Introduction
Dyslipidaemia, characterized by abnormal serum lipid profile, is a prevalent and significant risk factor for the development of cardiovascular diseases (CVDs) [1] and is closely associated with other metabolic disorders, such as insulin resistance [2]. The pathogenesis of dyslipidaemia is complex and multifactorial, involving genetic predisposition, dietary habits, sedentary lifestyles [3], and more recently, dysbiosis, and alterations in gut microbiota (GM) composition and its metabolites [4].
The GM, a complex ecosystem composed of trillions of microorganisms, including bacteria, viruses, fungi, and archaea [5], has emerged as a key player in various aspects of host physiology, including nutrient metabolism, immune function, and the maintenance of gut barrier integrity [6, 7]. The influence of the GM on host lipid metabolism is mediated through metabolites produced by the GM, including short-chain fatty acids (SCFA), secondary bile acids, trimethylamine (TMA), and lipopolysaccharide (LPS) or endotoxin [8].
In dysbiosis conditions, the intestinal barrier is disrupted, leading to increased gut permeability [9] and bacterial endotoxins can translocate into the systemic circulation, triggering inflammatory responses and metabolic dysfunction [10]. Increased serum endotoxin levels or low-grade endotoxaemia are biomarkers for the assessment of gut permeability [11] and have been observed in individuals who are at risk of atherosclerosis and CVDs [12].
TMAO, on the other hand, is a metabolite produced by the GM metabolism of dietary choline, betaine, and L-carnitine. These substances metabolize to TMA and are then transformed into TMAO by hepatic flavin monooxygenases (FMOs) [13]. Elevated TMAO can contribute to inflammation, impair vascular function and structure, inhibit reverse cholesterol transport, and induce dyslipidaemia [14].
Probiotics and prebiotics are suggested to improve dysbiosis, gut permeability, and subsequently, low-grade endotoxaemia [12], and also to decrease the serum TMAO [15] through the effect of GM on the epithelial barrier [9].
Synbiotics, a combination of probiotics and prebiotics, aim to restore a healthy GM balance and modulate the production of metabolites, potentially improving lipid metabolism and reducing cardiovascular risk [16].
To the best of our knowledge, this is the first study investigating the effects of synbiotic administration on serum levels of TMAO and LPS as indirect measures of gut permeability [11] novel metabolic biomarkers for CVD risk [17] in patients with dyslipidaemia. This study aimed to explore the potential effect of a 12-week synbiotic supplementation on TMAO, LPS, and FBG levels in patients diagnosed with dyslipidaemia while shedding light on the intricate connections between dysbiosis, metabolic disorders, and potential therapeutic strategies.
Material and methods
Ethics statements
This study was approved by the Ethics Committee at the Ahvaz Jundishapur University of Medical Sciences based on the ethical guidelines of the 1975 Declaration of Helsinki (Approval code: IR.AJUMS.REC.1400.581), and it was registered in the Iranian Registry of Clinical Trials (Registration reference: IRCT20180128038540N2).
All participants were informed about the study protocol, and a written consent form was signed by participants during their registration.
Study design and participants
This study was a randomized, double-blind, placebo-controlled clinical trial with a parallel design. The participants were selected from a pool of patients diagnosed with dyslipidaemia, who were referred to the nutrition clinic in Mahshahr, Iran, and met the following inclusion criteria: 1. Willingness to participate in the study; 2. Diagnosed with dyslipidaemia [18]; and 3. Adult individuals up to 60 years old. The patients were excluded from the study if any of the following criteria were detected at any time of the study procedure: 1. Frequent travel; 2. Using chemical or herbal lipid-lowering drugs; 3. Having familial dyslipidaemia; 4. Suffering from cardiovascular, kidney, liver, endocrine, gastrointestinal, malignancies, and autoimmune diseases; 5. Any significant changes in body weight and lifestyle in the last 6 months; and 6. Using tobacco, drugs, or alcohol.
The participant’s sociodemographic status, including age, gender, ethnicity, marital status, educational level, occupational status, smoking, and drinking alcohol, were evaluated through a self-report sociodemographic questionnaire at the time of recruitment.
Food intake and physical activity assessment
To evaluate the food intake of the participants, a 3-day (non-consecutive) food record was used at the beginning and end of the study. Energy and nutrient intakes including total calories, carbohydrates, protein, fat, saturated fatty acids (SFA), and fibre were analysed using Nutritionist IV software (First Data Bank; Hearst Corp, San Bruno, CA, USA).
Physical activity (PA) was assessed using a self-reported PA questionnaire [19] and was determined as metabolic equivalents of task hour/day (METs-h/day). To calculate each participant’s MET, times spent on each activity (h/day) were multiplied by their typical energy expenditures, expressed in terms of METs. Finally, these values were added together to give the MET-h/day score for each participant.
Anthropometric measurements
Anthropometric measurements, including height, weight, waist circumference (WC), and body fat percentage (BFP) were measured, and body mass index (BMI) was calculated at the beginning and the end of the study. Height was measured to the nearest 0.1 cm using a digital stadiometer (InBody, South Korea). Weight and BF were assessed in light clothes and without shoes by an electrical body composition analyser (InBody 270, South Korea). A measuring tape was used to measure WC to the nearest 0.1 cm at the midpoint between the lowest rib and the iliac crest.
Biochemical assessments
For biochemical assessments, blood samples (5 ml) after 10–12 h of overnight fasting at the beginning and after 12 weeks of intervention were taken. The serum was separated by centrifugation (3000 RPM for 15 min at 25°C) and kept refrigerated at –70°C for further analysis.
The Enzyme-Linked Immunosorbent Assay (ELISA) kits were applied for the determination of serum Endotoxin (MBS260730, MyBioSource, China) and serum levels of TMAO (MBS7269386, MyBioSource, China).
The serum level of fasting blood glucose (FBG) was assessed using a commercial test kit (Glucose-SL test kit, Henry Schein, Inc., USA) with an enzymatic colorimetric method.
Sample size
To estimate the necessary sample size, we used the equation for parallel interventional studies with an α error of 0.05 and a β error of 20% (power = 80%). Based on a previous study [20] and the parameter of total cholesterol, the sample size was determined to be n = 50, with 25 participants per group. To account for a projected 10% dropout rate, a total of 56 patients with dyslipidaemia (n = 28/group) were recruited after the screening process.
Intervention
Participants were allocated into a treatment or a control group by simple randomization method (computer-generated random numbers). Participants in the treatment group received one sachet of synbiotic powder, and those in the control group received a placebo sachet, dissolved in a cup of water, twice a day (30 min before lunch and dinner) for 12 weeks. Each synbiotic sachet contained a total dose of 3 × 1010 colony forming units (CFU) of 6 probiotic microorganism species, which were chosen based on previous studies, including Lactobacillus (L.) acidophilus [21], L. fermentum [22], L. plantarum [23], Bifidobacterium (B.) longum [24], B. lactis [25], and Saccharomyces (S.) boulardii [26] plus 5 g of prebiotics including inulin and fructooligosaccharide (FOS) [27] manufactured by Faradaru Pharmaceutical Company (Tehran, Iran). Placebo sachets (5 g corn starch) were identical in shape, size, colour, and packaging to the synbiotic sachets. Patients and researchers were blinded to the interventions. To blind the individuals who participated in the intervention, the packages were coded by a person who was not involved in the study.
Participants were asked to keep their usual diet and PA during the study. The daily reminder messages were sent to participants to ensure that they did not forget the consumption of supplements. At the end of the study, the percentage of unconsumed sachets was determined, and the patients who consumed less than 90% of their sachets were excluded from the study.
Statistical analysis
The normality of data distribution was determined by the Kolmogorov-Smirnov test. To compare parametric variables between 2 groups the independent sample t-test was used, and to compare variables within the group before and after the intervention a paired sample t-test was applied. To control for confounder variables, an analysis of covariance (ANCOVA) was used. Pearson’s coefficient correlation analysis was used to determine the correlation between changes in FBG with endotoxin and TMAO changes. All analysis was carried out by SPSS software version 28 (SPSS Inc., Chicago, Illinois, USA). Data were analysed using both intention-to-treat (ITT) and per protocol (PP) approach analysis. P ≤ 0.05 was considered statistically significant.
Results
Of 56 patients selected for the intervention (n = 28) and control groups (n = 28), 6 patients (3 patients of each group) were excluded from the study due to low compliance rates. A high compliance rate (90.0%) was seen in 50 patients who completed 12 weeks of study. The mean age of participants was 42.4 years (43.2 ±7.2 against 41.7 ±4.9 years, in the intervention and placebo groups, respectively, p = 0.4). All the participants were male because of logistic limitations.
No statistically significant differences were observed in anthropometric indices (weight, BMI, WC, BFP), nutrient intake (total calorie, carbohydrate, protein, fat, SFA, and fibre intakes), and PAL before and after the study between and within groups in the ITT and PP approaches (Table I).
Table I
Patients’ anthropometric indices, nutrient intake, and PAL before and after the study
| Variables | Intervention (n = 25) | Placebo (n = 25) | P-value* | |
|---|---|---|---|---|
| BMI [kg/m2] | Before | 30. 1 ±4.9 | 28.7 ±4.1 | 0.30 |
| After | 30.2 ±4.9 | 28.8 ±4.1 | 0.31 | |
| P-value* | 0.40 | 0.32 | ||
| WC [cm] | Before | 104.3 ±10.7 | 101.7 ±8.8 | 0.36 |
| After | 104.4 ±10.6 | 102.0 ±8.4 | 0.60 | |
| P-value | 0.80 | 0.47 | ||
| BF (%) | Before | 32.9 ±6.5 | 31.1 ±5.6 | 0.29 |
| After | 33.3 ±7.2 | 30.9 ±5.5 | 0.19 | |
| P-value | 0.27 | 0.56 | ||
| Calories intake [kcal] | Before | 2974±482 | 2861±441 | 0.51 |
| After | 3118.8±557 | 2980/3±453 | 0.44 | |
| P-value | 0.31 | 0.58 | ||
| CHO [gr] | Before | 418.8 ±85.0 | 397.7±72.4 | 0.41 |
| After | 433 ±89.2 | 411 ±81.2 | 0.46 | |
| P-value | 0.32 | 0.59 | ||
| PRO [gr] | Before | 118.9 ±18.4 | 115.7±16.4 | 0.74 |
| After | 125.5 ±19.7 | 117.7 ±17.2 | 0.20 | |
| P-value | 0.31 | 0.88 | ||
| Fat [gr] | Before | 111.6 ±30.1 | 99.2±14.9 | 0.11 |
| After | 114.7±32.2 | 105.4±18.8 | 0.29 | |
| P-value | 0.66 | 0.41 | ||
| SFA [gr] | Before | 28.4 ±9.9 | 28.1±8.3 | 0.91 |
| After | 29.5±10.8 | 29.0±8.2 | 0.87 | |
| P-value | 0.54 | 0.70 | ||
| Fiber [gr] | Before | 21.3 ±4.6 | 20.7±4.6 | 0.51 |
| After | 22.6±5.1 | 20.9±4.8 | 0.33 | |
| P-value | 0.21 | 0.93 | ||
| PAL [Met/h] | Before | 1.47 | 1.40 | 0.25 |
| After | 1.47 | 1.43 | 0.46 | |
| P-value | 0.78 | 0.12 | ||
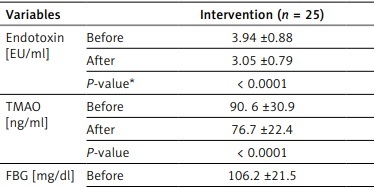
As shown in Table II, in the intervention group, the mean of serum endotoxin and TMAO significantly decreased after 12 weeks of supplementation. However, no significant differences were observed in the control group. Moreover, at the end of the study, a significant reduction was observed in FBG levels in the synbiotic group. Interestingly, Pearson’s coefficient correlation analysis showed a significant positive correlation between FBG changes with endotoxin and TMAO changes (Table III).
Table II
Serum endotoxin, TMA, and FBG levels before and after intervention
| Variables | Intervention (n = 25) | Placebo (n = 25) | P-value* | |
|---|---|---|---|---|
| Endotoxin [EU/ml] | Before | 3.94 ±0.88 | 3.56 ±1.02 | 0.16 |
| After | 3.05 ±0.79 | 3.64 ±0.83 | 0.012 | |
| P-value* | < 0.0001 | 0.66 | ||
| TMAO [ng/ml] | Before | 90. 6 ±30.9 | 91.1 ±24.7 | 0.90 |
| After | 76.7 ±22.4 | 87.5 ±26.5 | 0.12 | |
| P-value | < 0.0001 | 0.11 | ||
| FBG [mg/dl] | Before | 106.2 ±21.5 | 99.2 ±30.1 | 0.35 |
| After | 93.5 ±17.0 | 97.3 ±24.8 | 0.53 | |
| P-value | > 0.0001 | 0.26 | ||
Table III
Pearson’s correlation coefficients of changes in FBG with the changes in serum LPS and TMAO levels in the studied groups
| Parameter | Intervention | Placebo | ||
|---|---|---|---|---|
| P-value | r | P-value | r | |
| LPS | 0.041 | 0.41 | 0.41 | 0.17 |
| TMAO | 0.047 | 0.40 | 0.12 | 0.32 |
In this study, we did not observe any side effects of synbiotic supplementation in either group.
Discussion
To the best of our knowledge, this is the first study to evaluate the effect of synbiotic supplementation on serum levels of TMAO and endotoxin in patients with dyslipidaemia. In this randomized controlled trial, administration of a multi-species synbiotic supplement (containing a total dose of 3 × 1010 CFU probiotic microorganisms including 5 bacteria and one yeast species, and 5 g prebiotics) in patients with dyslipidaemia resulted in a significant decrease in serum endotoxin and TMAO in the intervention group. Moreover, our results showed a significant reduction in FBG levels in patients who received synbiotic supplements, and a significant positive correlation between FBG changes and serum endotoxin and TMAO changes.
Consistent with our results, Tenore et al. showed consumption of 125 g/day lacto-fermented Annurca apple puree for 16 weeks (each dose contained about 3 × 108 CFU L. rhamnosus LRH11 and L. plantarum SGL07) by individuals with CVD risk factors resulted in a decrease in TMAO level [28]. Moreover, Matsumoto et al. reported that supplementation with probiotic B. animalis subsp. Lactis LKM512 in healthy subjects could reduce TMA levels [29]. The results of another study by Moludi et al. showed that probiotic supplementation (containing 1.6 × 109 CFU of L. rhamnosus LGG) along with calorie restriction in patients suffering coronary artery disease for 12 weeks led to a significant decrease in IL-1β and endotoxin levels [30]. The findings of a study on psoriasis patients showed that supplementation with multi-strain probiotic capsules of at least 1.6 × 109 CFU/g of probiotics including L. acidophilus, B. bifidum, B. lactis, and B. langum for 8 weeks results in a significant reduction in serum endotoxin, hs-CRP, and IL-1β levels [31]. In contrast, other studies did not find any significant effect of probiotic/prebiotic supplementation on TMAO or endotoxin levels. Boutagy et al. reported that treatment with the multi-strain probiotic VSL#3 for 4 weeks in non-obese males did not influence plasma TMAO concentrations following a high-fat diet [32]. The finding of another study showed that supplementation with 3 × 109 CFU L. casei shirota for 3 months in patients with metabolic syndrome increased LPS-binding protein (LBP) levels [33]. Moreover, Tripolt et al. reported that treatment with 6.5 × 109 L. casei Shirota 3 times a day for 12 weeks did not decrease plasma levels of TMAO in patients with metabolic syndrome [34]. The inconsistency seen in the results of these studies could be explained by various dosages and species of probiotic microbes, the duration of the studies, the characteristics of participants, and various clinical settings [30].
Previous studies have shown that supplementation with the appropriate probiotic species or combination of probiotics can lead to modulation of the GM that in turn promotes the production of metabolites that can inhibit the TMAO synthesis pathway [35, 36]. It has been suggested that probiotics can produce bacteriocins that suppress pathogenic bacteria and modulate the anti-apoptotic and proliferation responses of intestinal epithelial cells [37, 38]. Furthermore, probiotics can protect intestinal epithelial cells from oxidative stress by secreting proteins that induce cytoprotective heat shock proteins [39].
The improvement in FBG levels following synbiotic supplementation is consistent with the known association between gut dysbiosis and metabolic disorders [40]. Recent research has suggested the role of dysbiosis in developing and progressing dyslipidaemia and related metabolic disorders [41]. Individuals with hyperlipidaemia showed an increase in serum levels of LPS and TMAO [42]. It is evident that synbiotics can lead to alterations in GM composition, favouring the growth of beneficial bacteria [43] and increasing the production of SCFAs [44]. SCFAs improve gut barrier function and reduce gut permeability, which can limit the entry of LPS into the bloodstream, thereby reducing low-grade inflammation and insulin resistance [45]. Furthermore, SCFAs can stimulate the release of incretin hormones, including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). These hormones play a crucial role in regulating blood glucose levels by promoting insulin secretion from pancreatic beta cells in response to elevated glucose levels. GLP-1 and GIP also inhibit glucagon release from pancreatic α cells, further contributing to glucose control [46].
We also found a positive correlation between changes in FBG and changes in endotoxin and TMAO levels. Aligned with our results, the study reported a positive correlation between serum endotoxin and FBG, and a negative association with serum HDL-C in patients with type 2 diabetes [47]. Our findings further support the potential interplay between GM and metabolic parameters. Our previous study showed that synbiotic supplementation significantly increased the abundance of beneficial gut bacteria and serum concentration of HDL-C in patients with dyslipidaemia [48]. The reduction in endotoxin, TMAO, and FBG levels following synbiotic supplementation suggests that targeting GM through synbiotic interventions could be a promising approach for managing dyslipidaemia and related metabolic disorders including insulin resistance.
Our study has several limitations. Firstly, the sample size was determined based on cholesterol parameters due to the limited existing studies on TMA and LPS at the time of study design. Secondly, only male patients were recruited, which limits the generalizability of our findings to the broader population. Lastly, we did not measure inflammatory biomarkers.
However, this study has some strengths. Firstly, it employed a rigorous randomized controlled trial design and was conducted on a homogeneous group of non-smoking men with similar lifestyles and ethnicities. Secondly, a high compliance rate was observed in participants who completed the 12-week study in both groups. Lastly, our study is the first to evaluate the effect of synbiotic supplementation on TMAO and LPS levels as novel biomarkers of CVD in patients diagnosed with dyslipidaemia.
In conclusion, the results of our study showed that a 12-week synbiotic supplementation in patients with dyslipidaemia resulted in significant reductions in serum endotoxin and TMAO levels, as well as improvements in FBG. Synbiotics might be a potential strategy for the management of metabolic disorders and the prevention of CVDs in adult men with dyslipidaemia. Future studies with larger and more diverse populations and a comprehensive assessment would be beneficial to further investigate the effects of synbiotic supplementation on metabolic status in patients with dyslipidaemia.