
Introduction
Almost 20–40% of the adult population all over the world and approximately 50–75% of patients with type 2 diabetes (T2D) are diagnosed with non-alcoholic fatty liver (NAFL: histologically documented 5% fat or more in the liver) disease (NAFLD), after the exclusion of excess alcohol intake (recent or ongoing) and other causes of secondary or monogenic liver steatosis [1]. The prevalence of NAFLD varies significantly between different geographic areas and by ethnicity [1, 2]. It is growing dramatically even in children and young adults [1–3]. NAFLD is tightly associated with the global pandemic of obesity, metabolic syndrome (MS) and T2D, as well as with several genetic factors. Insulin resistance (IR) is one of the most crucial factors underlying its pathogenesis and significant determinant of its progression to non-alcoholic steatohepatitis (NASH: at least 5% fat in the liver in relation to histologically proven hepatocellular inflammation and injury, with or without evidence of pericellular fibrosis) [1, 2, 4]. The pivotal role of central dysfunctional, insulin-resistant adipose tissue to the evolution of advanced fibrosis in patients with T2D and NAFLD, beyond body mass index (BMI) or steatosis, has been well established [5]. Furthermore, the stage of hepatic fibrosis is the key determinant of future evolution of liver-related complications [4, 5].
In June 2023, an international, multi-society guided Delphi process established the definition of metabolic dysfunction-associated steatotic liver disease (MASLD), which is defined as the presence of high triglyceride (TG) storage inside the hepatocytes in the presence of at least one cardiometabolic risk factor, trying to unveil the nuances of a heterogenous and complex disorder [6, 7]. MASLD consists of different conditions, including isolated liver steatosis (metabolic dysfunction-associated steatotic liver, MASL), metabolic dysfunction associated steatohepatitis (MASH), as well as fibrosis and cirrhosis. Indeed, there is almost a complete overlap between NAFLD and MASLD populations in several epidemiological studies, while only 5.3% of individuals with NAFLD did not fulfil the MASLD criteria in the population-based Nutrition Examination Survey (NHANES III) [6, 8]. Unfortunately, NAFLD is often underdiagnosed because of its asymptomatic nature, the absence of standardized diagnostic assays in everyday clinical practice and the lack of awareness among individuals and physicians (less than 5% of individuals with NAFLD are aware of their disease) [1, 6, 9].
It is estimated that 10–30% of individuals with NAFLD can be complicated by NASH and approximately 20% of individuals with NASH will progress to cirrhosis, hepatocellular carcinoma and/or liver failure; the presence of IR is associated to higher rates of liver-specific and overall mortality [9, 10]. Indeed, NAFLD has been identified as the cause of many cases previously defined as cryptogenic cirrhosis, while NASH is the second most common factor for liver transplantation in the USA after hepatitis C [11, 12]. However, many studies and meta-analyses suggested that individuals with NAFLD experienced significant risks for subclinical and clinical cardiovascular events, even after adjustment for atherosclerotic cardiovascular disease (ASCVD) risk factor covariates, establishing ASCVD together with extrahepatic malignancies (mostly gastrointestinal and thyroid) as the leading causes of morbidity and mortality in individuals with less advanced disease [13–15]. Interestingly, a large meta-analysis that included data from 34,043 individuals with NAFLD, who were diagnosed either with imaging studies or histological evidence and were followed over a median period of 6.9 years, suggested that there was a 64% higher risk for experiencing both fatal and nonfatal cardiovascular events vs. those without NAFLD [16].
NAFLD: pathophysiological aspects
Long before individuals with IR experience defects of glucose metabolism, increased circulating levels of non-esterified fatty acids (NEFAs) are found. The main mechanism underlying this phenomenon is the loss of the suppressive activity of insulin to regulate lipolysis in a metabolic dysregulated visceral adipose tissue, even during times of nutrient excess [17]. Increased levels of NEFAs in the liver are mainly the result of: (i) stimulated lipolysis from visceral fat (hormone-sensitive lipase cannot be sufficiently downregulated). The higher the ambient levels of insulin, the bigger the degree of NEFAs that penetrate the liver; (ii) de novo lipogenesis from excess carbohydrates (glucose and fructose). This is achieved after the activation of the transcriptional regulator sterol regulatory element-binding protein 1c (SREBP-1c) that is extremely sensitive to hyperinsulinemia and the carbohydrate response element-binding protein (ChREBP), although its expression is suppressed in individuals with NASH and (iii) the metabolism of intestinal chylomicrons that penetrate the liver through the portal system [9, 10, 17].
After entering the liver NEFAs: (i) can be transported into the mitochondria and metabolized through β-oxidation. During an IR state mitochondrial oxidative phosphorylation is suppressed (because of mitochondrial dysfunction and/or reduced mitochondrial content); (ii) can be converted to neutral TG, packaged into very-low-density lipoprotein cholesterol (VLDL-C) particles and secreted into the circulation, while intrahepatic TG are stored as intracellular lipid droplets contributing to the fatty acid pool inside hepatocytes and (iii) glycerol substrates and odd chain NEFAs can be used during gluconeogenesis. When these cellular pathways are overwhelmed and hepatic lipid storage overcomes lipid clearance and utilization, excess intrahepatic TG levels can form cytosolic intracellular fat droplets and eventually steatosis [9, 17]. Moreover, increased VLDL-C secretion promotes excess ectopic fat accumulation (including the pancreas), in case the subcutaneous adipose tissue cannot efficiently store the excess TG. Fatty infiltration of the pancreas promotes impaired pancreatic β-cell function and gradual hyperglycemia, which will further enhance de novo hepatic lipogenesis and promote higher NEFAs levels to the circulation (the twin cycle hypothesis) [18]. After fatty infiltration of the pancreas, beta (β)-cell dysfunction was tightly connected to the presence and severity of NAFLD creating a vicious-cycle of a feed-forward effect [19, 20]. Furthermore, when the delivery rate of NEFAs inside hepatocytes exceeds the rate of intracellular β-oxidation and/or formation to neutral TG, excess NEFAs can enter into harmful non-oxidative pathways. Hence they stimulate the accumulation of lipid intermediate metabolites [lysophosphatidic acid (LPA), diacylglycerol (DAG), acylcarnitines and ceramides], which promote defects of the insulin signaling pathway, exacerbate IR and stimulate several signaling pathways related to inflammation and oxidative stress, creating a second vicious-cycle of a feed-forward effect [17, 21–23].
Several mechanisms including glucotoxicity, lipotoxicity, altered secretion of adipokines/cytokines, hepatokines (mainly higher circulating fetuin-A levels), stimulation of multiple inflammatory pathways, reduced bile-acid synthesis, endoplasmic reticulum stress, increased oxidative stress, mitochondrial dysfunction and alterations in gut microbiota/gut-derived endotoxins, in a complex interplay with genetic predisposition, drive the evolution of inflammation, hepatocellular injury and fibrosis [24–26].
NAFLD during a diabetic state: therapeutic approach
Lifestyle modifications (dietary changes and the implementation of healthier eating patterns (such as the Mediterranean diet), as well as increased physical activity through participation in a structured exercise program) are the cornerstones for the management of individuals with NAFLD and excess adiposity. Weight reduction at least 5% and preferably 10% or more, can be associated with greater histological liver improvements and cardiometabolic benefits; however preventing the progression to fibrosis varies among individuals, is less predictable and there is no definite threshold to reverse inflammation and/or fibrosis [27–30]. In most of the current studies there was a dose-response association between weight reduction and histological hepatocellular improvement. Nevertheless, lifestyle changes require stable and durable adaptation on a life-long basis, which remains difficult and challenging [31, 32]. Bariatric surgery in proper candidates can be effective and safe for improving steatosis, inflammation and to a lesser degree liver fibrosis and must be carefully evaluated in individuals with cirrhosis [33, 34]. Liver fibrosis has been shown to start decreasing 1 year after surgery and continued to improve until 5 years postoperatively [35]. Bariatric surgery can also promote improvement/remission of several comorbid conditions that are associated to NAFLD (such as prediabetes, T2D, obstructive sleep apnea (OSA) and polycystic ovary syndrome (PCOS)) [36–38]. However, recent evidence from 7391 Roux-en-Y gastric bypass and 5872 sleeve gastrectomy individuals showed that at least one in six individuals experienced 10% weight gain or more after surgery [39]. Hence, combining non-pharmaceutical strategies with pharmacological therapies is crucial, to prevent the evolution of NASH to cirrhosis and its future devastating sequelae.
In the most recent American Association of Clinical Endocrinology clinical practice guidelines for the diagnosis and management of NAFLD it was recommended to administer pioglitazone (PIO) or glucagon-like peptide 1 receptor (GLP-1R) agonists with proven benefit for patients with T2D and biopsy-proven NASH, while these medications should be considered when there is high probability of having NASH (based on higher plasma aminotransferase levels and non-invasive tests) [40]. Furthermore, it was stated that clinicians must consider treating patients with T2D and NAFLD with PIO, GLP-1R agonists or sodium-glucose co-transporters 2 (SGLT2) inhibitors to reduce their significant cardiovascular risk. Early diagnosis and treatment of obesity, hypertension and dyslipidemia were also stated to be of major importance in this population. In the recent European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO) clinical practice guidelines on the management of MASLD it was also stated that PIO can be used safely in individuals with non-cirrhotic MASH [6]. GLP-1R agonists cannot be currently recommended as targeted approaches for MASH but should be administered for their indications (T2D, obesity); SGLT2 inhibitors cannot be also currently recommended as MASH-targeted therapy but should be used for their respective indications (T2D, chronic heart failure (CHF) and chronic kidney disease (CKD)) [4].
The complex pathophysiology, which underlies the pathogenesis of NAFLD emphasizes the need for combination treatment strategies with different drug classes that target different cellular pathways. Combination therapies could be particularly important to face the evolution and progression of NAFLD, since no single agent can control all the mechanisms driving its development [41–43]. This review explores thoroughly the combinations of PIO with either GLP-1R agonists or SGLT2 inhibitors in individuals with NAFLD and discusses their future role in this setting. Since in all of the above studies the terminologies NAFLD/NASH were applied, these definitions will be used in this review.
PIO, GLP-1R agonists, SGLT2 inhibitors and NAFLD: pathophysiological background
PIO
PIO, currently the only thiazolidinedione (TZD) in clinical practice, is a potent exogenous agonist of the nuclear peroxisome proliferator-activated receptor-gamma (PPAR-γ) and to a lesser extent, PPAR-α [17, 44]. It is the only true insulin sensitizing antidiabetic drug in our therapeutic armamentarium for the treatment of patients with T2D [17, 44, 45]. It augments the effects of insulin on its cellular targets (especially in the adipose tissue) and has shown cardiovascular benefits in randomized controlled trials (RCTs), meta-analyses of several prospective studies and large observational studies [45, 46]. It has achieved β-cell function preservation, meaningful reduction of albuminuria and significant improvements of several components of the MS [46, 47].
Since IR governs the pathogenesis of NAFLD, the possible role of PIO in this setting gained special interest during the last two decades. PIO was the first antihyperglycemic medication that demonstrated beneficial liver effects in a small RCT, which analyzed data from 55 individuals with prediabetes/diabetes and biopsy-proven NASH [48]. Since then, several RCTs and meta-analyses have shown beneficial histological improvements after the administration of PIO in individuals with overweight/obesity, prediabetes and T2D who experience NASH; some studies suggested improvements in liver fibrosis of any stage [49–53]. In one meta-analysis PIO was found to be the most effective drug for the treatment of NASH followed by Roux-en-Y gastric bypass procedure [53]. Interestingly, a subgroup analysis of the Thiazolidinediones Or Sulfonylureas Cardiovascular Accidents Intervention Trial (TOSCA.IT) suggested that even low doses of PIO can significantly improve liver steatosis and inflammation in patients with T2D independently of its blood glucose lowering effect [54]. Current international practice guidelines recommend PIO as a promising therapy for patients who experience NASH and T2D [6, 40, 55, 56].
PIO can: (i) promote adipocyte differentiation with the predominance of insulin-sensitive small adipocytes, which correlates with insulin sensitivity; (ii) suppress lipolysis from visceral adipose tissue; (iii) upregulate fatty acid translocase, which is the enzyme that moves circulating NEFAs into adipocytes, so less NEFAs are available for infiltration into the liver; (iv) promote diversion of fat storage from hepatocytes to adipocytes through the stimulation of PPAR-γ in adipose tissue; (v) stimulate NEFAs oxidation in hepatocytes; (vi) downregulate de novo lipogenesis after suppressing hyperinsulinemia; (vii) reduce the production/secretion of tumor necrosis factor alpha (TNF-α), interleukin-6 (IL-6), monocyte chemoattractant protein-1 (MCP-1/CCL2), plasminogen activator inhibitor type 1 (PAI-1), transforming growth factor beta-1 (TGF-β1) and angiotensinogen, while it can stimulate the secretion/activity of adiponectin; (viii) improve mitochondrial dysfunction that has been associated with IR and (ix) achieve β-cell function preservation (both in patients with T2D and individuals with prediabetes) and suppress excess intra-pancreatic fat deposition [44, 45, 57–64] (Figure 1). In contrast to PIO, rosiglitazone was not shown to promote histologic improvements of NASH during a 12-month well-organized study [65].
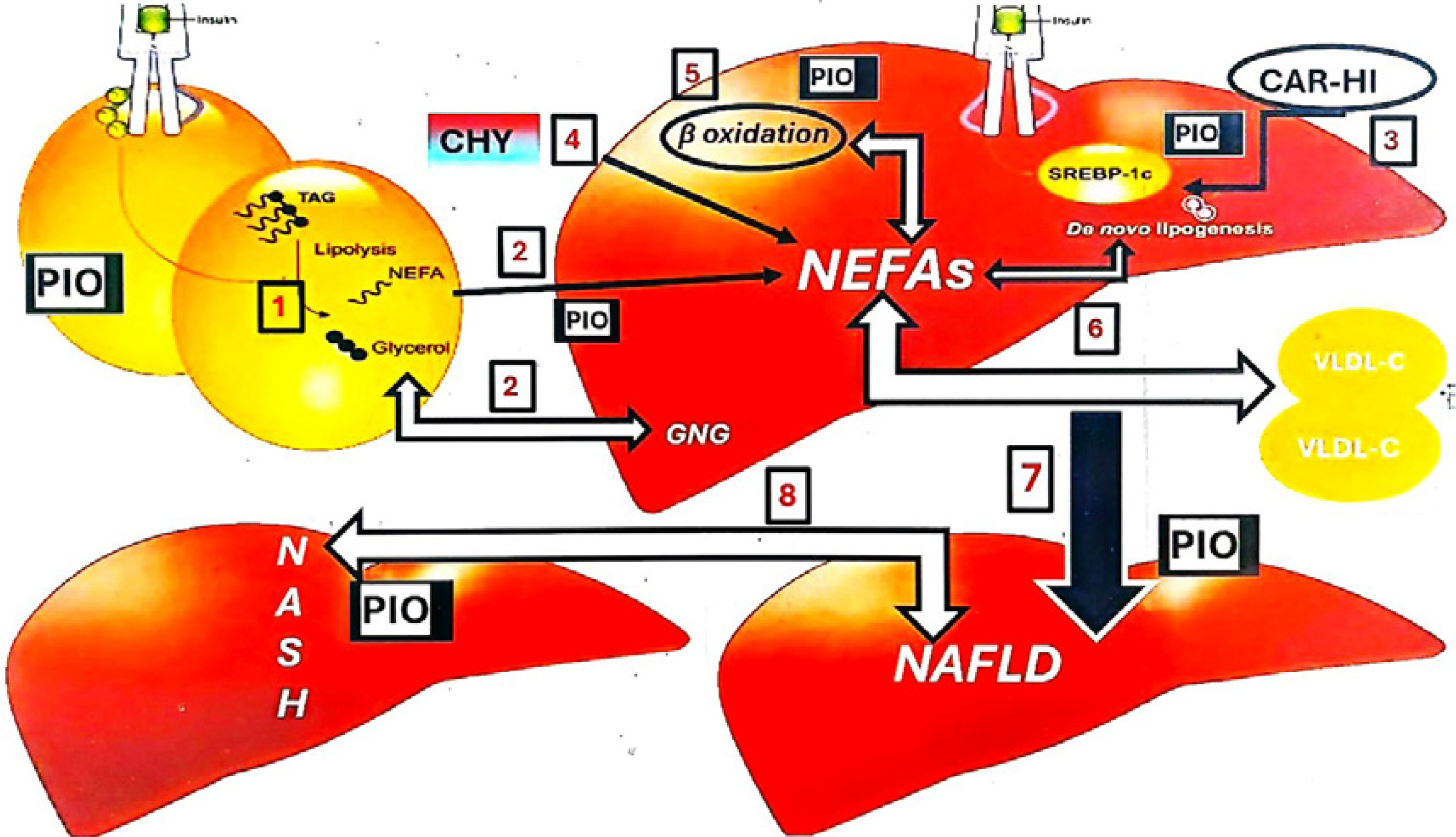
Figure 1
NAFLD: pathophysiological background and the intrahepatic activity of PIO. Increased levels of NEFAs in the liver are mainly the result of: 1. Stimulated lipolysis from visceral fat since hormone-sensitive lipase cannot be sufficiently downregulated during an insulin resistant state 2. Higher amounts of NEFAs are delivered from visceral fat into the hepatocytes, while glycerol is used as a main substrate for hepatic GNG 3. De novo lipogenesis from excess CAR (glucose and fructose). This is achieved after the activation of SREBP-1c that is extremely sensitive to HI 4. The metabolism of intestinal CHY that penetrate the liver through the portal system. After entering the liver NEFAs: 5. Can be transported into the mitochondria and metabolized through β-oxidation 6. Can be converted to neutral TAG, packaged into VLDL-C particles and secreted into the circulation 7. When these cellular pathways are overwhelmed and hepatic lipid storage overcomes lipid clearance and utilization, excess intrahepatic TAG levels can form cytosolic intracellular fat droplets and eventually steatosis 8. Several mechanisms including altered secretion of adipokines/cytokines, hepatokines, stimulation of multiple inflammatory pathways, endoplasmic reticulum stress, increased oxidative stress (in a complex interplay with genetic predisposition) drive the evolution of inflammation, hepatocellular injury and fibrosis promoting NASH. PIO can: (i) suppress lipolysis from visceral adipose tissue; (ii) upregulate fatty acid translocase, which is the enzyme that moves circulating NEFAs into adipocytes, so less NEFAs are available for infiltration into the liver; (iii) promote diversion of fat storage from hepatocytes to adipocytes; (iv) stimulate NEFAs oxidation in hepatocytes; (v) downregulate de novo lipogenesis after suppressing HI; (vi) reduce the production/secretion of several adipokines/cytokines that promote inflammation and (vii) stimulate the secretion/activity of adiponectin.
PIO – pioglitazone, NAFLD – non-alcoholic fatty liver disease, NASH – non-alcoholic steatohepatitis, NEFAs – non-esterified fatty acids, GNG – gluconeogenesis, SREBP-1c – sterol regulatory element-binding protein 1c, HI – hyperinsulinemia, CAR – carbohydrates, CHY – chylomicrons, TAG – triglycerides, VLDL-C – very-low-density lipoprotein cholesterol.
GLP-1R agonists
The administration of GLP-1R agonists in patients with T2D has achieved significantly lower hemoglobin A1C (A1C) levels and promoted remarkable weight loss and significant cardiometabolic improvements [66]. Abdominal fat loss, as well as sustained reductions of fasting insulin levels and markers of IR, have been also shown to individuals with overweight/obesity, prediabetes, PCOS and OSA during their administration [31, 38, 67–70]. Liraglutide (LIRA) and semaglutide (SEMA) gained approval by the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for weight reduction in obese individuals or people who are overweight with BMI ≥ 27 kg/m2 and also experience at least one weight-associated comorbid situation (such as hypertension, dyslipidemia, prediabetes and OSA) combined to lifestyle modifications [71]. SEMA has also been approved from FDA for treating obesity in pediatric patients aged 12 years and older [72]. SEMA was shown to be the most effective of its category in terms of meaningful weight reduction as it can penetrate certain areas in the central nervous system that are critical for hunger and appetite control and are not protected by the blood-brain barrier, regulating key appetite-modulating relay areas [70, 73].
The administration of GLP-1R agonists to individuals with NAFLD reduced liver fat content, normalized plasma aminotransferase levels and promoted histological improvements in terms of hepatocellular inflammation, preventing fibrosis progression [74–78]. However, the absence of statistically significant effects of GLP-1R agonists, with respect to at least one fibrosis stage histological improvement without worsening of NASH, could be the result of: (i) the insufficient duration of the current studies; (ii) the insufficient power to detect any association; (iii) the heterogeneity of study populations and (iv) the different methodologies applied [74, 75]. Moreover, it is not possible to clarify whether these effects are fully secondary to weight reduction and if this drug class has other beneficial hepatocellular activities beyond weight loss. Preclinical evidence has suggested that GLP-1R agonists can suppress hepatocellular inflammation and increased oxidative stress indirectly through several cellular pathways that are, in part, independent of weight reduction, since hepatocytes, Kupffer cells, and stellate cells do not express GLP-1Rs [79–85]. They can also: (i) improve the composition of gut microbiota; (ii) suppress hepatic de novo lipogenesis; (iii) decrease enterocyte chylomicron production/secretion and (iv) promote β-oxidation of NEFAs inside the hepatocytes [79, 81, 82, 86]. A recent network meta-analysis suggested that GLP-1R agonists were associated with significantly greater activity in decreasing liver fat content and improving cardiometabolic risk parameters in overweight or obese patients with NAFLD vs. PIO. However, no statistical significance was found as far as liver biopsy-based outcomes were concerned [87].
SGLT2 inhibitors
SGLT2 inhibitors can achieve about 50% reduction of tubular maximum renal glucose reabsorptive capacity and consequently they can promote significant glycosuria [88–90]. They have achieved median A1c reductions of 0.6–0.8% in patients with T2D and normal renal function, while higher improvements have been demonstrated in patients who experienced baseline A1c levels ≥ 10% [88–90]. SGLT2 inhibitors have shown salutary cardiovascular and renal benefits in patients with T2D and signified a new era, in which antidiabetic therapies should be based on end-organ protection and patient comorbidities, rather than aiming only on decreasing blood glucose concentration [88–91]. Their cardiovascular and renal benefits were also shown in non-diabetic population with CKD and/or CHF [92].
Both preclinical and clinical studies have consistently demonstrated significant body weight reduction (significant loss of 240–320 calories/daily resulting in average weight loss of 2–4 kg during the first 24 weeks) after their administration. Systolic blood pressure (BP) levels were also decreased after their administration [89, 93]. Through increased NEFAs oxidation and ketogenesis SGLT2 inhibitors can reduce visceral adipose tissue and liver steatosis; enhanced lipolysis and visceral fat loss (reaching up to 70% of total weight reduction) have been reported in most of the current literature [89, 93–95]. Moreover, several studies suggested that this drug class possesses significant anti-inflammatory and anti-oxidative stress properties [38, 88, 92]. The beneficial effects of SGLT2 inhibitors on metabolic outcomes (BP control, body weight) were also shown in a meta-analysis of RCTs in non-diabetic individuals [96].
Several small, open-label studies, systematic reviews and meta-analyses of these studies have demonstrated that SGLT2 inhibitors significantly decreased hepatic steatosis and improved liver biochemistry in patients with T2D [97–101]. A recent prospective study, which analyzed data from 237 patients with T2D, followed by nearly 5 years with elastography, suggested that SGLT2 inhibitors reduced the risk of worsening liver stiffness [102]. Few small RCTs suggested histological improvements in terms of hepatocellular inflammation (especially ballooning) and beneficial effects on liver fibrosis [103–106]. Possible mechanisms for their beneficial effects in individuals with NAFLD are: (i) reduction of visceral adipose tissue and thus IR; (ii) stimulation of adiponectin levels; (iii) improvement of mitochondrial function/oxidative capacity; (iv) suppression of high oxidative stress and systemic inflammation; (v) promotion of autophagy; (vi) reduction of endoplasmic reticulum stress; (vii) inhibition of hepatic apoptosis; (viii) suppression of de novo lipogenesis after decreasing fatty acid synthase and acetyl-CoA carboxylase 1 expression and (ix) reduction of insulin/glucagon ratio that results in almost 25% restriction of glucose utilization and enhanced ketogenesis. Higher β-hydroxybutyrate levels can deactivate the nucleotide-binding oligomerization domain (NOD)-like receptor family pyrin domain containing 3 (NLRP3) inflammasome pathway in neutrophils and monocytes/macrophages; hence they can subsequently reduce the production of downstream inflammatory cytokines and chemokines inside the liver [88, 89, 107–112].
Combination of PIO with SLGT2 inhibitors
Preclinical evidence
The possible activities of ipragliflozin (IPRA), PIO or their combination on a variety of diabetic features (IR, hyperinsulinemia, obesity, dyslipidemia) and the progression to NASH were explored after their administration to high-fat diet-fed KK/Ay T2D mice [113]. Specifically IPRA (0.1–3 mg/kg), PIO (3–30 mg/kg), IPRA (1 mg/kg) combined with PIO (10 mg/kg), or a vehicle were given orally to diabetic mice with NASH for 4 weeks. IPRA stimulated urinary glucose excretion and reduced significantly total body and visceral fat weights without any meaningful effects on food consumption. PIO increased both body and visceral fat without affecting food consumption and also reduced urinary glucose excretion through suppression of glucosuria. Combination therapy showed additive effects on suppressing non-fasting blood glucose levels, plasma insulin levels, A1C levels and lipid parameters. Body and visceral fat weights were significantly reduced without effects on food consumption. The administration of IPRA significantly decreased hepatic lipid concentrations and plasma levels of ALT/AST in a dose-dependent fashion. PIO also improved steatohepatitis indices. The combination of PIO with IPRA showed synergistic effects in suppressing these parameters. IPRA and PIO significantly improved hepatocellular hypertrophy, micro-vesicular steatosis, lobular inflammation and mild fibrosis in a dose-dependent manner, with the activities of PIO being weaker compared to those of IPRA. Combination therapy significantly and additively improved all these liver defects. PIO and IPRA also improved several markers of inflammation and oxidative stress in a dose-dependent manner, while combination therapy significantly and additively reduced these parameters. Furthermore, the combination of these two medications in T2D diabetic mice with NASH suppressed PIO-induced fluid retention through IPRA-induced osmotic diuresis [114].
An interesting preclinical study explored the activity of PIO, metformin (MET) and dapagliflozin (DAPA) individually and in combinations vs. silymarin in 5-week-old male Wistar rats, starting at the third week of NAFLD induction and continued for another 3 weeks. The experimental arm consisted of rats that consumed atherogenic diet, which promoted the evolution of NAFLD, as well as several other metabolic alterations (including dyslipidemia, systemic inflammation, increased oxidative stress and IR) [115]. Rats fed with high-fat atherogenic diet experienced higher hepatic mass (as indicated by an elevated liver index), which was independent of their body weight vs. control rats fed with standard chow. All combination groups that included DAPA achieved suppression of this effect. Significant histological liver improvements (including marked tissue regeneration, normal portal tracts and less hepatic ballooning) were found in all treatment groups. The least protective impact was shown when rats were treated with MET monotherapy. Combination therapies were shown to have stronger benefits regarding most of the measured parameters [including abnormalities in aspartate aminotransferase (AST) and alanine aminotransferase (ALT) concentrations, markers of systemic inflammation (clear reductions of IL-1β levels), liver inflammation, hepatocellular oxidative stress, hepatic fibrosis and hepatocyte apoptosis] vs. monotherapy arms. Interestingly, the combination of PIO with DAPA showed the biggest reductions of hepatic tissue inhibitor of metalloproteinase 1 (TIMP-1) concentrations.
Clinical evidence
The effectiveness of combination therapy with PIO (15–30 mg daily) and tofogliflozin (TOFO – 20 mg daily) for 24 weeks was investigated in 32 patients who experienced T2D and NAFLD in an open-label RCT [116]. This study was part of the ToPiND trial that explored the activities of PIO and TOFO in 40 patients with T2D and NAFLD [117]. In that study it was shown that both PIO and TOFO for 24 weeks significantly improved hepatic steatosis based on the absolute change in MRI-proton density fat fraction (MRI-PDFF), as well as ALT levels, with the differences being statistically insignificant between the two drugs. However only PIO significantly improved MR elastography-liver stiffness (MRE-LSM), whereas TOFO did not, suggesting that PIO could be more effective in improving liver fibrosis [117]. The combination was administered after the 24th week of monotherapy completion in patients who experienced A1c levels of at least 6% (6.5% or higher for patients aged 65 years or more who were treated with sulfonylurea). Combination treatment 24 weeks after monotherapy improved MRI-PDFF vs. baseline values (–5.98 ±4.70%, p < 0.0001). Specifically, when TOFO was administered as the first-line therapy and PIO was subsequently added, the combination showed significant additional improvements of MRI-PDFF and ALT concentrations vs. monotherapy with TOFO. When TOFO was added on top of PIO, the improvement of MRI-PDFF was insignificant (–0.42%). Combination therapy of TOFO with PIO showed significant reduction in MRE-LSM vs. monotherapy. Type IV collagen 7S concentration showed no significant improvement after monotherapy with either TOFO or PIO. However, it was significantly improved during the combination therapy (p = 0.0193). Combination of PIO with TOFO also suppressed oxidative stress (urinary 8-hydroxydeoxyguanosine) and cytokeratin-18 fragments (molecules that are essentially involved in the pathogenesis of NASH) vs. monotherapies [118, 119]. Interestingly, the combination therapy suppressed PIO-induced gain effect, in concordance to preclinical evidence. The main limitations of this study were its small size and short duration, as well as its open-label design.
A double-blind multicenter placebo-controlled RCT was organized in 249 patients with T2D suboptimally treated with the combination of MET and DAPA [120]. They were randomized to receive either PIO (in a daily dose of 15 mg) or placebo for 24 weeks, followed by a 24-week PIO extension for those who had completed the main study. Reductions of AST, ALT and γ-glutamyl transferase (γ-GT) were found in the PIO arm although the between-arm difference was only significant for γ-GT (p = 0.024). NAFLD liver fat score was reduced only in the PIO arm (p < 0.001), promoting a significant between-group difference (p = 0.006). No significant differences were shown for fatty liver index (FLI) or hepatic steatosis index (HIS) in either group at 24 weeks of therapy. A possible explanation for this finding could be the inclusion of BMI and/or waist circumference in estimating these surrogate markers of hepatic steatosis, which were increased in the PIO arm. The possible role of combined PIO and empagliflozin (EMPA) therapy vs. monotherapy with each medication in patients with T2D and NAFLD is currently under intense investigation [121–123].
Combination of PIO with GLP-1R agonists
The possible role of exenatide (EXE) and PIO combination therapy on hepatic fat content was investigated in 21 patients with T2D being on diet (n = 4) and/or MET therapy for at least 3 months (n = 17) [124]. Specifically, patients were randomized in an open-label fashion to receive either: (i) PIO 30 mg/day for 2 weeks followed by PIO 45 mg/day for 50 weeks (n = 10) or (ii) EXE 5 µg twice daily and PIO 30 mg/day for 2 weeks followed by EXE 10 µg twice daily and PIO 45 mg/day for 50 weeks (n = 11). Both arms experienced similar liver fat content, which was estimated with magnetic resonance spectroscopy (MRS). PIO administration suppressed hepatic fat content (11.0 ±3.1 to 6.5 ±1.9%, p < 0.05) after 12 months of therapy. After combination treatment hepatic fat content was reduced significantly (12.1 ±1.7 to 4.7 ±1.3%, p < 0.001). The reduction in hepatic fat content was significantly higher in the combination arm vs. the monotherapy arm (Δ = 61% vs. 41%, p < 0.05). Liver transaminases were significantly reduced after 12 months of PIO therapy, as well as after combination therapy. Combination therapy was related to higher reduction of ALT (p < 0.05) vs. monotherapy with PIO. Plasma adiponectin concentration was significantly higher after 12 months of PIO administration (8.5 ±0.8 to 15.8 ±1.4 µg/ml, p < 0.001). Following combination treatment for 12 months, plasma adiponectin concentration increased almost threefold (7.9 ±0.9 to 23.2 ±2.7 µg/ml, p < 0.001). Combination treatment was related to higher increase in plasma adiponectin (86% vs. 193%, p < 0.001). Combining EXE with PIO also suppressed the significant change in body weight induced by PIO compared to weight gain found after its administration. The higher reduction in hepatic fat content in the combination arm (without a significant change in body weight) vs. monotherapy with PIO suggested that EXE/PIO combination may exert additional therapeutic benefits in treating NAFLD beyond weight loss. Furthermore, it has shown greater reduction of plasma TGs in the combination arm vs. PIO monotherapy (Δ = 38% vs. 14%, p < 0.01), which was noteworthy since baseline TGs were significantly lower in those patients receiving combination treatment (136 ±13 mg/dl vs. 192 ±25 mg/dl). Fasting plasma concentration of fibroblast growth factor 21 (FGF21), which has been recently recognized as a possible molecule for the treatment of NAFLD, was not altered after 12 months of PIO administration despite its effect in decreasing hepatic fat content [125, 126]. However, combination therapy promoted significant decline in fasting plasma FGF21 after 12 months of treatment (p < 0.01), possibly a sign of improved FGF21 resistance in hepatocytes [126].
EDICT (Efficacy and Durability of Initial Combination Therapy) was initially a 3-year (extended to 6 years) trial that investigated the activity of triple combination therapy (MET/PIO/EXE) vs. conventional stepwise treatment (MET/glipizide/insulin) on glycemic control of recently diagnosed patients with T2D [127]. Sixty-eight patients (n = 29 in the triple arm vs. n = 39 in the conventional arm) who completed 5.4 years of median follow-up underwent vibration-controlled transient elastography (FibroScan) to provide evidence of steatosis (controlled attenuation parameter (CAP)) and fibrosis [liver stiffness measurement (LSM)], while 42 participants (25 in conventional and 17 in triple therapy arms) eventually underwent MRI-PDFF to estimate liver fat content [128]. Several fibrosis scores were estimated such as AST/ALT ratio, fibrosis-4 (FIB-4) index, AST to platelet ratio index (APRI) and NAFLD fibrosis score (NFS). A1c levels at the end of the study were 6% vs. 6.8% in the triple therapy and conventional therapy arms respectively (p = 0.0006). Change in body weight between the two treatment groups at the end of the study was insignificant. Both plasma AST and ALT concentrations were significantly reduced in patients receiving the triple therapy (p < 0.01). However, in the conventional arm ALT significantly increased and AST remained unchanged. When separated into tertiles of AST and ALT, triple therapy promoted significant reductions in ALT and AST compared to baseline and conventional therapy; in the conventional group no changes were observed in any of the three baseline tertiles. At the end of the trial patients who were treated with conventional treatment experienced more hepatic steatosis and fibrosis vs. those receiving triple therapy. Specifically, 69% of the patients in the conventional arm experienced grade 2/3 steatosis vs. 31% in the triple therapy group (p = 0.003), while 26% of participants in the conventional arm had stage 3/4 fibrosis vs. 7% in the triple therapy arm (p = 0.04). Median CAP indices were 311 and 284 (p = 0.04) and the median LSM scores were 7.8 and 5.8 (p = 0.02) in patients treated with conventional and triple therapy, respectively. Patients in the conventional therapy group experienced significantly higher liver fat content vs. those enrolled in the triple therapy group (p = 0.03). LSM values were also significantly associated to liver fat content measured with MRI-PDFF. In the entire cohort (triple and conventional arms) the severity of CAP (p < 0.001) and LSM (p < 0.001) were strongly and inversely related to the Matsuda Index of insulin sensitivity, but not with the percentage of body fat. Improved insulin sensitivity and lower BMI values were related to lower rates of steatosis and fibrosis. Lower plasma AST and ALT concentrations were the only parameters associated to the severity of steatosis and fibrosis at the end of the study, while changes in liver fibrosis scores (APRI, NFS, FIB-4, and AST/ALT ratio) showed limited value in predicting response to therapy. Although glycemic control in the conventional treatment arm was quite good (A1C: 6.8%) but not as good as with triple therapy (A1C: 6%) and the prevalence of hepatic fibrosis and steatosis was markedly higher in the former, it was stated that improved glycemic control with triple therapy was unlikely to exert significant roles in the beneficial liver effects of this combination. Lack of baseline measurements for liver steatosis and fibrosis before the initiation of the EDICT study, as well as the small number of patients enrolled were the main limitations of this trial. The main results of the combinations of PIO with either GLP-1R agonists or SGLT2 inhibitors in patients with T2D and NAFLD are shown in Table I.
Table I
Combinations of PIO with either GLP-1R agonists or SGLT2 inhibitors in patients with type diabetes mellitus and nonalcoholic fatty liver disease: main results
| Authors [ref.]/year | Study population | Study design | Major results |
|---|---|---|---|
| Yoneda et al. [116]/2022 | 32 patients with T2D and NAFLD | The effectiveness of combination therapy with PIO (15–30 mg daily) and TOFO (20 mg daily) for 24 weeks was investigated. This study was part of the ToPiND study that explored the activities of PIO vs. TOFO in 40 patients with T2D and NAFLD for 24 weeks. The combination was administered after the 24th week of monotherapy completion in patients who experienced A1C levels of at least 6% (6.5% or higher for patients at least 65 years old who were treated with SUL). | Combination therapy showed an improvement of MRI-PDFF of –5.98 ±4.70% from baseline (p < 0.0001). Specifically, when TOFO was administered as the first-line therapy and PIO was subsequently added, the combination showed significant additional improvement of MRI-PDFF and ALT levels vs. monotherapy with TOFO. Combination therapy of TOFO with PIO showed significant reduction in MRE-LSM vs. monotherapy with TOFO. |
| Lim et al. [120]/2024 | 249 patients with T2D suboptimally treated with MET and DAPA | Double-blind multicenter placebo-controlled RCT in which participants were randomized to receive either PIO in a daily dose of 15 mg or placebo for 24 weeks, followed by a 24-week PIO extension for those who had completed the main study. | PIO promoted reduction of AST, ALT and γ-GT levels although the between-arm difference was only significant for γ-GT (p = 0.024). NAFLD liver fat score was reduced inly in the PIO arm (p < 0.001), promoting a significant between-group difference (p = 0.006). |
| Sathyanarayana et al. [124]/2011 | 21 patients with T2D being on diet (n = 4) and/or MET therapy for at least 3 months (n = 17) | Patients were randomized in an open label fashion to receive either: (i) PIO 30 mg/day orally for 2 weeks followed by PIO 45 mg/day orally for 50 weeks (n = 10) or (ii) EXE 5 µg subcutaneously twice daily and PIO 30 mg/day orally for 2 weeks followed by EXE 10 µg twice daily and PIO 45 mg/day orally for 50 weeks (n = 11). | The reduction in hepatic fat content was significantly higher in the combination arm vs. the monotherapy arm (Δ = 61% vs. 41%, p < 0.05). Combination therapy was related to higher reduction of ALT (p < 0.05) vs. monotherapy with PIO. Combination treatment was related to higher increase in plasma adiponectin levels (86% vs. 193%, p < 0.001). The higher reduction in hepatic fat content without significant change in body weight in the combination arm vs. monotherapy with PIO (96.8 ±7.3 vs. 95.7 ±5.1 kg) suggested that combined EXE and PIO therapy probably exerts additional therapeutic benefits in treating NAFLD beyond weight loss after GLP-1R agonist therapy. |
| Lavynenko et al. [128]/2022 | Sixty-eight patients recently diagnosed with T2D | EDICT was initially a 3-year trial (extended to 6 years) that investigated the activity of triple combination therapy (MET/PIO/EXE) vs. conventional stepwise treatment (MET/glipizide/insulin). Sixty-eight patients (n = 29 in the triple arm vs. n = 39 in the conventional arm) who completed 5.4 years of follow-up experienced a vibration-controlled transient elastography to provide evidence of steatosis (CAP) and fibrosis (LSM), while 42 participants (25 in conventional and 17 in triple therapy arms) eventually experienced MRI-PDFF to estimate liver fat content. | Change in body weight between the two treatment groups at the end of the study was insignificant. At the end of the trial 69% of the patients in the conventional arm experienced grade 2/3 steatosis vs. 31% in triple therapy (p = 0.003), while 26% of participants in the conventional arm had stage 3/4 fibrosis vs. 7% in the triple therapy arm (p = 0.04). Patients in the conventional therapy group experienced significantly higher liver fat content versus those enrolled in the triple therapy group (p = 0.03). In the entire cohort (triple and conventional arms) the severity of CAP (p < 0.001) and LSM (p < 0.001) were strongly and inversely related to the Matsuda Index of insulin sensitivity, but not with percentage body fat. Improved insulin sensitivity and lower BMI values were related to lower rates of steatosis and fibrosis. |
[i] PIO – pioglitazone, GLP-1R – glucagon-like peptide 1 receptor, SGLT2 – sodium-glucose co-transporters 2, TOFO – tofogliflozin, SUL – sulfonylurea, MET – metformin, DAPA – dapagliflozin, EXE – exenatide, NAFLD – non-alcoholic fatty liver disease, T2D – type 2 diabetes, A1C – glycated hemoglobin, ALT – alanine aminotransferase, AST – aspartate aminotransferase, γ-GT – gamma-glutamyl transferase, MRI-PDFF – MRI-proton density fat fraction, MRE-LSM – MR elastography-liver stiffness, RCT – randomized controlled trial, EDICT – Efficacy and Durability of Initial Combination Therapy, CAP – controlled attenuation parameter, LSM – liver stiffness measurement, BMI – body mass index.
Conclusions
Over the last three decades, NAFLD has emerged as one of the leading causes of cirrhosis worldwide and an increasingly important health issue; its presence amplifies the risk of T2D incident by approximately twofold [1, 6, 9, 129–131]. Current evidence suggests that no more than 40% of individuals with NAFLD will benefit from a single therapy, emphasizing the urgent need for combination therapies. These therapies must not be antagonistic and ideally should exert synergist effects targeting concomitant abnormal cellular and molecular pathways that drive its pathogenesis (thereby expanding the biological response) and prevent compensatory pathways that can reduce the efficacy of a single drug [6, 9, 132]. Hence, it seems reasonable for patients with T2D and NASH to combine medications that beyond their antihyperglycemic activities, can synergistically contribute to the improvement and/or resolution of liver pathology and simultaneously exert salutary cardiovascular and kidney benefits [41–43]. To bridge this gap, many clinical trials have been published and others are ongoing with promising results [43, 133–135]. Moreover, the recent dual GIP/GLP-1 receptor agonist tirzepatide promoted greater decrease of liver fat content and of the volume of visceral adipose tissue vs. insulin degludec and was found to be more effective vs. placebo with respect to resolution of MASH without worsening of fibrosis [136, 137]. Liver-targeting medications (such as resmetirom, fibroblast growth factor 21 analogs and lanifibranor), aiming at liver inflammation and collagen deposition, are expected to become crucial in individuals with more advanced liver disease [138].
In one of the longest published studies until today (with a follow-up of 6 years) it was clearly shown that in patients with T2D and NAFLD the severity of both steatosis and fibrosis were strongly and inversely related to the Matsuda Index of insulin sensitivity, emphasizing the crucial role of PIO (currently the most well-studied TZD) that targets IR directly to its genesis [128]. Indeed, two decades ago Reaven stated that although compensatory hyperinsulinemia may prevent the evolution of fasting hyperglycemia in individuals with IR, the price paid is NAFLD and the relevant atherogenic lipoprotein profile, which characterizes this population [139].
Preclinical models of NAFLD have shown interesting and additive beneficial effects when PIO was combined with SGLT2 inhibitors, with less PIO-induced weight gain and fluid retention. When PIO was added on top of an SGLT2 inhibitor in patients with T2D and NAFLD it promoted significant improvements of liver function tests, as well as non-invasive quantitative biomarkers that estimate liver steatosis and fibrosis. The combination of PIO with GLP-1R agonists also demonstrated significant reductions of hepatic fat content, liver indices, as well as markers of inflammation and fibrosis (Table I). Interestingly, both GLP-1R agonists and SGLT2 inhibitors suppressed PIO-induced weight gain to statistically insignificant levels between the comparing groups, suggesting that both drug categories can exert additional beneficial effects in treating NAFLD beyond weight reduction. Reduced body weight after the combination of PIO with either GLP-1R agonists or SGLT2 inhibitors was also verified in a recent systematic review/meta-analysis, as well as an analysis of a large international real-world database [140]. However, it must be stated that any possible beneficial liver effects of both SGLT2 inhibitors and GLP-1R agonists beyond weight loss are awaiting definitive proof in future mechanistic clinical studies [141, 142]. Moreover, their role in the treatment of non-obese or lean individuals with NAFLD (approximately 20% of individuals with NAFLD are lean) requires future investigation [143].
Larger, multiple-arm prospective RCTs including monotherapies with PIO, SGLT2 inhibitors and GLP-1R agonists vs. double and/or triple PIO combinations, in patients with biopsy-proven NASH and T2D (having no contraindications to receive any of these medications) are crucially anticipated. Combination approaches are expected to achieve more robust and durable hepatic effects, as well as significant improvements in hard liver outcomes (including reduced fibrosis progression, evolution to cirrhosis and its complications). The future of NAFLD treatment seems exciting and challenging and has the potential to include more personalized and targeted therapeutic approaches, while issues concerning their safety must be thoroughly recorded and appropriately evaluated [42, 43, 138, 144–146].