Introduction
Peripheral arterial disease (PAD) remains a major cause of morbidity worldwide, with aortoiliac involvement accounting for a substantial proportion of symptomatic cases. Patients commonly present with intermittent claudication in earlier stages, whereas advanced disease may progress to ischaemic rest pain or tissue loss as a result of critically impaired lower-extremity perfusion [1, 2]. Within this spectrum, chronic total occlusion (CTO) of the common iliac artery (CIA) represents one of the most technically demanding manifestations of aortoiliac occlusive disease due to lesion length, severe calcification, and frequent proximity to the aortoiliac bifurcation [3].
Historically, open surgical reconstruction was considered the preferred treatment modality for complex iliac lesions, particularly those classified as TransAtlantic Inter-Society Consensus (TASC) II type C and D [4]. However, advances in endovascular devices, guidewire technology, stent design, and imaging guidance have substantially expanded the role of endovascular therapy in the treatment of iliac artery occlusive disease. Contemporary studies have demonstrated high technical success rates and acceptable mid- to long-term outcomes for endovascular recanalisation of iliac artery CTOs, even in anatomically complex TASC II C–D lesions [5–7]. Accordingly, current European guidelines endorse an endovascular-first strategy as a viable alternative to surgery in selected patients with aortoiliac occlusive disease [8].
Despite these advances, endovascular treatment of unilateral CIA CTOs remains technically challenging, particularly when the occlusion extends close to the aortoiliac bifurcation. Lesion crossing and stent deployment at this level require precise control to avoid suboptimal proximal landing, incomplete lesion coverage, or inadvertent compromise of the contralateral iliac ostium, a recognised complication of iliac interventions [9]. While various antegrade, retrograde, and combined crossing techniques have been described, limited data exist regarding the optimal vascular access strategy for these complex unilateral lesions [10].
From a procedural standpoint, angiographic visualisation during critical steps of lesion crossing and stent deployment is closely linked to access planning. Single-access approaches may provide limited spatial orientation at the level of the bifurcation, whereas bilateral femoral access enables continuous contralateral diagnostic angiography throughout the procedure. This strategy may facilitate accurate identification of the proximal cap, precise stent positioning, and preservation of the aortoiliac bifurcation, thereby enhancing procedural control and safety in anatomically complex cases [9–15]. However, bilateral femoral access has traditionally been reserved as a bailout option rather than adopted as a planned first-line approach, and evidence supporting its routine use in unilateral CIA CTO remains scarce.
Therefore, the aim of the present study was to evaluate the feasibility, technical success, and clinical outcomes of a planned first-line bilateral femoral access strategy for the endovascular treatment of unilateral chronic total occlusion of the common iliac artery, with emphasis on procedural control and bifurcation preservation.
Material and methods
Study design and patient population
This retrospective, single-centre study included consecutive patients with unilateral CTO of the CIA, who underwent endovascular revascularisation using a planned first-line bilateral femoral access strategy between January 2020 and December 2024. Patients with acute occlusion, prior aorto-iliac bypass surgery, or incomplete procedural data were excluded. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Lesion assessment and classification
All lesions were evaluated using pre-procedural digital subtraction angiography. Lesion morphology and complexity were classified according to the TransAtlantic Inter-Society Consensus (TASC II) criteria. Only unilateral CTOs confined to the common iliac artery were included in the analysis.
Endovascular procedure
All procedures were performed via bilateral common femoral artery access. Initial access was obtained on the non-occluded side to allow continuous diagnostic angiography of the aorto-iliac segment and iliac bifurcation. Access on the occluded side was subsequently obtained for lesion crossing using a 0.035-inch hydrophilic guidewire with catheter support.
A planned first-line bilateral femoral access strategy was preferentially adopted in cases with anticipated technical complexity, including CTOs located close to the aorto-iliac bifurcation, suspected ostial involvement, long-segment occlusions, and lesions with severe calcific burden. In such scenarios, continuous contralateral angiographic visualisation was considered essential to optimise stent positioning and preserve the iliac bifurcation.
Following successful guidewire passage, mandatory predilatation was performed in all cases. Stent implantation was subsequently carried out, predominantly using self-expanding stents selected according to vessel diameter and lesion characteristics. During stent deployment, contralateral diagnostic angiography was used to guide accurate positioning, assess stent expansion, and confirm preservation of the iliac bifurcation.
Definitions and study endpoints
Technical success was defined as restoration of antegrade flow with residual stenosis < 30% on final angiography. The primary endpoint was technical success. Secondary endpoints included periprocedural complications (access-site haematoma, flow-limiting dissection, and distal embolisation), symptom recurrence, and radiographic evidence of restenosis or reocclusion.
Follow-up protocol and medical therapy
All patients were followed clinically after the procedure. Duplex ultrasonography and/or computed tomography angiography were performed selectively in patients with recurrent symptoms, in accordance with routine clinical practice.
Following the procedure, all patients received dual antiplatelet therapy consisting of acetylsalicylic acid (100 mg/day) and clopidogrel (75 mg/day). Dual therapy was continued for at least 12 months, followed by lifelong single antiplatelet therapy with acetylsalicylic acid, unless contraindicated.
Statistical analysis
Continuous variables are presented as mean ± standard deviation or median with interquartile range, as appropriate. Categorical variables are expressed as counts and percentages. Given the descriptive nature of the study and the relatively small sample size, no comparative or multivariable analyses were performed.
Results
Patient characteristics
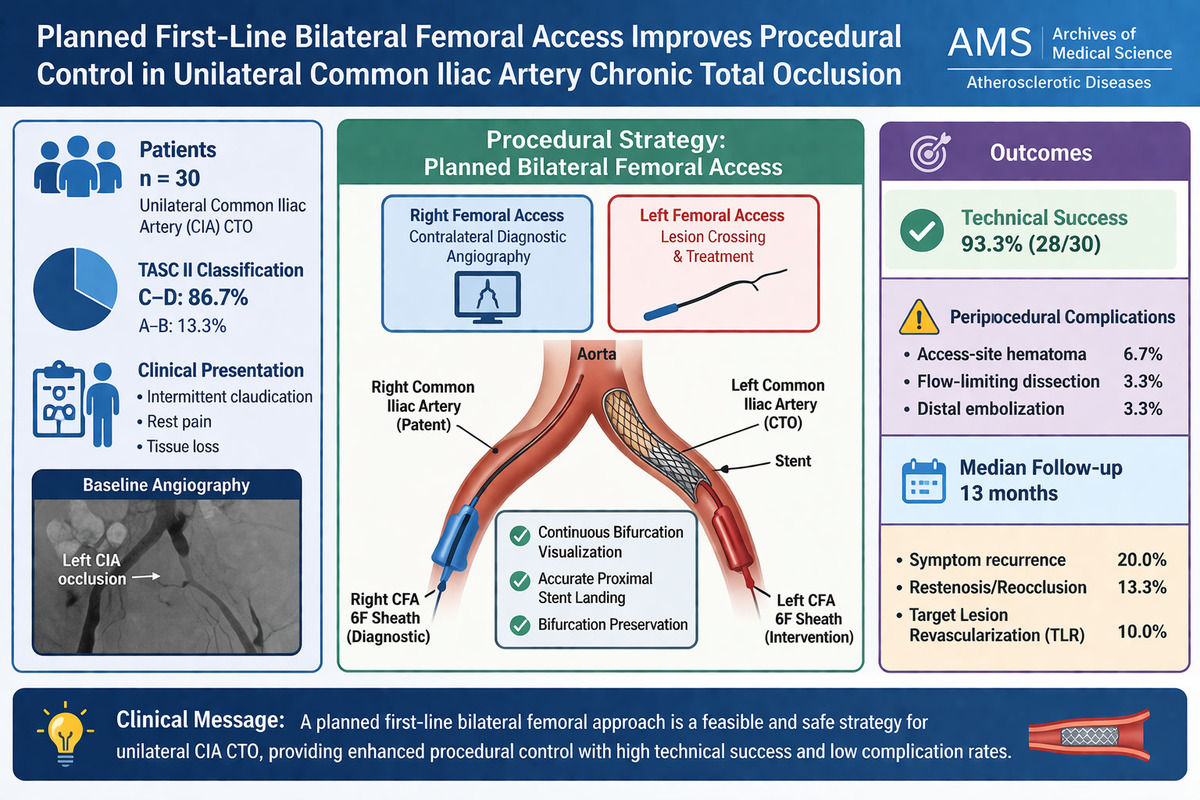
A total of 30 patients with unilateral chronic total occlusion of the CIA were included in the analysis. The mean age was 67.6 ±9.3 years, and most patients were male (73.3%). Hypertension was present in 83.3% of patients, diabetes mellitus in 50.0%, and dyslipidaemia in 70.0%. Clinical presentation consisted of intermittent claudication in 56.7% of patients, ischaemic rest pain in 13.3%, and tissue loss in 30.0%. Baseline demographic and clinical characteristics are summarised in Table I.
Table I
Baseline demographic and clinical characteristics of the study population (n = 30)
Lesion characteristics and procedural details
All target lesions involved the common iliac artery and were classified according to the TASC II criteria. Most lesions were categorised as TASC II C–D (86.7%), with a mean occlusion length of 53.5 ±17.9 mm. Bilateral femoral arterial access was successfully established in all patients. Lesion crossing was achieved using a 0.035-inch hydrophilic guidewire with catheter support, and mandatory predilatation was performed in all cases. Stent implantation was carried out predominantly using self-expanding stents selected according to vessel diameter and lesion morphology. Detailed procedural characteristics are presented in Table II.
Table II
Lesion characteristics, procedural details, and clinical outcomes
Procedural outcomes and technical success
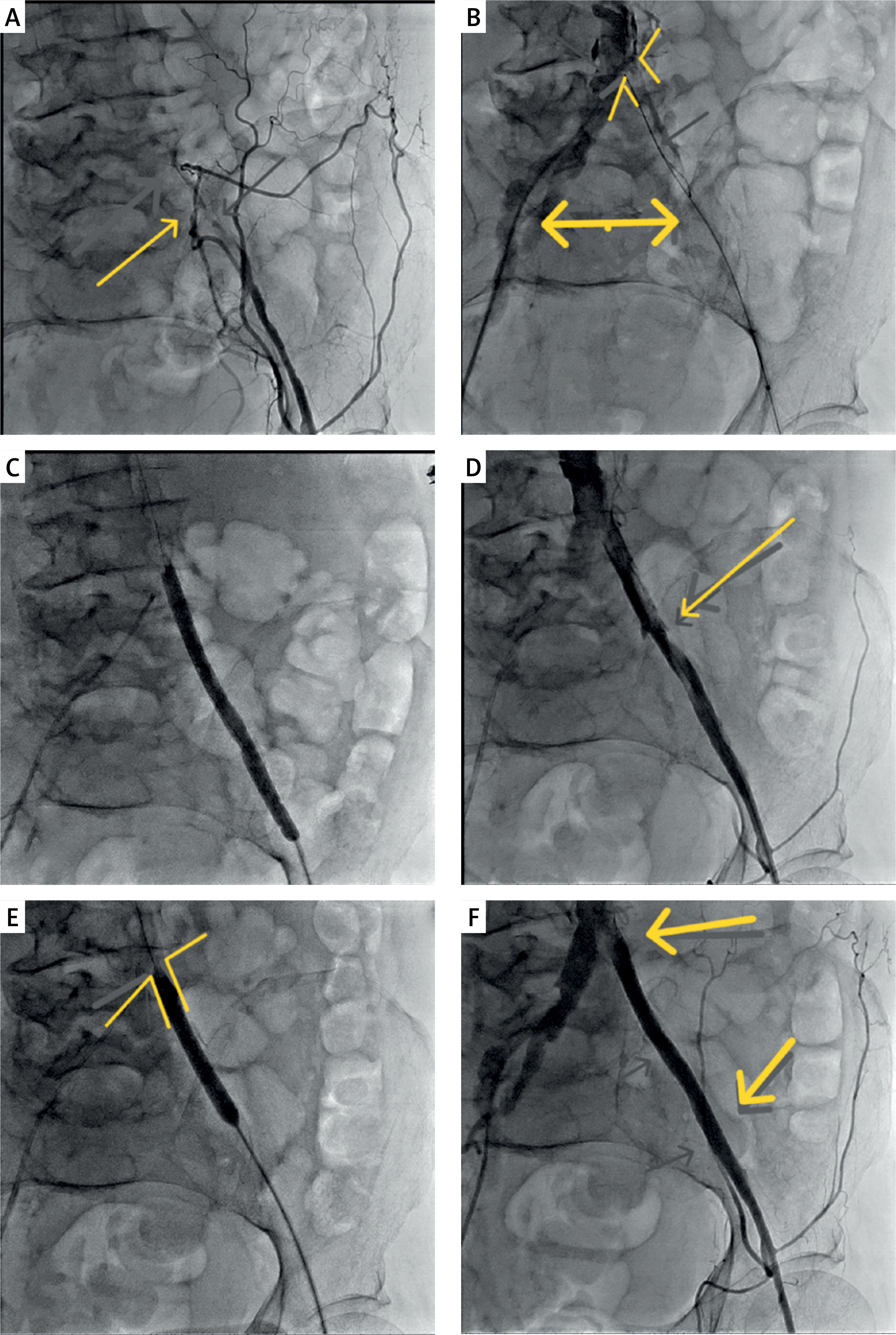
Technical success, defined as restoration of antegrade flow with residual stenosis < 30%, was achieved in 93.3% of patients (28 of 30). The bilateral femoral approach enabled continuous contralateral angiographic guidance during lesion crossing and stent deployment, facilitating accurate stent positioning and preservation of the iliac bifurcation (Figure 1).
Figure 1
Stepwise angiographic depiction of a planned first-line bilateral femoral access strategy for unilateral common iliac artery chronic total occlusion. A – Baseline angiography demonstrating complete occlusion of the left common iliac artery adjacent to the aortoiliac bifurcation. B – Contralateral diagnostic angiography from the right femoral access demonstrates complete occlusion of the left common iliac artery at the level of the aortoiliac bifurcation. The proximal cap of the occlusion and the exact bifurcation line are clearly identified and marked, while lesion crossing is initiated from the ipsilateral side using a 0.035-inch hydrophilic guidewire within the true lumen. C – Initial predilatation of the occluded segment. D – Control angiography after predilatation showing residual stenosis. E – Deployment of a balloon-expandable stent under continuous contralateral angiographic guidance, using the previously marked bifurcation line as a reference to ensure accurate ostial positioning at the iliac bifurcation. F – Final angiography demonstrating restoration of antegrade flow with preserved iliac bifurcation
Periprocedural complications were infrequent. Access-site haematoma occurred in 6.7% of patients and was managed conservatively. Flow-limiting dissection and distal embolisation were each observed in 3.3% of cases. No procedure-related deaths were recorded.
Follow-up and clinical outcomes
The median follow-up duration was 13 months (interquartile range: 10–20 months). Symptom recurrence was observed in 20.0% of patients. In accordance with the follow-up protocol, imaging studies (duplex ultrasonography and/or computed tomography angiography) were performed selectively in symptomatic patients. Restenosis or reocclusion was confirmed in 13.3% of the overall cohort, and target lesion revascularisation was required in 10.0% of patients. Follow-up outcomes are summarised in Table II.
Discussion
The present study demonstrates that a planned first-line bilateral femoral access strategy is a feasible and effective endovascular approach for the treatment of unilateral CTO of the CIA, achieving a high technical success rate with a low incidence of periprocedural complications. Notably, the majority of lesions in this cohort were classified as TASC II C–D, underscoring the applicability of this access strategy in anatomically complex aortoiliac disease [4, 5].
Endovascular recanalisation of iliac artery CTOs has evolved considerably over the past two decades, with contemporary series reporting technical success rates ranging from 85% to 95%, even in extensive and complex lesions [5–7, 11]. The technical success rate of 93.3% observed in the present study is consistent with these reports and supports the feasibility of an endovascular-first approach in selected patients with unilateral CIA CTO. Compared with open surgical reconstruction, endovascular therapy offers reduced perioperative morbidity, shorter hospitalisation, and faster recovery while maintaining acceptable mid-term outcomes [14]. A key contribution of this study is its focus on vascular access strategy as a determinant of procedural control, rather than merely a technical adjunct. Lesion crossing and stent deployment at the level of the aortoiliac bifurcation represent critical steps that may influence both immediate technical success and long-term patency. Inadequate angiographic visualisation during these steps may result in suboptimal proximal stent landing, incomplete lesion coverage, or inadvertent compromise of the contralateral iliac ostium, a recognised complication of iliac interventions [9, 15]. In this context, planned first-line bilateral femoral access functioned as a procedural optimisation strategy by providing continuous contralateral diagnostic angiography throughout the intervention. Continuous real-time visualisation of the aortoiliac bifurcation facilitated precise identification of the proximal cap, accurate determination of stent landing zones, and immediate confirmation of bifurcation preservation. These advantages are inherently access-related and cannot be consistently achieved with single-access techniques, particularly in unilateral CIA CTOs extending close to the bifurcation. Accordingly, our findings support the concept that access planning should be regarded as an integral component of endovascular strategy rather than a bailout manoeuvre reserved for failed single-access attempts [9–11]. Although various antegrade, retrograde, and combined crossing techniques have been described for iliac artery CTOs, evidence guiding the optimal initial access approach remains limited [10, 12]. Traditionally, dual-access strategies have been employed as secondary options after unsuccessful primary attempts. In contrast, the present study suggests that planned bilateral femoral access may offer procedural advantages in selected anatomically complex unilateral lesions, including those with suspected ostial involvement, long-segment occlusions, or heavy calcification, where enhanced angiographic control is essential for procedural safety. Importantly, despite the use of bilateral femoral access, access-related complications were infrequent and manageable in this cohort. Access-site haematomas occurred at a low rate and were treated conservatively, while no access-related major adverse events were observed. These findings indicate that, when performed in a controlled and planned manner, bilateral femoral access does not substantially increase access-related risk and may provide a favourable balance between procedural safety and angiographic control in complex iliac interventions.
Clinical follow-up was conducted in accordance with routine practice and current guideline recommendations, with imaging reserved for patients presenting with recurrent symptoms [8]. During a median follow-up of 13 months, symptom recurrence occurred in 20% of patients, and target lesion revascularisation was required in 10%. These outcomes are comparable to mid-term results reported in previous endovascular series addressing iliac artery CTOs [11, 12]. Although asymptomatic restenosis may have been underestimated due to selective imaging, the relatively low rates of clinical recurrence and reintervention suggest acceptable durability of the intervention. The absence of a comparator group precludes direct conclusions regarding the superiority of bilateral femoral access over single-access strategies. Therefore, this approach should be interpreted as a procedural optimisation tool aimed at enhancing technical control and safety in complex unilateral CIA CTOs rather than as a universally superior access technique. Nevertheless, the high technical success observed in a cohort predominantly composed of TASC II C–D lesions highlights the potential value of this strategy in carefully selected patients and supports further comparative evaluation in larger prospective studies.
Mechanical thrombectomy using the ClotTriever system has emerged as an effective option for the management of extensive iliocaval thrombosis, particularly in patients with large thrombus burden or associated pulmonary embolism. Recent reports have demonstrated successful thrombus removal without the need for systemic thrombolysis, highlighting the growing role of mechanical thrombectomy devices in complex venous thromboembolic disease and their potential to reduce bleeding-related complications [16]. Similarly, hybrid strategies combining endovascular and open techniques have been reported as feasible and safe in patients with multilevel vascular disease. Simultaneous treatment of abdominal aortic aneurysm (AAA) and common femoral artery (CFA) aneurysm using EVAR and open CFA repair has shown favourable outcomes in selected patients, supporting its role in reducing cumulative operative exposure and hospitalisation time [17]. Dialysis access steal syndrome (DASS) represents another challenging vascular condition requiring individualised management. Contemporary treatment options include flow-reduction techniques such as banding or MILLER procedures and revascularisation strategies including DRIL, RUDI, and PAI, all of which have demonstrated effective symptom relief while preserving access patency [18].
This study has several limitations. First, its retrospective, single-centre design and relatively small sample size may limit the generalisability of the findings. Second, the absence of a comparator group precludes direct comparison between bilateral femoral access and single-access strategies. Third, follow-up imaging was performed selectively in symptomatic patients, which may have led to underestimation of asymptomatic restenosis. Finally, lesion assessment was based on angiography alone, without routine use of cross-sectional imaging.
In conclusion, in patients with unilateral chronic total occlusion of the common iliac artery, a planned first-line bilateral femoral endovascular approach achieved high technical success with a low rate of periprocedural complications, even in predominantly TASC II C–D lesions. By providing continuous contralateral angiographic visualisation, this strategy enhances procedural control and bifurcation preservation and may be particularly valuable in anatomically complex cases, although comparative studies are required to define its role relative to single-access approaches.