Autoamputation is defined as the spontaneous detachment of a necrotic, nonviable part of the body without surgical intervention. This rare phenomenon typically occurs in tissues that have undergone severe ischemic insult, become desiccated and mummified, and subsequently separate along a natural line of demarcation between viable and necrotic tissue. While autoamputation is often reported in the digits, it may occasionally involve more proximal parts of the limb, including the foot or even the entire lower extremity [1–3].
The process of autoamputation is most associated with dry gangrene, in which progressive arterial occlusion or microcirculatory failure leads to tissue necrosis and mummification in the absence of infection. The affected region becomes dry, black, and shrunken, often remaining painless due to concomitant neuropathy or ischemic nerve damage. In contrast, wet gangrene, typically characterized by superimposed bacterial infection and tissue edema, requires urgent surgical debridement or amputation to prevent systemic sepsis [4].
Historically, autoamputation has been described in diverse contexts, including profound peripheral arterial insufficiency, frostbite injuries at high altitudes [1], diabetic foot disease with severe ischemia and neuropathy [2, 4, 5], vasopressor-induced peripheral ischemia during septic shock, and severe autoimmune vasculopathies such as Raynaud’s phenomenon in connective tissue diseases such as Sjögren’s syndrome [3]. Case reports have also documented spontaneous loss of limbs in the setting of untreated gas gangrene [6]. These observations highlight that although the underlying etiologies vary, the final pathway involves critical ischemia leading to dry, mummified gangrene.
Management of dry gangrene remains debated. Some vascular specialists advocate early surgical amputation to shorten the healing period and minimize the risk of secondary infection. In contrast, others favor a conservative “awaiting autoamputation” strategy, particularly in frail patients with high operative risk or limited life expectancy [4, 5]. Observational studies have shown that the autoamputation process may take several months, which can be distressing for patients but may avoid higher-level amputation in ischemic limbs [5].
Herein, we describe two cases of lower-extremity autoamputation following severe peripheral ischemia of different etiologies: one related to vasopressor-induced ischemia during septic shock, and the other in a bedridden elderly patient with chronic critical limb ischemia. We discuss their clinical course and management in the context of current literature on this uncommon but clinically significant phenomenon.
Case 1. A 70-year-old woman without a history of diabetes mellitus was admitted to the intensive care unit (ICU) of a regional hospital because of severe community-acquired pneumonia complicated by acute respiratory failure. She required endotracheal intubation and mechanical ventilation. During the course of septic shock, she developed persistent hypotension that necessitated high-dose vasopressor support with norepinephrine and adrenaline to maintain adequate mean arterial pressure.
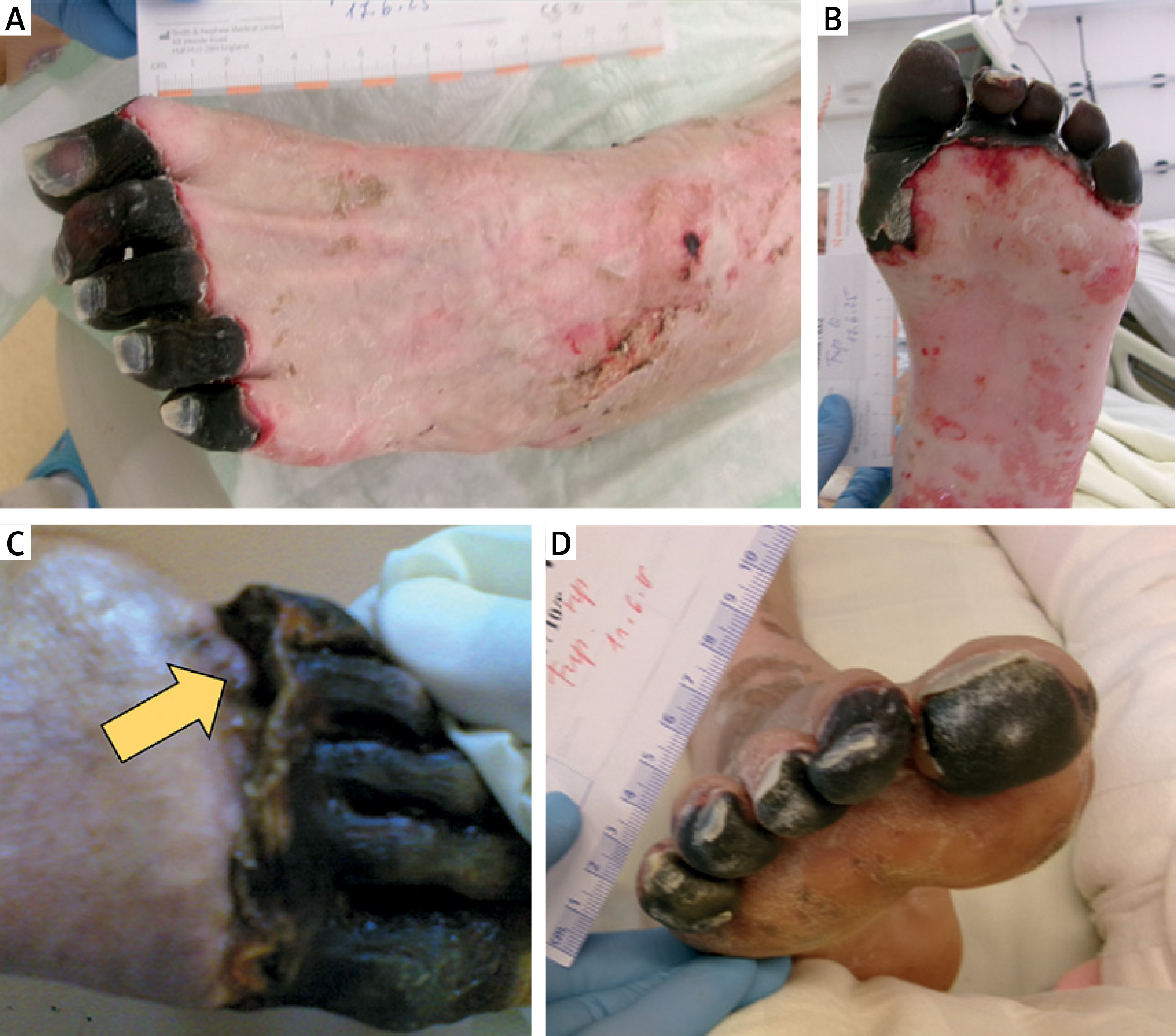
Within the second week of her ICU stay, progressive cyanotic discoloration of all toes on both feet became evident. Over subsequent days, the lesions evolved into well-demarcated, mummified dry gangrene affecting all digits bilaterally (Figure 1). No signs of local infection – such as erythema, swelling, drainage, or malodor – were noted, and laboratory markers of systemic infection remained unremarkable. Vascular imaging studies could not be obtained at that stage because her hemodynamic status remained fragile and she was not fit for transfer. The ischemic necrosis was attributed to profound peripheral vasoconstriction and microcirculatory compromise secondary to prolonged vasopressor therapy in the context of septic shock.
Figure 1
Lower-limb involvement in Case 1 showing progressive ischemic changes and autoamputation of both feet. A – Dorsal view of the left foot demonstrating sharply demarcated acral ischemic lesions. B – Plantar view of the left foot with similar mummified changes. C – Autoamputation (arrow) of the distal portion of the left foot after prolonged conservative management. D – The right foot exhibiting dry gangrene of the toes with a clear line of demarcation
Once her pulmonary function and hemodynamics stabilized, she was successfully weaned off vasopressors and ventilatory support and later transferred to a general medical ward. Considering the dry nature of the gangrene and the absence of superimposed infection, a conservative, non-operative strategy was pursued. The patient was instructed to minimize weight bearing and was treated with daily local antiseptic dressings to prevent secondary infection and to protect the fragile necrotic tissue.
Over the ensuing 6 months, the toes remained dry, shriveled, and sharply demarcated from viable tissue, without any clinical evidence of cellulitis or progressive necrosis. Eventually, spontaneous autoamputation occurred: the necrotic digits became detached with minimal manipulation because the phalangeal bones were friable and fractured easily with gentle traction (Figure 1 C). The process was completed at the bedside by carefully removing the remaining non-viable fragments, followed by limited debridement of the exposed bone ends using a Luer osteotome.
The wounds were allowed to heal by secondary intention under continued daily dressing changes. Complete epithelialization was achieved within two months after autoamputation. Throughout the entire course, the patient remained free from local or systemic infection, and the healed amputation sites were stable and painless at follow-up. She retained adequate ambulation despite the loss of all toes.
Case 2. An 83-year-old woman, long-term bedridden in a nursing home because of profound physical disability following a previous ischemic stroke, was referred to the vascular surgery service with advanced ischemic gangrene of the right lower limb. Her medical history was significant for severe cardiovascular and neurological comorbidities, rendering her non-ambulatory for several years. The affected limb showed extensive dry gangrene extending from the foot to the mid-leg level, with clear demarcation between necrotic and viable tissue. There was no associated foul odor, discharge, erythema, or other signs suggestive of superimposed infection or wet gangrene. Laboratory workup showed no leukocytosis or biochemical evidence of systemic sepsis.
Given her advanced age, frailty, poor functional status, and prohibitive surgical risk, as well as the absence of infection, the treating team elected to manage her conservatively. The goals of care focused on comfort, local infection prevention, and preservation of the remaining viable tissue. The patient remained in the nursing facility under close outpatient vascular follow-up. Regular antiseptic dressings were applied, and she was closely monitored for pain, local cellulitis, or systemic deterioration.
Approximately 2 months after initial presentation, the patient returned to the emergency department because of progressive loosening and near-complete separation of the necrotic distal portion of the limb, consistent with ongoing autoamputation (Figure 2). At the bedside, the vascular surgeons noted that the devitalized segment was attached only by fragile, desiccated soft tissue and nonviable bone. With minimal manual effort, the distal bones fractured due to their marked ischemic fragility and were removed. Gentle trimming of the residual bony stump was performed, using a Luer osteotome to smooth sharp edges and prevent skin trauma.
Figure 2
Formation of the natural demarcation line between viable and necrotic tissues in the affected limb in Case 2. The dermis progressively advanced inward along this line (arrows), promoting healing of the proximal viable tissue, while the distal gangrenous segment became progressively desiccated and shrunken before eventual autoamputation

The wound was left open to heal by secondary intention, protected with daily antiseptic dressings performed at the nursing home under medical supervision. No clinical infection developed during the healing phase. Over the following weeks, gradual granulation and epithelialization of the wound occurred, leading to satisfactory closure of the stump without the need for further surgical intervention. The patient remained hemodynamically stable, with no evidence of recurrent ischemia or septic complications during follow-up.
The two presented cases illustrate the rare but clinically significant occurrence of autoamputation in dry gangrene of the lower extremities, arising from different etiologies. They highlight the importance of understanding underlying mechanisms, carefully selecting patients for conservative management, and closely monitoring for complications.
Pathophysiology and predisposing factors. Autoamputation represents the result of prolonged ischemia, where necrotic, mummified tissue separates spontaneously at a natural line of demarcation between viable and non-viable tissue [1–3]. In Case 1, the ischemic insult was caused by vasopressor-induced peripheral ischemia in septic shock. High-dose vasoconstrictors such as norepinephrine and adrenaline can severely compromise peripheral perfusion in an already unstable microcirculation, occasionally leading to ischemic necrosis and tissue loss [7–9]. Sepsis itself may exacerbate the process through endothelial injury and micro-thrombotic changes [8]. In Case 2, the patient’s chronic critical limb ischemia – likely from advanced peripheral arterial disease and compounded by severe comorbidities – created a low-flow state that predisposed her to spontaneous dry gangrene without acute hemodynamic stress.
Aside from vasopressor-induced ischemia, other recognized causes of autoamputation include frostbite [1], diabetic foot disease [2, 4, 5], autoimmune vasculopathies such as severe Raynaud’s phenomenon in Sjögren’s syndrome [3], and rare infections such as gas gangrene [6]. Despite the diverse etiologies, these conditions share the common pathway of critical ischemia resulting in dry, mummified gangrene.
Temporal course of autoamputation. The process of autoamputation is typically slow and protracted. In our first case, separation occurred after about 6 months, while in the second case, it was completed within 2 months. This timeline is comparable to findings in diabetic foot series. Fikri et al. reported that autoamputation often required 4–6 months when a conservative “wait-and-see” approach was adopted [5]. The brittle nature of necrotic bone and connective tissue facilitates spontaneous detachment; in both of our patients, the non-viable segments separated with minimal traction.
Management: conservative vs. surgical. A key challenge in managing dry gangrene is deciding between early surgical amputation after demarcation versus a conservative strategy allowing natural autoamputation [5, 9]. Conservative management can be advantageous in frail patients or those with poor limb perfusion, as surgical wounds in ischemic tissue may heal poorly or require a more proximal level of amputation [4, 5]. Some studies support this approach: Fikri et al. demonstrated that certain patients with diabetic toe gangrene healed successfully after spontaneous autoamputation, avoiding higher-level surgery [5]. Similarly, Elgzyri et al. showed that many patients with diabetic forefoot gangrene achieved healing below the ankle without major amputation [10].
However, the conservative approach is not risk-free. Al Wahbi et al. report that in diabetic patients with dry toe gangrene, only a few experience autoamputation, while most patients eventually need surgical amputation [4]. This underlines the risks of delayed healing, prolonged wound care, and potential progression to infection. Furthermore, in some vascular series, conversion from dry to wet gangrene was reported in approximately 7–8% of cases within 30 days after revascularization, emphasizing the need for vigilant follow-up [11, 12].
In our cases, advanced age, comorbidities, absence of infection, and high operative risk justified a conservative approach. Both patients achieved complete healing by secondary intention, avoiding higher-level amputations. In Case 1, delayed intervention was prudent during ongoing microcirculatory compromise from vasopressors. In Case 2, limited life expectancy and chronic ischemia further favored non-operative care.
Where perfusion is adequate and infection risk is low, some vascular surgeons advocate early surgical removal of well-demarcated necrotic tissue to shorten the healing period and reduce nursing demands [4, 5]. Thus, treatment decisions should be individualized based on vascular status, comorbidities, infection risk, and patient preference.
Clinical recommendations. 1) Frequent inspection of extremities in ICU patients receiving vasopressors is crucial to detect early ischemic changes [7–9]. 2) Titration and timely tapering of vasopressors – or use of less vasoconstrictive agents when feasible – may mitigate further ischemic damage [7, 8]. 3) Conservative management should be reserved for patients with clearly demarcated dry gangrene, no evidence of infection, high operative risk, or limited life expectancy. 4) Close monitoring is mandatory; any sign of cellulitis or systemic infection warrants prompt surgical intervention. 5) Meticulous wound care and daily dressings are essential to support secondary healing. 6) Detailed case reporting contributes to collective knowledge of prognosis and best practices for dry gangrene and autoamputation.
Our report is limited by the absence of vascular imaging to objectively assess arterial inflow and collateral circulation. Much of the current evidence derives from diabetic foot literature, which may not directly translate to non-diabetic or vasopressor-induced ischemia. Further prospective studies and multicenter data are needed to clarify optimal management strategies.
To sum up, autoamputation of the lower extremity remains rare but can be a viable outcome in selected high-risk patients with stable dry gangrene. Conservative care is effective when infection is absent, but vigilant follow-up is vital to avoid deterioration. Individualized treatment planning remains the cornerstone of managing this complex condition.
Autoamputation of the lower extremities is an uncommon but clinically relevant outcome of severe peripheral ischemia, typically occurring in the context of dry, non-infected gangrene. The 2 cases presented – one associated with vasopressor-induced ischemia in septic shock and the other with chronic critical limb ischemia – illustrate that conservative management can be a safe and effective strategy in carefully selected, high-risk patients. This approach may spare frail individuals from higher-level amputations and extensive surgical trauma. Nevertheless, close monitoring is essential to detect early signs of infection or conversion to wet gangrene, which would necessitate prompt intervention. Timely recognition of ischemia, individualized treatment planning, meticulous wound care, and interdisciplinary decision-making remain crucial to optimizing outcomes in this rare but challenging clinical scenario.