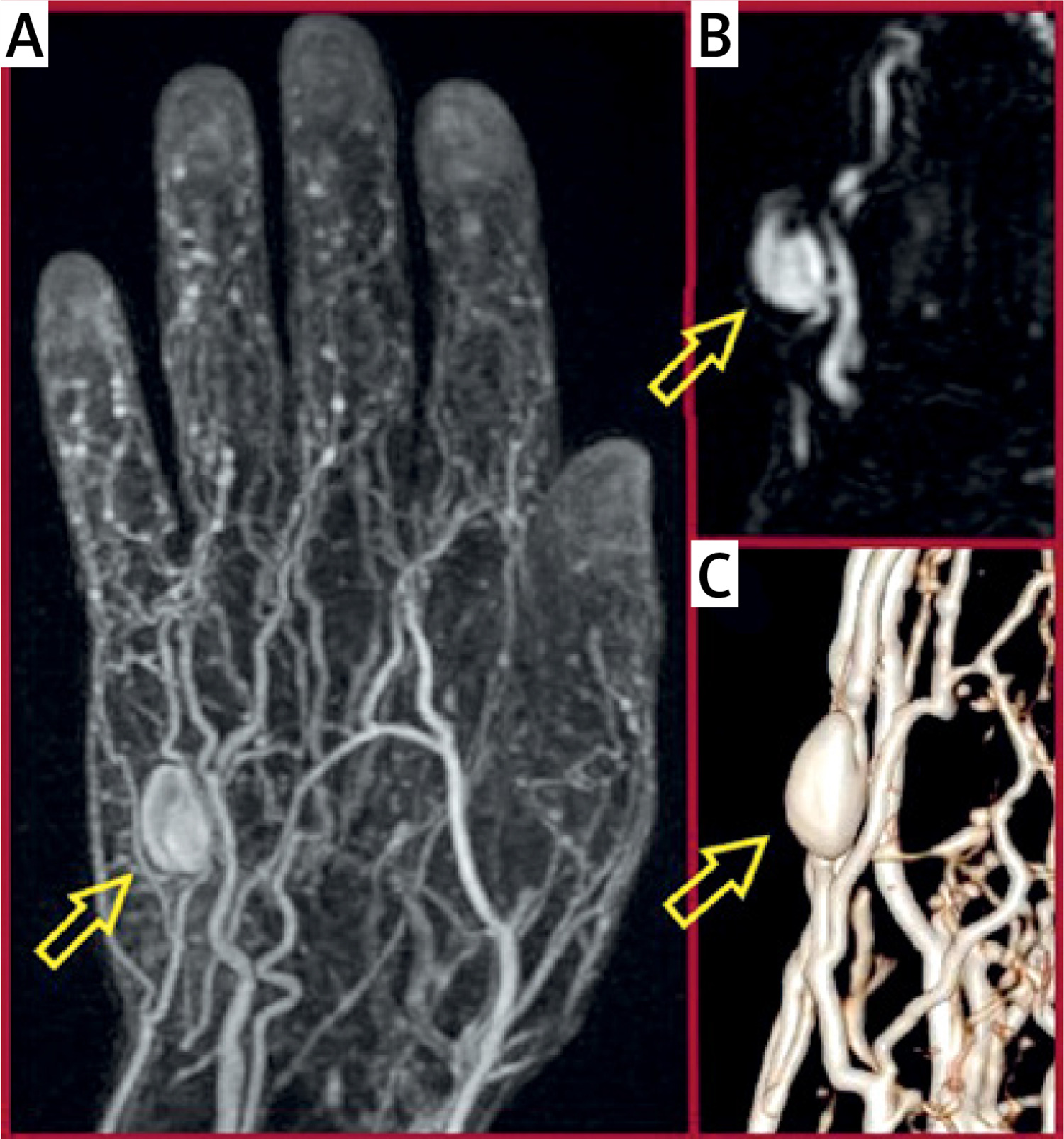
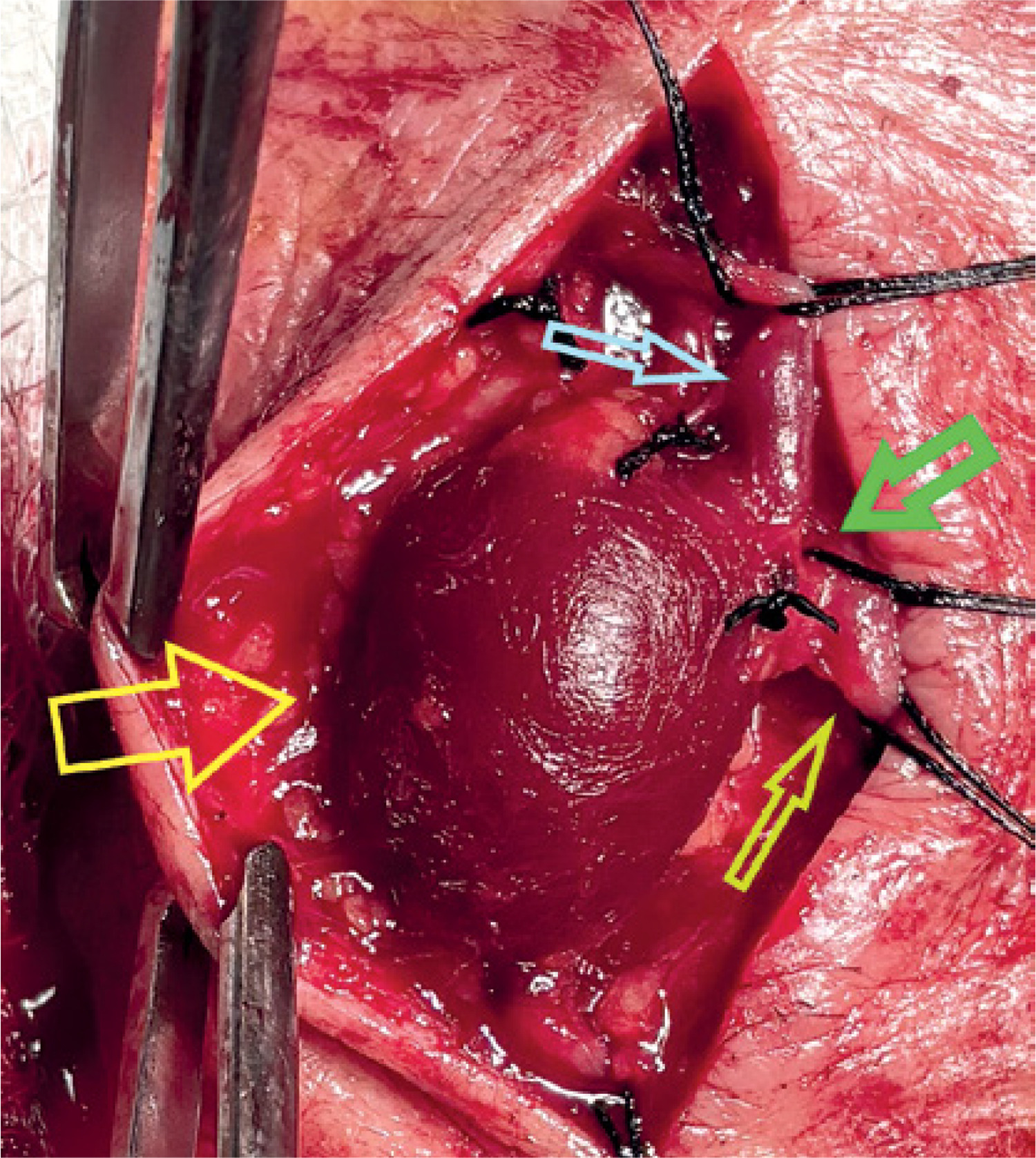
Figure 4
The aneurysm was dissected free from the surrounding subcutaneous tissues. A neck was revealed (green arrow), suggesting the diagnosis of a venous pseudoaneurysm (yellow arrow), which was not confirmed on histopathology. The efferent (light green arrow) and the afferent vein (light blue arrow) were evident
Discussion
Definition
A true VA is defined as a solitary venous dilation that contains all three layers of the vein [1, 4, 5]. Additionally, it should communicate with a main venous network by a single channel and not be associated with arteriovenous communication or a VPA [4, 6, 7]. Most importantly, it should not be contained within a varicose vein segment [1, 8, 9]. Currently, there is no consensus regarding specific diagnostic criteria for a VA [10–12]. Generally, it is defined by size > 3 cm or a diameter 1.5 times above the diameter of the adjacent normal vessel [13–18]. However, this definition is not always easy to apply, since many veins contain long dilated segments that meet these criteria [12, 14, 16]. Moreover, other veins show abnormalities consistent with VAs, but it is hard to characterize them as they run through a long course of varicosities [14]. Some suggest that a more accurate definition should include criteria regarding both the normal vessel diameter and the contiguous vein [10, 12, 17]. Others consider that the substantive identification of a VA requires a case-by-case approach [14]. Venous pseudoaneurysms are also a rare type of pathologic and localized vascular dilation [19]. Contrary to true VAs, there is a defect in the venous wall, usually after trauma, resulting in formation of a perivascular hematoma with ultimate fibrous encapsulation [19–21]. They have a neck through which the sac communicates with the vessel lumen.
Classification and epidemiology
Regarding morphology, VAs may be saccular, diverticular, or fusiform [22–24]. Saccular aneurysms are the most common, especially in the extremities and internal organs [25–27]. Fusiform aneurysms predominate in the cervical region [23]. Diverticular VAs are scarce in the literature and mostly occur in the cephalic vein, particularly in the distal forearm and the antecubital fossa [28].
Regarding pathophysiology, VAs are classified as either primary or secondary. Secondary VAs occur after trauma, infections, inflammation, venous valve insufficiency, or medical procedures including venous cannulation [4, 6, 15, 16, 18, 28–35]. They may arise from increased venous pressure in cardiovascular diseases or from venous compression by adjacent masses [25, 36, 37]. Rarely, a venous wall leiomyosarcoma may cause aneurysmal formation [38]. Secondary VAs arising from an arteriovenous fistula created for dialysis in chronic kidney failure represent a distinct clinical entity beyond the scope of this review [6, 22, 39]. Primary venous aneurysms are usually unilateral, and they can present at any age [9, 23, 25, 36, 40]. They have equal sex distribution, with a possible slight female predominance [18, 38, 34, 41–43]. Higher body mass index (BMI) values are related to a higher prevalence of venous aneurysms, since higher intraabdominal pressure increases reflux from incompetent valves and turbulent flow [15, 28, 44].
Regarding location, both primary and secondary VAs can occur in all major veins [29, 30, 35]. They are mostly found in the internal jugular vein, superior vena cava, lower extremities veins, and the portal vein [31, 36, 45, 46]. Upper extremity incidence is estimated at 4.2% [47]. They can be classified as either deep or superficial, depending on the location of the affected vein [28, 46, 48]. Superficial VAs are very rare, with an estimated incidence of 0.1% [27, 44, 48, 49]. Location in the upper extremities is even scarcer, with a few cases reported in the literature [50–52]. Cephalic VAs are considered the most uncommon of upper extremity aneurysms in the absence of an arteriovenous fistula [8]. Aneurysm diameters ranging from 1 to 7 cm have been reported in the literature [53]. We present all the superficial VAs of the upper extremity reported in the English literature so far (Table I).
Table I
Superficial venous aneurysms of the upper extremity
| Date | Author | Age Sex | History | Location | Size cm | Symptoms | Treatment | Follow up | Complications |
|---|---|---|---|---|---|---|---|---|---|
| 1962 | Schatz et al. [32] | 32 M | None | R forearm | 1.5 × 1.0 | Painless mass | Excision | – | – |
| 1990 | Perler et al. [76] | 39 F | None | R wrist | 3.5 × 1.5 | Rapidly enlarging mass, discomfort | Excision, local anesthesia | – | – |
| 1991 | Paes et al. [31] | 29 M | Chronic strain by repeated movement (oarsman) | R forearm, not otherwise specified | 2.0 × 3.0 . 3.0 × 4.0 | Enlarging painful masses | Excision, general anesthesia | 4 m | None |
| 1995 | Ekim et al. [74] | 17 F | None | R cephalic vein, multiple | 4.0 . 3.0 . multiple smaller | Tenderness in the forearm | Excision | 2 y | None |
| 1996 | Morrison et al. [33] | 40 F | None | L forearm | 2.0 | Enlarging mass, paresthesias | Ligation, excision | – | – |
| 1998 | Goto et al. [55] | 41 F | None | L cephalic vein | 2.5 × 1.5 × 1.0 | Enlarging mass | Simple excision, local anesthesia | 3 y | None |
| 2001 | Uematsu et al. [30] | 61 F | None | R basilic vein, multiple | 6.0 × 4.0 | Rapidly enlarging, painful mass | Excision, local anesthesia | – | None |
| 2001 | Wang et al. [78] | 67 M | None | R cephalic vein | 1.0 × 1.5 | Enlarging mass | Ligation, excision | 11 y | None |
| 2001 | Wang et al. [78] | 53 M | None | R cephalic vein | 3.0 | Mass | Ligation, excision | 9 y | None |
| 2005 | Yamamoto et al. [52] | 45 F | None | L 5th finger | NR | Painful mass | Ligation, excision | – | None |
| 2007 | Yaylak et al. [45] | 21 F | Cavernous hemangioma in R upper extremity | R basilic vein, multiple | NR | Painful, congenital mass | Acetaminophen for pain | – | – |
| 2007 | Faraj et al. [47] | 19 M | None | L cephalic vein | 7.0 × 2.0 × 1.0 | Enlarging mass | Excision, ligation | – | None |
| 2008 | Seo et al. [63] | 60 M | None | L forearm | 0.3 × 0.3 × 0.4 | None | 0.5% STS 0.4 ml | 1 m | None |
| 2008 | Irwin et al. [73] | 26 M | None | R forearm | 2.0 × 2.0 | Arm pain | Ligation, excision | – | None |
| 2008 | Irwin et al. [73] | 32 M | None | R hand | 2.5 × 2.5 | Hand pain | Ligation, excision | – | None |
| 2014 | Irwin et al. [74] | 82 M | Excision of similar mass in antecubital fossa 40 years prior | Bilateral forearm | 2.0 × 2.0 | Mass | Spontaneous rupture of R lesion | – | R lesion partially thrombosed |
| 2014 | Cakici et al. [77] | 61 F | None | R cephalic vein | 4.0 × 3.0 | Mass, wrist pain and numbness | Ligation, excision | 1 m | None |
| 2016 | Garetier et al. [51] | 37 M | Overweight, tophaceous gout | L index finger | 2.0 | Mass | Ligation, excision | – | None |
| 2016 | Naqvi et al. [49] | 35 F | None | R cephalic vein | 2.9 × 2.2 × 4.6 | Swelling, numbness in R thumb and index finger | Ligation, excision | 1 w | None |
| 2018 | McKesey et al. [15] | 59 M | BCC, SCC, actinic keratoses, lipomas | R wrist | 1.0 × 1.0 | Mass | None | – | – |
| 2018 | Weeks et al. [46] | 54 M | None | L cephalic vein | 1.5 × 0.9 × 1.6 | Enlarging, painful mass | Ligation, excision | 2 w | None |
| 2022 | Mahajan et al. [28] | 41 M | Related trauma 5y ago | R cephalic vein | 1.7 × 1.2 | Enlarging mass | Foam sclerotherapy | – | Pigmentation of skin, localized erythema |
Pseudoaneurysms (PAs) are usually traumatic in etiology [54]. The majority result from iatrogenic injury during central venous access manipulation [54]. We additionally present all the superficial PAs of the upper extremity reported in the English literature so far (Table II).
Table II
Superficial venous pseudoaneurysms of the upper extremity
| Date | Author | Age | History | Location | Size [cm] | Symptom | Treatment | Follow up | Complications |
|---|---|---|---|---|---|---|---|---|---|
| 1999 | Chakra-borty et al. [75] | 57 F | Mitral and aortic valve replacement, anticoagulation | L cephalic vein | 4.5 | Tender mass, restricted motion | Embolization | 6 w | None |
| 2002 | Jain et al. [88] | 28, ? | Blunt trauma to the area | Wrist | 3.0 | Painful mass | Sclerotherapy | 2 m | Partial occlusion but relief of symptoms Firm, noncompressible, tender lesion for 4–6 weeks |
| 2007 | Lotfi et al. [56] | 43 M | None | L median cubital vein | 3.0 × 1.5 | Tender swelling | Ligation, excision | – | None |
| 2008 | Min et al. [20] | 13 M | None | R cephalic vein | 3.0 × 3.0 × 2.5 | Enlarging mass, pain after exercise | Ligation, excision | 3 m | None |
| 2009 | Ward et al. [70] | 64 M | Afib under warfarin | R basilic vein | 4.3 × 3.3 × 2.0 | Swelling | Compression (failed), ligation – excision | – | – |
| 2017 | Niimi et al. [19] | 58 F | None | R basilic vein | 2.4 × 1.9 | Mass, sensory disturbance | Ligation, excision | 2 y | None |
| 2017 | Niimi et al. [19] | 56 F | None | L basilic vein | 2.3 × 1.7 | Mass | Ligation, excision | 6 m | None |
| 2023 | Sharda et al. [21] | 59 M | None | R cephalic vein | 2.0 × 1.4 | Enlarging mass | Excision, ligation | 3 m | None |
| 2024 | Kanani et al. [54] | 50 M | Related trauma 2y ago | R dorsum of hand | 1.7 × 1.4 × 1.0 | Painless swelling | Excision | – | – |
Clinical presentation
Unlike deep VAs, superficial VAs are usually asymptomatic [5, 13, 24, 33, 41, 55–58]. They present as a painless, palpable, and easily compressible bluish superficial mass, without detectable pulsation or bruit [47, 51, 59–62]. Presence of a bruit aids in the diagnosis of an arteriovenous malformation, or a traumatic arteriovenous fistula. The mass may be more prominent in the dependent position, during the Valsalva maneuver, or after exercise [62–64]. Most VAs increase in size over time [22, 46, 64]. When symptomatic, they may present with pain and moderate swelling or with limb edema [1, 2, 13, 65, 66]. Symptoms from adjacent structure compression (e.g. radial or median nerve compression) have occasionally been reported [56, 63, 67]. When located in the lower extremities, they may cause signs and symptoms of venous insufficiency such as pain, varicosities, skin changes, and stasis ulcers [38, 41, 68]. Severe venous insufficiency is a major risk factor for complications of superficial VAs [68]. Rarely, superficial VAs may be associated with thrombosis (superficial venous thrombosis, also known as ‘thrombophlebitis’ in the past) resulting in severe pain and tenderness [3, 4, 8, 15, 56, 57]. The mass becomes hard on palpation in this case [39, 51, 52, 61]. Thrombus extension to the deep venous system and pulmonary embolism have been reported [2, 3, 17]. Saccular aneurysms have a higher incidence of thromboembolic events, with presence of luminal thrombus and turbulent flow being risk factors for these complications [7, 42, 43]. Generally, superficial VAs have a marked lower risk for lung embolism compared with the deep ones. This difference may be due to the slower drainage of the superficial venous system, which makes it hard for the local thrombi to be dislodged [13, 14, 24]. Rupture is very rare, regardless of their site [3, 26, 27, 48, 64, 69]. Signs, symptoms and complications of superficial VPAs are very similar to true aneurysms [19–21, 54, 70, 71]. Finally, there are two reported cases of dissecting superficial VAs, with the one located in the upper extremity [47, 72]. It is likely a result of wall thinning and weakening of the medial layer due to reduction of smooth muscle cells and elastic fibers [72]. The morbidity of superficial VAs is estimated to be around 33% [8].
Histopathology
Histological findings of superficial VAs include thinning of the wall, reduction or absence of smooth muscle cells, increased number of endothelial cells, increase in fibrous tissue and disruption of elastic layers architecture (Figure 5) [22, 32, 64]. These changes may also be present in the adjacent, non-aneurysmal venous wall [8, 50, 58]. Smooth muscle cell loss may be congenital or due to replacement by hyalinized connective tissue [22]. Thrombus may be present with medial fibrosis in the area of thrombus adherence [30, 53, 63, 73]. As these pathological findings are also apparent in varicose veins, Pascarella et al. [34] suggested that superficial VAs are advanced and localized forms of varicose veins and may be promoted by the same hemodynamic factors [34, 24, 68]. Other researchers highlight their histological differences and support that venous aneurysms and varicose veins are two distinct pathological entities [8, 44]. More precisely, varicose veins are characterized by elongation of the vein, thickening of the muscle layer and venous wall, and by a decreased fibrinolytic activity [8, 72]. Irwin et al. found that varicose veins present with asymmetric thinning of the venous wall and increased mast cells when compared with venous aneurysms, and this asymmetry is also characteristic of VAs [73]. Venous aneurysms secondary to venous hypertension may resemble varicose segments, showing hypertrophy of the muscular layer of the wall [17]. In chronic lesions, the vessel is further dilated, with elongation of the muscle fibers and disruption of the internal and external elastic membrane [17]. An inflammatory reaction, especially in areas of thrombus, may also be present in all layers of the venous wall, with the presence of both macrophages and mast cells. It seems to be dependent on the degree of inflammation [53, 56, 73, 74]. Despite being quite an impressive finding in many cases, it is mostly considered an epiphenomenon rather than a cause of the aneurysm [35, 36, 55, 74]. The differences in histological findings between different reports may stem from diverse etiology and could aid in differential diagnosis of a primary aneurysm and a secondary lesion due to trauma, venous hypertension, etc. [60].
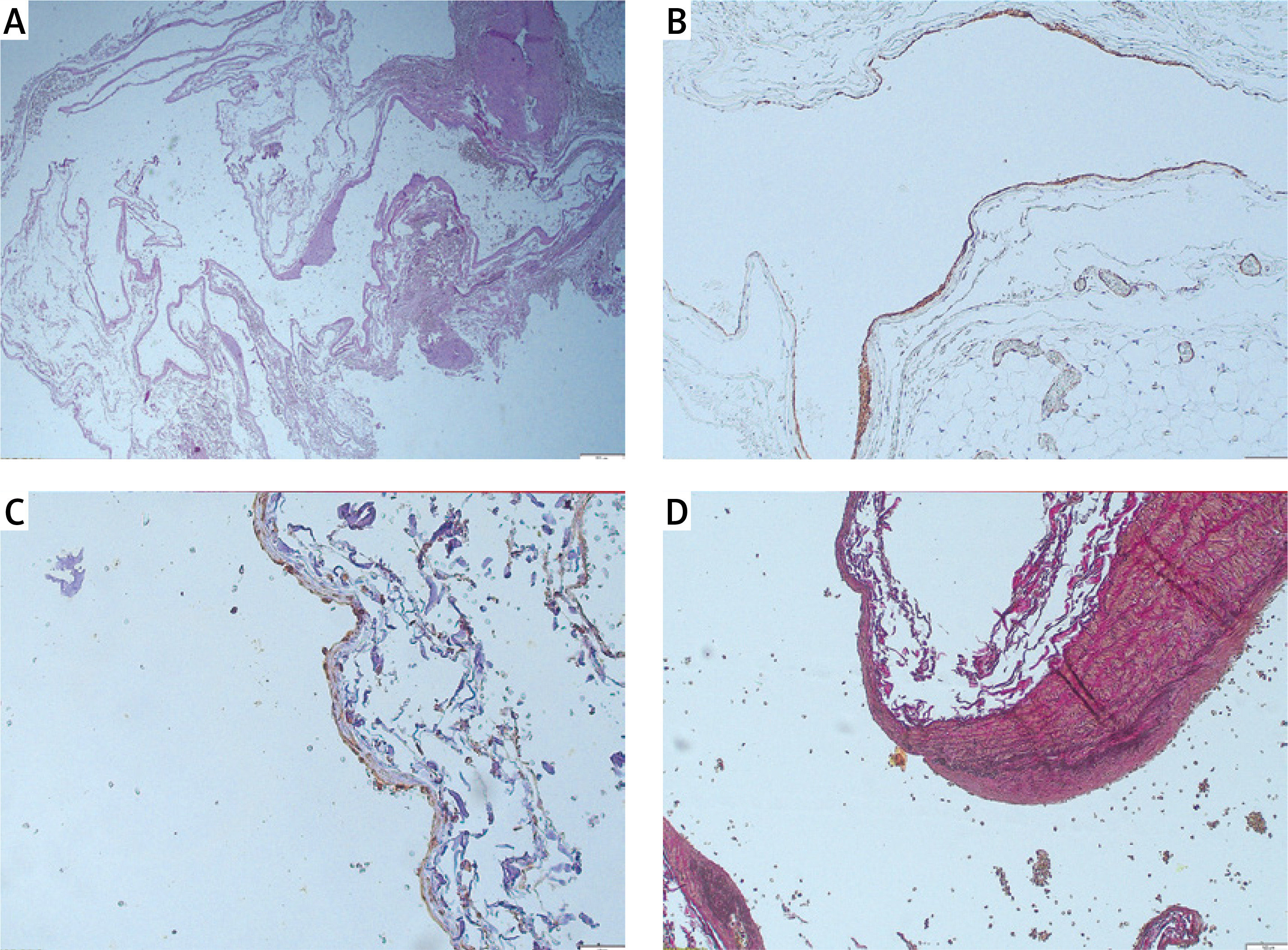
Figure 5
Histopathology: A – Thinning of the wall and dilation greater than 1.5 times the diameter of the vein (H/E – hematoxylin and eosin, ×2). B – Reduction or absence of smooth muscle cells (SMA – smooth muscle actin, ×10). C – Immunohistochemical stain for ERG shows the endothelial lining of the vessel (×20). D – Histochemical stain for elastic fibers highlights the disruption of the architecture of elastic fibers and illustrates the absence of an external elastic lamina and a thick internal elastic lamina, indicating the venous nature of the vessel
Regarding venous PAs, the histology is quite different. The wall is composed mainly of fibrous tissue, with some smooth muscle cells, confirming its venous origin [20, 59]. There is no vascular endothelium in the lining, and there may be thickening of the media in the venous wall, suggesting arterialization [19, 75].
Etiology and pathogenesis
The etiology of primary VAs remains unknown [65, 76, 77]. There are no reported cases of patients presented with both arterial and VAs simultaneously or in a metachronous setting. Consequently, different driving mechanisms should be encountered in these two entities [26, 44]. Increased venous outflow causes hypertrophy of the venous wall and eventually dilatation and sclerosis [30, 58, 60]. External forces may contribute, as VAs are often observed in areas of mechanical stress, such as tributaries close to the arteries [47, 55, 60]. Schatz and Fine [32] posited that endophlebohypertrophy and endophlebosclerosis are the major pathophysiologic mechanisms resembling the pathogenesis of arterial aneurysms [59, 62, 63]. Endophlebohypertrophy is a normal response to mechanical stress beginning at birth, whereas endophlebosclerosis is a degenerative process [45, 58, 78].
Congenital weakness of the venous wall from connective tissue degeneration has been described in connective tissue disorders, such as Marfan and Ehlers-Danlos syndrome [35, 76, 77, 79]. Focal defects in the media have been observed in these cases [49, 55]. In fact, local inflammatory processes, endophlebohypertrophy, and congenital defects could work in synergy to drive the pathogenesis of a venous aneurysm [43, 47, 55].
Irwin et al. identified increased expression of metalloproteinases (MMPs) 2, 9, and 13 in smooth muscle cells, extracellular space, and microvascular endothelial cells lining the adventitial vasa vasorum in venous aneurysms [42, 48, 74]. Over-expression of MMPs could explain the elastic fiber disruption, although their production is not sufficient to account for the venous wall alterations [44, 68, 73, 77]. On the other hand, MMPs 2, 9, and 13 have rarely been observed in varicose vein segments [73]. Whether they are involved in venous dilation or are merely a result of the inflammatory process remains to be studied [73].
Venous valve insufficiency could also promote venous dilation due to the turbulent reflux flow [46, 64, 68]. There is a relationship between venous insufficiency and venous aneurysms in the lower limbs. However, as chronic venous disease is much more prevalent than venous aneurysms, it cannot be the only driving factor [68]. Certain cardiopathies or venous pulmonary anomalies that decrease the blood flow to the right heart chambers could also be involved in venous aneurysm pathogenesis [69]. Finally, hormonal and hemodynamic changes during pregnancy may play a role in venous aneurysm formation [35, 65], despite the unilateral appearance of these lesions in most cases [65]. Therefore, both intraluminal and external factors may be responsible for aneurysm formation [30, 58].
Some syndromes may predispose to development of venous aneurysms, especially in the superficial system. A patient with hyper-eosinophilic syndrome and multiple deep and superficial VAs has been reported, although the arterial system is involved more often [80]. Weakening of the venous wall due to degranulation and release of cytokines and free radicals after eosinophilic infiltration has been suggested [80]. Primary deep or superficial VAs in young adults are most often associated with Klippel-Trenaunay syndrome [15, 41, 81]. It is thought to be caused by a developmental mesodermal anomaly, causing weakening of the vascular wall [41]. A probable genetic cause has also been discussed, but due to the limited patient sample the results are not definite [81].
Although there are no case reports describing VAs resulting from weightlifting so far, systematic weight training may be implicated in VA development. Exercise-induced increases in blood flow, venous return, and circulating volume promote increased venous diameter and compliance [82–84]. Elevated intraluminal pressure is a recognized contributor to venous degeneration and aneurysm formation; therefore, it is plausible that repeated strain from physical activity could contribute to venous aneurysm formation in predisposed individuals (Figure 6).
Figure 6
A focal dilatation of the right cephalic vein in a young patient representing a superficial venous aneurysm (light green arrow). He engages in regular resistance/weight training recreationally

The pathogenesis of VPAs is unclear. Although arterial pseudoaneurysms are a common complication of vascular puncture, there are few reports of iatrogenic VPAs [20, 21, 70]. This may be attributed to the lower venous pressures, leading to a hematoma and not a VPA after a vein wall injury [20, 21, 70]. Another difference between arterial and VPA is that the first usually occur in anticoagulated patients, while there seem to be no such relation in the latter [56]. Iatrogenic arteriovenous fistula or other forms of arteriovenous communication could be a predisposing factor for venous pseudoaneurysms, as they cause increased pressure in the venous system [85]. Other possible causes of venous pseudoaneurysm include surgical maneuvers and non-iatrogenic causes, such as trauma or intravenous drug abuse [70, 79]. There are also two reports about non-iatrogenic, non-traumatic VPAs in 2 patients with clear medical histories and no known comorbidities [20, 21]. The pathogenesis remains unclear [20].
Differential diagnosis
Both superficial VAs and PAs are often misdiagnosed, as they may mimic other soft tissue masses [61, 63, 65, 69, 77, 78]. The differential diagnosis includes varicose veins, diffuse phlebectasia, cysts, lymphoceles, hygromas, abscesses, hemangiomas, angiokeratomas, other venous malformations, inflammatory lesions, inguinal or femoral hernias, and soft tissue tumors [3, 5, 9, 10, 11, 15, 27, 40, 74, 46, 48, 54, 57, 58, 63, 65, 69, 77, 78]. The exact location of the lesion aids in the diagnostic process. True and false aneurysms may complicate an arteriovenous fistula during its lifetime (at about 7–17%) and they are known as vascular access aneurysms. Arterialization of venous circulation is apparent in the outflow tract, including the aneurysms [86].
Imaging methods
Diagnosis of superficial VAs is primarily clinical [59, 64, 76]. Color duplex ultrasonography (CDU) is the first examination, as it is a non-invasive, inexpensive, and accurate technique [41, 45, 50, 58, 66, 87]. The VA appears as an anechoic cystic lesion in continuity with a superficial vein, which may contain hyperechoic intraluminal floating thrombus [4, 28, 46, 63]. It is easily compressible when probed and expands after pressure is released [46, 63]. CDU differentiates between arterial and VAs and depicts the feeding vessels [41, 48, 50, 57, 61]. The so-called “yin and yang sign” seen in arterial aneurysms, due to turbulent flow, may appear spontaneously or during compression in VAs [12, 46]. However, CDU may fail to diagnose a superficial VA when the feeding vessels are too small, the aneurysm is thrombosed, or in cases of complex anatomy and special patient habitus [52, 68].
Computed tomography (CT) and magnetic resonance imaging (MRI) [37, 61, 87] accurately reveal the lesion’s size and morphology, confirming its vascular origin [26, 37, 51, 61, 63, 87]. They are especially useful to delineate any diagnostic uncertainty or in complex venous anatomy [14, 26, 41, 44]. Attenuation on CT images depends on aneurysm patency and thrombus age, if apparent [28, 46]. Dynamic enhanced CT shows a slight enhancement in the early (arterial) phase and homogeneous enhancement in the late phase [4]. MRI may not be helpful in thrombosed aneurysms, as the findings are non-specific (mildly hyperintense to muscle on T1-weighted images with heterogeneously increased signal intensity on T2-weighted images). Additionally, a flow-sensitive gradient-recalled pulse sequence cannot demonstrate vascular flow [33]. The finding of a peripheral, high-intensity crescent in the T2 sequence could help differentiate a venous aneurysm from neoplasms, where central hyperintensity is more common [33]. Krinky et al. described the “layered gadolinium sign” on MRI [60]. Phlebography may also aid in diagnosis [68, 76, 87], by depicting any intra-sac thrombus or the communicating veins [49, 68, 76, 87]. However, it cannot diagnose a thrombosed aneurysm and, moreover, it was responsible for fatal emboli formation [24, 25, 64, 78]. Isotopic 99mTc human serum albumin angiography has also been used [60]. The gold standard for VPAs is magnetic resonance angiography (MRA) [54, 70]. It may be performed preoperatively, at the discretion of the treating physician, to provide a more detailed anatomy of the lesion and identify a possible arteriovenous communication or a different vascular anomaly. Definite diagnosis is established by histopathological examination which confirms the absence of smooth muscle cells (antidesmin Ab) [27, 58].
Regarding PAs, the presence of recent trauma in patients’ history (e.g. venipuncture) is crucial [75]. The rest of the physical examination and imaging workup is identical to that of superficial VAs [19, 20]. CDU shows a swirling pattern of blood flow and the aneurysm neck, which represents the communication with the vein [19, 21, 54, 70]. The “eccentric ripple sign of BAARISh” on dynamic ultrasound refers to a ripple effect of retrograde flow after transducer pressure on the draining vein [54]. Diagnosis of a PA is confirmed with histopathological examination after resection and not during surgical exploration [46, 52, 56, 58, 75].
Therapeutic approaches and outcomes
Indications for treatment include symptomatic or enlarging lesions, increased risk for thrombus formation, any diagnostic uncertainty and, most commonly, cosmetic issues [64–66]. Saccular aneurysms of any size and large fusiform aneurysms should also be considered for intervention [60]. Although there is no agreed size criterion for superficial VAs, 20 mm has been used as the threshold for popliteal venous aneurysms in the deep venous system [11, 26, 60]. The method of treatment depends largely on anatomic location [10, 87]. Similarly, venous pseudoaneurysms with thromboembolism risk or other complicating features should not be left untreated [19, 20, 70].
Surgical excision is the treatment of choice, especially when anticoagulation is ineffective [19, 70]. It allows immediate relief and complete removal of the lesion, while allowing histological examination to confirm the diagnosis [65, 70]. It consists of simple ligation and excision [2, 31, 77]. May-Thurner and Klippel-Trenaunay syndrome should be excluded before surgery [2, 38, 41]. Alternative techniques include venorrhaphy or vein patching after resection of the excess aneurysmal wall or excision with interposition vein grafting [62, 64, 66]. Aneurysm location plays a role in the treatment plan. The first technique with venorrhaphy has been associated with early occlusion and has little to offer over simple ligation [8, 58]. However, it could be considered in young patients with aneurysms close to the saphenofemoral junction, to fully preserve the superficial venous outflow [11]. Complications of surgical approach, although rare, include hematoma, wound infection, thrombophlebitis, nerve injury and recurrence [1, 38, 42]. Surgical intervention is preferred in lesions with proximity to nerve structures [77]. The risk of recurrence after treatment is minimal to none [65]. Infected pseudoaneurysms are always treated surgically with complete excision of the involved vein [71].
The role of postoperative anticoagulation has not yet been clarified and depends on the physician’s preference [11]. A 3- to 6-month course should be considered in the context of pulmonary embolism (PE) or in the presence of risk factors for PE and in venous thrombosis or other thromboembolic complications [42, 64, 66]. Although exceptionally rare, an inferior vena cava (IVC) filter could be considered for patients who cannot receive anticoagulation, or in severe PE with hemodynamic instability [16].
Ultrasound-guided compression is widely used in arterial pseudoaneurysms and can also be used for venous pseudoaneurysms but is not likely to succeed in chronic lesions or anticoagulated patients [56, 70, 75].
Sclerotherapy acts by damaging the vascular endothelium, resulting in thrombotic occlusion and fibrosis [88, 89]. Most sclerosing agents show efficacy and excellent cosmetic results, but more research is needed in VAs and VPAs, as limited data are available [63]. Polidocanol is a widely used sclerosing agent. Sclerotherapy can also be used in residual lesions after previous treatment [28, 63, 65, 77, 78]. Complications include pain, superficial erythema, skin induration, telangiectatic matting (15–20%), hypertrichosis, and hyperpigmentation [28, 88, 89]. Hyperpigmentation may be due to an inflammatory reaction after leakage of the sclerosing agent [89]. It usually resolves after 6–12 months but may be permanent in 1–2% of patients [89]. Other complications are thrombophlebitis (4–7.5%) of the feeding veins and, rarely, pyoderma gangrenosum [65, 88, 89]. Nerve injury may also occur, depending on the location [89]. Cutaneous necrosis is a serious complication which may result after exsanguination of any sclerosing agent but does not always represent physician error [89]. Exceptionally rare complications may be encountered such as acute ischemia, necrotizing fasciitis, cerebrovascular adverse effects, epileptic seizures, cardiac toxicity, pulmonary embolism, deep venous thrombosis, and serious anaphylactic reactions [89]. In our patient, we decided not to proceed with sclerotherapy but with open surgery, as the aneurysm was located at the dorsum of the hand. Concerns were raised about inflammatory involvement of nearby nerves, as these nerves are responsible for motor/sensory functions.
Endovenous laser (EVLA) or radiofrequency ablation (RFA) is an alternative treatment option for superficial VAs with large feeding veins [49, 63, 87]. This is especially true in VAs located in the route of great and small saphenous veins or in their accessory branches [90]. Ablation has a low rate of recanalization and reflux (higher with RF compared to EVLA) [91]. This may be a result of the thickening of the venous wall due to chronic inflammation [68]. They are contraindicated in larger lesions (above 2.5–3 cm) as failure rates are increased [14, 34, 68, 91, 92]. Rare complications include damage to the adjacent skin or neuromuscular structures, as well as endothelial heat-induced thrombosis (EHIT) leading to deep venous thrombosis (DVT) and PE [38, 91]. For superficial VAs close to the saphenofemoral or saphenopopliteal junction, safe ablation can be performed only if lesions are > 3 cm from the junction. If the distance is < 3 cm, ablation should be performed only after open excision and high saphenous ligation (Figure 7) [10].
Figure 7
A 50-year-old man presented with a palpable venous aneurysm (2.5 cm in diameter) near the saphenofemoral junction (at about 1 cm distally). He complained about periodical mild pain. He had abdominal surgery for trauma 7 years previously, but no trauma in the inguinal area was reported (orange arrow: great saphenous vein, light blue arrowheads: venous aneurysm, red arrows: draining veins to the anterior accessory saphenous branch) (Supplementary material)
Coil embolization, stenting, or thrombin injection can be used instead of surgery especially in patients who are not able to stop anticoagulation due to other comorbidities [56, 60, 70, 75, 93]. Embolization has a higher possibility of failure than surgical excision [56, 75]. There is a small risk of coil migration and distal embolization. Both embolization and percutaneous thrombin injection may cause persistent mass effects after treatment, especially in larger peripheral lesions [70]. Other complications include development of mural thrombus, late stenosis or vessel occlusion from intimal hyperplasia and stent fracture [93]. Nevertheless, surgery is not compromised by previous endovascular treatment [75]. Edema and neuralgia after surgical exposure have been reported [93]. Postoperative anticoagulation may be needed, and lifelong follow-up is recommended [93].
Finally, we must emphasize that in some cases, clinical observation aided with CDU imaging may be adequate and no intervention is warranted [60, 63, 66]. This is true for small, fusiform superficial VAs without thrombus formation, as they carry a very small risk of complications [43, 60, 66].
Review of the literature
We performed a scoping review of the English literature available up to June 10th 2025 on the PubMed and Google Scholar databases. The retrieved records were screened for relevance to superficial venous aneurysms of the distal upper extremity, and superficial venous pseudoaneurysms of the upper extremity. The references in the relevant articles were checked to identify additional resources. Duplicate articles were removed. Keywords included: superficial venous aneurysm, venous pseudoaneurysm, superficial venous false aneurysm. Secondary VAs arising from an arteriovenous fistula were not included in this review.
Superficial venous aneurysms
Twenty-two patients with true superficial VAs of the distal arm were identified. There were 13 male and 9 female patients, aged 17 to 82 years. Aneurysm size ranged from 0.4 cm to 7 cm. The cephalic vein was affected in 9 patients, basilic in 2, and unidentified in 11. Five patients had multiple aneurysms. Possible traumatic etiology due to injury or excessive strain was identified in 9.1% and 2 cases had a history of previous vascular malformation or vascular tumor, suggesting a possible congenital defect [28, 31, 45, 73]. Both patients presented with multiple lesions. Symptoms included asymptomatic mass (45.5%), pain (36.4%) or discomfort (9.1%), swelling (4.5%), and paresthesias (13.6%). Most patients (77.3%) underwent surgical excision with ligation of the feeding vessels, without complications. Two cases were managed conservatively [15, 45], and one experienced spontaneous rupture with partial thrombosis prior to surgical treatment [15, 45, 73]. Two patients underwent sclerotherapy; one developed pigmentation of the skin and local erythema [28]. Table I includes all reported cases of superficial VAs of the upper extremity, focusing on history, location, size, symptoms, management, and outcome.
Superficial venous pseudoaneurysms
Nine superficial VPAs of the upper extremity were identified (5 male, 3 female, and 1 unidentified) with an age range of 13 to 64 years. Diameter ranged from 1.7 to 4.5 cm. Etiology included traumatic (n = 2) and anticoagulation-related (n = 2). In the remaining cases, no known etiology was identified. Three cases involved the cephalic vein, 3 the basilic vein, 1 the antecubital vein, and 2 were unspecified. Symptoms included pain (n = 2), tenderness (n = 2), swelling (n = 3), restricted movement (n = 1), and sensory disturbance (n = 1). Seven patients underwent surgical excision with ligation of the feeding vessels, including one failed prior compression therapy [70]. No complications were reported. One patient was successfully managed with catheterization and embolization of the feeding vessels [75]. One patient underwent two sessions of sclerotherapy, achieving partial occlusion and symptom relief. Table II includes all reported cases of superficial PAs of the upper extremity, focusing on history, location, size, symptoms, management, and outcome.
Two additional images from patients who presented in our clinic upon completion of this review are included (Figures 6 and 7). Although not analyzed extensively, they provide further insight and offer further illustrative value.
Conclusion
Venous aneurysms and VPAs are rare entities, usually asymptomatic, but may pose significant diagnostic and therapeutic challenges [1–3]. Excision with ligation of feeding vessels is preferred over sclerotherapy and embolization. Further research, including larger case series, is warranted to guide management decisions and clarify intervention thresholds, particularly in asymptomatic patients.