Introduction
Perioperative atrial fibrillation (POAF) is a complication that is most commonly encountered after coronary artery bypass grafting (CABG), with a reported incidence of 20% to 40% in recent series [1–3]. While percutaneous coronary intervention and CABG are well-proven methods for treating patients with coronary artery disease, it is largely within the context of CABG that POAF is encountered, and it is a significant factor for early morbidity within this patient population [1, 2]. Traditionally, POAF was considered to be a stress-induced, reversible arrhythmia. Recently, however, there is growing evidence that POAF is linked with significant adverse postoperative outcomes, such as increased intensive care unit stay, longer hospitalization, greater need for postoperative interventions, and increased incidence of acute kidney injury [3–6]. These findings would suggest that POAF might be indicative of underlying systemic postoperative risk, rather than merely an electrophysiological phenomenon. There are several patient-related and procedure-related risk factors that have been identified for the development of POAF. Advanced age, atrial structural abnormalities, left ventricular systolic dysfunction, chronic kidney disease, and the pro-inflammatory effects of cardiopulmonary bypass have been identified as risk factors for the development of atrial fibrillation following cardiac surgery [2, 4, 6–10]. It is important to note that these risk factors are not only common but also occur cumulatively in patients undergoing CABG.
From a contemporary perioperative cardiology perspective, integrating patient-related and procedure-related factors into a clinically meaningful risk phenotype may provide greater practical value than evaluating individual predictors in isolation. Such an approach may enable improved perioperative risk stratification, targeted postoperative surveillance, and earlier multidisciplinary intervention in patients undergoing isolated CABG.
Although numerous individual risk factors for perioperative atrial fibrillation have been previously reported, data evaluating the combined effect of these factors within contemporary CABG populations and their association with early clinically relevant outcomes remain limited. In particular, real-world institutional cohorts reflecting modern perioperative management strategies may provide clinically relevant insights into early postoperative morbidity patterns.
Therefore, the aim of the present study was not only to identify independent clinical and procedural predictors of POAF, but also to characterise a contemporary high-risk perioperative phenotype and to evaluate its relationship with early, clinically significant outcomes in patients undergoing isolated CABG. The current study will focus on patients with isolated CABG and at increased risk for early postprocedural complications [7, 11, 12]. Nevertheless, literature incorporating both risk factors into a comprehensive risk profile in modern CABG patient populations is scarce. In this context, the purpose of the current study is to determine the clinical and procedural risk predictors of POAF, and to assess the relationship between POAF and early clinical outcomes. The current study aims to contribute to better perioperative risk stratification and cardiology-focused perioperative care in patients with isolated CABG. The current study will focus on patients with isolated CABG.
Material and methods
Study design and population
The present retrospective cohort study included all adult patients who underwent isolated CABG between January 2022 and December 2025 at a single centre. Patients with a documented history of atrial fibrillation or flutter before the procedure, patients with concurrent cardiac surgery, and all patients with incomplete data were excluded from the study, after which, a final study population of 550 patients was achieved.
Data collection
Demographic, clinical, laboratory, echocardiographic, procedural, and early postoperative variables were collected from the institution’s electronic medical record system. These variables included preoperative factors: age, sex, cardiac risk factors, comorbidities, baseline renal function, and transthoracic echocardiographic studies, which included measurements of the left ventricular ejection fraction and the left atrial dimension. Other factors were procedural variables: the use of cardiopulmonary bypass, the duration of cardiopulmonary bypass, the aortic cross-clamp time, and the transfusion of red blood cells.
Definition of perioperative atrial fibrillation
Atrial fibrillation or flutter occurring perioperatively (POAF) was considered to be new onset and occurred within seven days following surgery or before hospital discharge, whichever came first. The diagnosis of POAF was made using continuous telemetry monitoring and/or standard 12-lead electrocardiogram. Only those episodes lasting 30 s or more, or those that required pharmacologic or electrical cardioversion, were considered to be clinically significant.
Study outcomes
The main endpoint was the development of POAF. Secondary endpoints were early clinically relevant events in the postoperative course, such as acute kidney injury according to Kidney Disease: Improving Global Outcomes (KDIGO) criteria, intensive care unit stay, total hospital stay, need for prolonged ventilation defined by ventilation for more than 24 h, cerebrovascular events, and in-hospital mortality.
Patients with incomplete data in the perioperative period were removed before stratification of the groups. The analysis was performed using the complete-case method, considering only the patients in whom the variables related to the preoperative, operative, and postoperative periods were completely available. Due to the retrospective nature of the study, the percentage of patients removed, and the nature of the data, imputation strategies were not necessary.
Statistical analysis
For continuous variables, the data are represented as mean ± standard deviation or median with interquartile range, depending upon the nature of data, and analysed using Student’s t-test or the Mann-Whitney U test. For categorical variables, data are represented in terms of frequency and proportion, and analysed using the χ2 test or Fisher’s exact test, depending upon the sample size. The univariable analysis was first conducted to evaluate the relationship of clinical and procedural factors with the incidence of POAF. Those with a p-value of < 0.10 in the univariable analysis, along with clinically relevant factors suggested by previous studies, were included in a multivariable logistic regression analysis to determine the independent predictors of POAF. Collinearity between the potential predictors of age and chronic kidney disease was evaluated before the development of the multivariable logistic regression analysis, which was found to be acceptable. The results of the multivariable analysis are given in the form of odds ratios along with their 95% confidence intervals. The calibration and discriminant ability of the models was tested by standard methods. For all statistical tests, p < 0.05 was considered significant. Standard statistical software was used for statistical calculations.
Results
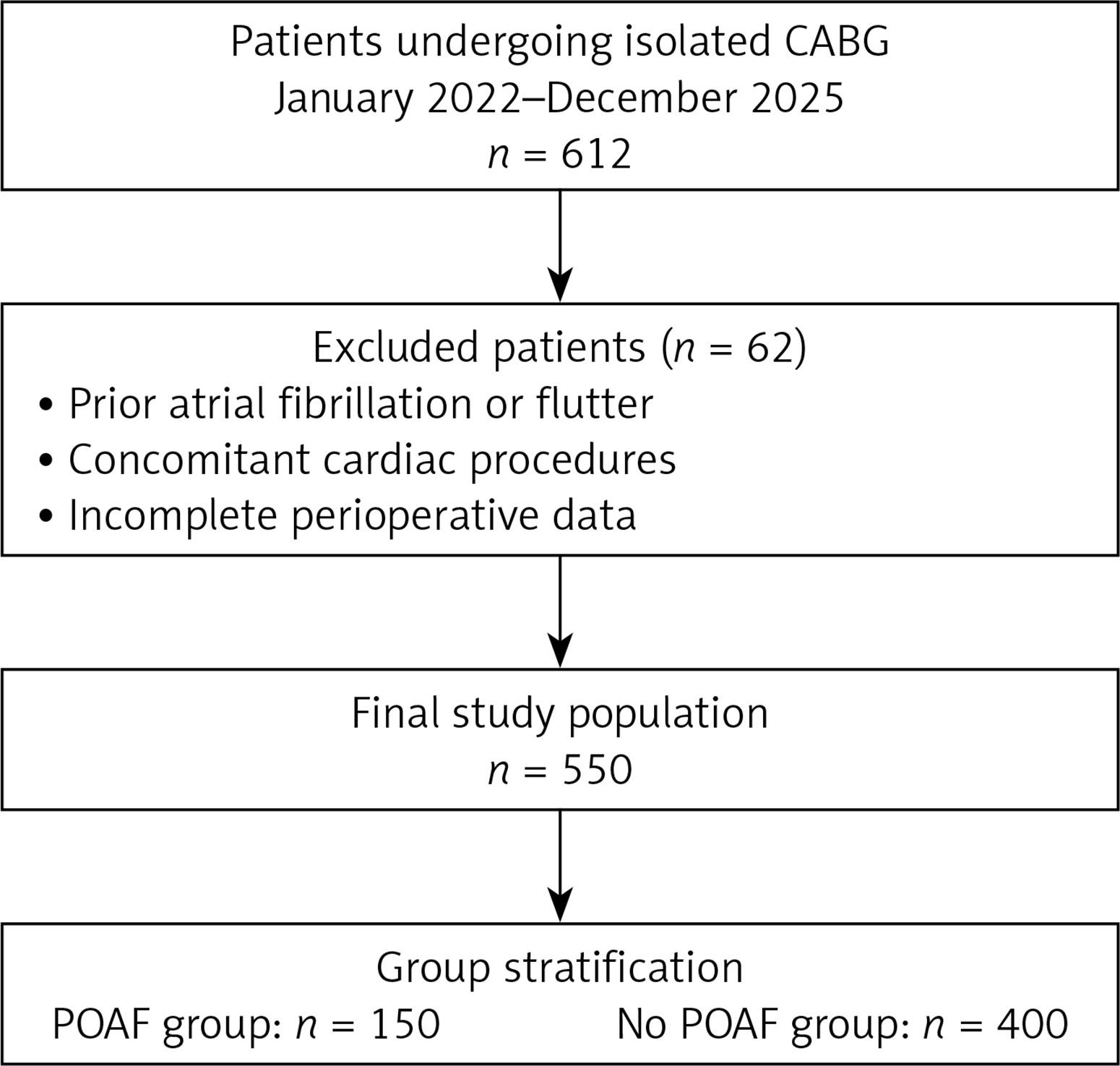
From January 2022 through December 2025, a total of 612 consecutive patients underwent an isolated CABG procedure. After exclusion of the patients with a previous history of atrial fibrillation or flutter, associated cardiac surgery, or incomplete data, a final study population of 550 patients was obtained (Figure 1). Patients were divided into a POAF group (150) and a no-POAF group (400) based on the development of POAF. The incidence of POAF was found to be 27.3%.
Figure 1
Study flow diagram of the isolated coronary artery bypass grafting (CABG) cohort. The diagram illustrates patient selection, exclusion criteria, and final group stratification according to the development of perioperative atrial fibrillation
Baseline clinical and procedural characteristics
The baseline clinical, echocardiographic, and selected procedural variables of the studied population are shown in Table I. The patients who had POAF were older than those who had sinus rhythm. The incidence of chronic kidney disease was greater in the POAF group. Echocardiography showed a diminished ejection fraction of the left ventricle and increased diameter of the left atrium.
Table I
Baseline clinical and procedural characteristics of the study population
| Variable | POAF (n = 150) | No POAF (n = 400) | P-value |
|---|---|---|---|
| Age [years] | 68 ±9 | 61 ±10 | < 0.001 |
| Male sex, n (%) | 108 (72.0) | 300 (75.0) | 0.46 |
| Chronic kidney disease, n (%) | 27 (18.0) | 36 (9.0) | 0.003 |
| Left ventricular ejection fraction, % | 48 ±9 | 51 ±8 | 0.002 |
| Left atrial diameter [mm] | 42 ±5 | 38 ±4 | < 0.001 |
| Hypertension, n (%) | 102 (68.0) | 248 (62.0) | 0.17 |
| Diabetes mellitus, n (%) | 66 (44.0) | 154 (38.5) | 0.24 |
| Cardiopulmonary bypass time [min] | 102 ±26 | 88 ±22 | < 0.001 |
| Perioperative red blood cell transfusion*, n (%) | 69 (46.0) | 116 (29.0) | < 0.001 |
In terms of procedural variables, the cardiopulmonary bypass time was longer and perioperative blood transfusion was more often needed in patients with POAF (Table I). There were no statistically significant differences between patients with and patients without POAF with respect to gender distribution, presence of hypertension, and diabetes mellitus (Table I).
Early postoperative outcomes
Early clinically significant outcomes after surgery, stratified by the development of POAF, are reported in Table II. Patients with POAF had a significantly increased risk of acute kidney injury than those without POAF (22.0% vs. 11.0%, p = 0.001). Furthermore, patients with POAF had an increased length of stay in the ICU and overall hospital stay.
Table II
Early postoperative outcomes according to POAF status
The incidence of prolonged mechanical ventilation (> 24 h) was also higher in the POAF group. On the other hand, the incidence of cerebrovascular events and in-hospital deaths did not differ significantly between the two groups (Table II).
Independent predictors of perioperative atrial fibrillation
The outcome of the multivariate logistic regression analysis to determine the independent predictors of POAF is presented in Table III and Figure 2. Older age, chronic kidney disease, larger left atrium, lower left ventricular ejection fraction, longer cardiopulmonary bypass time, and perioperative red blood cell transfusion were identified as predictors of POAF.
Table III
Multivariable predictors of perioperative atrial fibrillation after isolated CAB
| Variable | Odds tatio | 95% confidence interval | P-value |
|---|---|---|---|
| Age [year] | 1.05 | 1.03–1.07 | < 0.001 |
| Left atrial diameter [mm] | 1.17 | 1.11–1.23 | < 0.001 |
| Left ventricular ejection fraction (%) | 0.97 | 0.95–0.99 | 0.01 |
| Chronic kidney disease | 1.68 | 1.05–2.68 | 0.03 |
| Cardiopulmonary bypass time [min] | 1.01 | 1.00–1.02 | 0.002 |
| Perioperative red blood cell transfusion* | 1.59 | 1.10–2.30 | 0.01 |
Figure 2
Multivariable predictors of perioperative atrial fibrillation after isolated coronary artery bypass grafting. Multivariable logistic regression analysis identified advanced age (OR = 1.05, 95% CI: 1.03–1.07), left atrial diameter (OR = 1.17, 95% CI: 1.11–1.23), reduced left ventricular ejection fraction (OR = 0.97, 95% CI: 0.95–0.99), chronic kidney disease (OR = 1.68, 95% CI: 1.05–2.68), prolonged cardiopulmonary bypass time (OR = 1.01, 95% CI: 1.00–1.02), and perioperative red blood cell transfusion (OR = 1.59, 95% CI: 1.10–2.30) as independent predictors of POAF
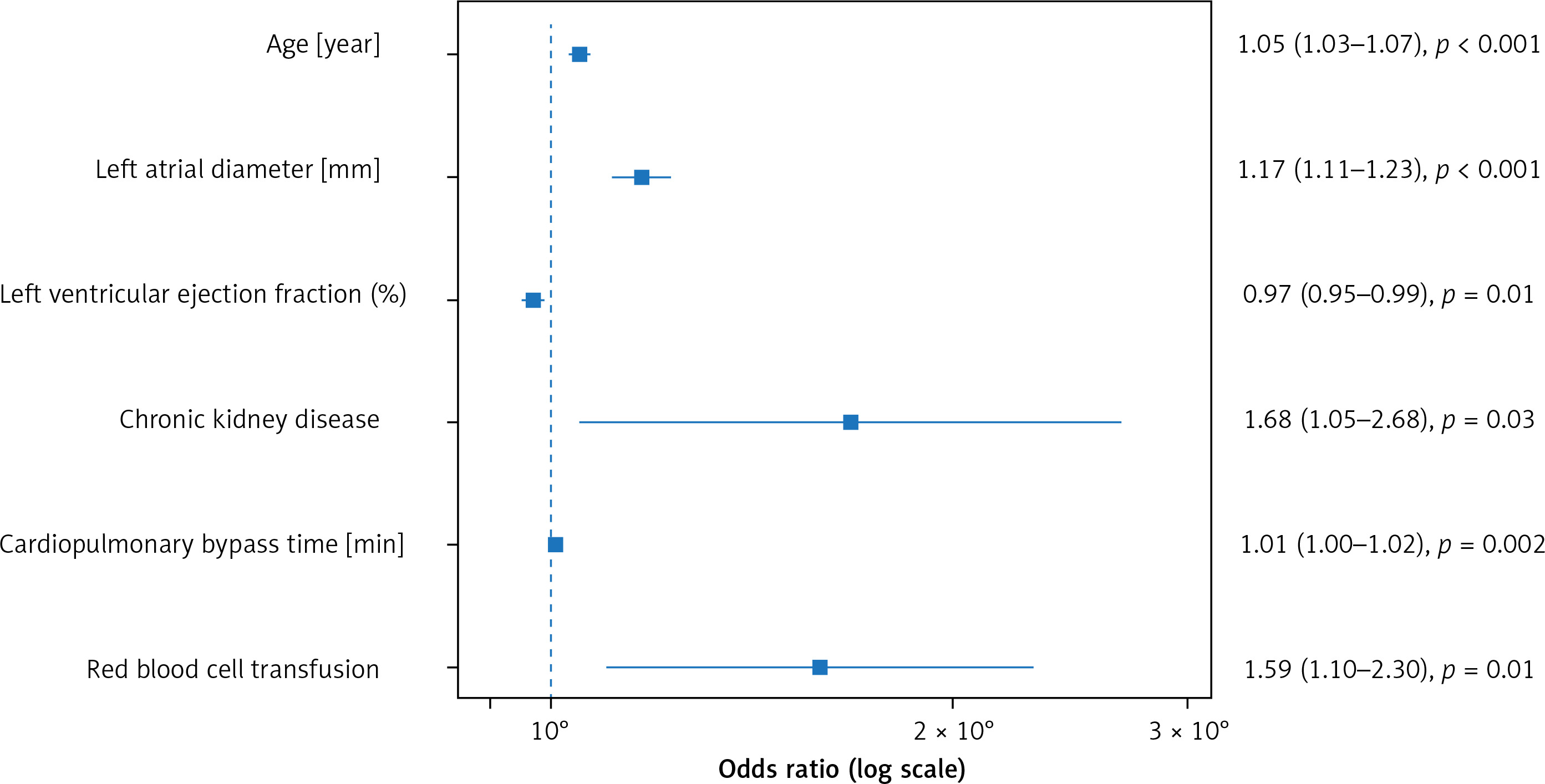
The forest plot in Figure 2 above shows the strength of the associations, suggesting that both patient variables and CABG procedure variables played a part in the risk of having POAF.
Discussion
What this case study shows is that POAF continues to be a common complication following isolated CABG, and that POAF is strongly linked to an increased risk of early morbidity in the postoperative period. In this contemporary population, POAF also occurred in more than a quarter of the patients, which is in keeping with previously published figures, which have ranged from 20% to 40% in patients undergoing CABG [1–3]. Notably, the occurrence of POAF increased the risk of AKI and length of stay in both the ICU and in-hospital, but in-hospital mortality was not increased, as previously reported [5–7]. Importantly, the novelty of the present study lies not in identifying entirely new predictors of perioperative atrial fibrillation, but in defining an integrated high-risk perioperative phenotype within a contemporary CABG population. This phenotype-based interpretation provides a clinically applicable framework that links routinely available clinical and procedural parameters to early postoperative morbidity risk. In contrast to the discovery of new predictors, the current study focuses on the importance of a set of common clinical and operative variables that tend to combine into a distinct high-risk perioperative pattern for the development of POAF. Older age, the presence of chronic kidney disease, atrial structural abnormalities, left ventricular systolic dysfunction, and indicators of operative stress, such as prolonged cardiopulmonary bypass and perioperative blood transfusions, have all been individually identified as contributing factors to postoperative atrial fibrillation in previous investigations [2, 4, 6–10]. The current study confirms the significance of these variables within a comprehensive multivariate model. The finding of an association between POAF and early postoperative morbidity is in keeping with the literature, which has shown an increase in healthcare utilisation, prolonged recovery times, and a heightened incidence of postoperative complications among patients with atrial fibrillation following cardiac surgery [3–7, 13]. Specifically, the finding of a marked association between POAF and acute kidney injury in the current study lends support to the idea that POAF can be considered a marker of a state of systemic perioperative stress, rather than a purely electrical event [6, 9]. A lack of association with in-hospital mortality supports the idea that POAF has a predominantly early effect on morbidity [5, 7].
From the perspective of a cardiology-oriented perioperative service, these data have several implications. The identification of patients who are at risk for POAF, according to easily obtainable clinical, echocardiographic, and procedural parameters, may allow for more careful observation for signs of abnormal rhythms in the postoperative period, as well as earlier consultation with the cardiology service [7, 11]. This may be particularly useful in patients who have compromised renal function, reduced cardiac reserve, or have had extensive operative time, where the presence of POAF often reflects a more complicated course [6, 9, 10]. However, the present study was not designed to derive or validate a formal predictive risk model. The identified variables should therefore be interpreted as indicators of an increased-risk clinical profile rather than components of a weighted prediction tool. Future prospective studies with dedicated derivation and validation cohorts are needed to develop and externally validate a formal risk score for POAF after CABG.
The procedural factors that were independently associated with the risk of POAF further underscore the importance of the stress of surgery and the inflammation process in the pathogenesis of atrial fibrillation postoperatively. The importance of cardiopulmonary bypass duration and perioperative blood transfusion could be a marker of the degree of inflammation, instability, and atrial distention, which have been suggested in the pathophysiology of atrial fibrillation postoperatively [4, 8, 9]. Although advanced age and chronic kidney disease are interrelated, both factors were independently associated with the development of POAF, which suggests that kidney dysfunction is a risk factor for developing atrial fibrillation over and above the effect of age. This finding is consistent with previous research indicating that postoperative atrial fibrillation can occur due to systemic inflammatory and metabolic processes and kidney dysfunction [6, 9, 10]. Cumulatively, the current findings indicate that POAF can be used to distinguish a subset of patients undergoing elective CABG, who are predisposed to the early postoperative development of complications. This predisposition can potentially be addressed through the optimisation of postoperative care, based on the appreciation of this high-risk subgroup.
Several limitations of this study should be acknowledged. First, the retrospective and single-centre design may limit the generalisability of the findings. Although consecutive patients were included, unmeasured confounding factors inherent to observational studies cannot be completely excluded. Second, despite the use of continuous telemetry monitoring, brief or asymptomatic episodes of atrial fibrillation may have remained undetected, potentially leading to underestimation of the true incidence of POAF. Third, perioperative pharmacological strategies, including prophylactic antiarrhythmic or beta-blocker use, were not systematically analysed due to heterogeneity in institutional practice, and therefore their potential influence on the occurrence of POAF could not be fully assessed. Additionally, certain historical clinical variables, including detailed prior myocardial infarction history, previous coronary revascularisation procedures, prior cerebrovascular events, and formal diagnoses of heart failure, were not consistently available in a standardised format within the institutional database. Therefore, these variables could not be included in the baseline characterisation, which may limit the comprehensiveness of risk profiling. Finally, the analysis was restricted to in-hospital outcomes, and the long-term clinical consequences of POAF, including late recurrence of atrial fibrillation or thromboembolic events, could not be evaluated. In addition, this study was not designed to derive or validate a weighted clinical risk score; therefore, the identified predictors should not be interpreted as a formal prediction model.
In conclusion, in the setting of isolated coronary artery bypass graft surgery, the perioperative occurrence of atrial fibrillation is known to be a frequent complication, associated with increased morbidity in the early postoperative period, but without having any significant effect on in-hospital mortality. The use of clinical variables could aid in the stratification of risk in patients, to provide more intensive cardiology-oriented care in the early postoperative period.