A left ventricular assist device (LVAD) can help as a bridge to heart transplantation. It is also a long-term solution for patients who are not candidates for a heart transplant. Recent data have shown that between 2008 and 2016, the use of LVADs in the United States increased almost threefold. This led to a remarkable drop in the in-hospital mortality rate, from 19.6% to 8.1% [1]. The use of LVADs has become more popular in high-volume centers as it requires a higher level of expertise and resources. Despite its significant benefits, patients undergoing LVAD implantation are at risk of numerous periprocedural adverse events, including stroke. In a recent meta-analysis, Llerena-Velastegui et al. estimated that LVAD patients face a 2.6 times higher risk of stroke. In addition, they were also more susceptible to bleeding, infection, and various arrhythmias [2]. Patients using LVADs thus require more vigilant management.
To date, there is a critical lack of large-scale studies evaluating the various risk factors for hemorrhagic or ischemic stroke among patients undergoing LVAD implantation. We conducted this retrospective study, leveraging nationally representative data, to identify the key risk factors of perioperative and early postoperative stroke following LVAD implantation. Our findings are intended to enhance risk stratification, which may help improve their outcomes.
We conducted a retrospective cohort study using data from the National Inpatient Sample (NIS), a publicly available database maintained by the Healthcare Cost and Utilization Project (HCUP). Adult patients (≥ 18 years) who underwent LVAD implantation between 2016 and 2021 at urban teaching hospitals (UTCs) were identified using relevant ICD-10 procedural codes. We then used ICD-10 codes to identify cases of ischemic and hemorrhagic strokes.
We analyzed a comprehensive set of patient-level data, including demographics, existing health conditions, and prior medical history. The primary outcomes were the occurrence of ischemic or hemorrhagic stroke during hospitalization. In-hospital mortality from any cause was assessed as a secondary outcome. To identify independent risk factors for each type of stroke and to examine their relationship with inpatient mortality, we used multivariable logistic regression models. Results were reported as adjusted odds ratios (aOR) with 95% confidence intervals (CI).
We used STATA 18.0 and R Studio to analyze the data. To protect patient privacy, we followed HCUP guidelines and did not report any results based on fewer than 11 cases. We applied discharge weights and made sure to adjust for the survey’s complex design, including how the data were grouped and sampled. Since the NIS database contains only de-identified information, our study did not require approval from an institutional review board (IRB).
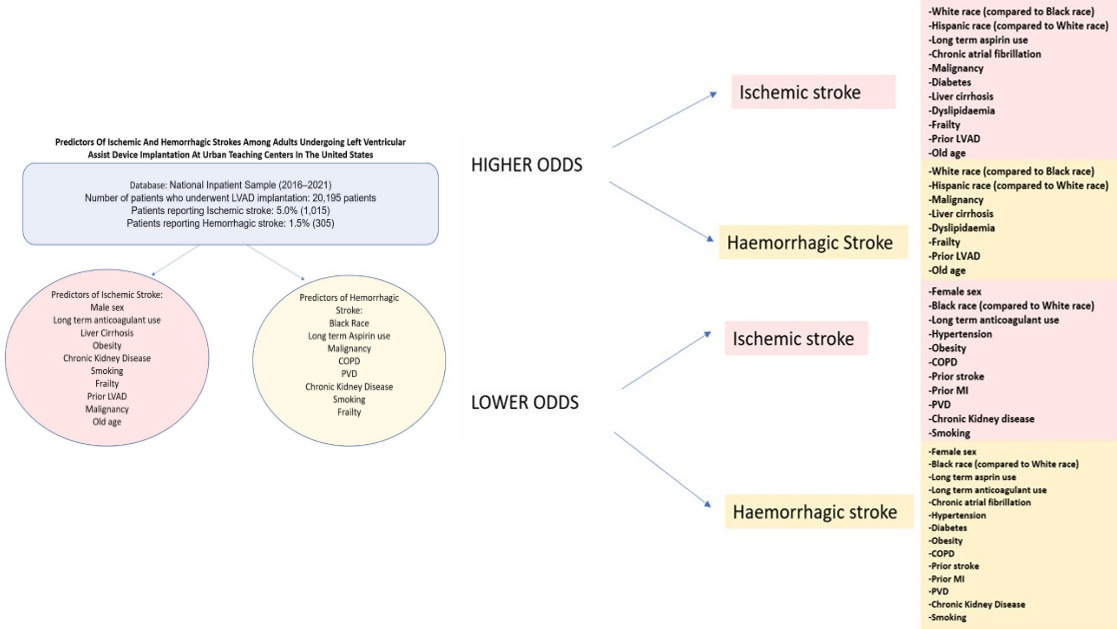
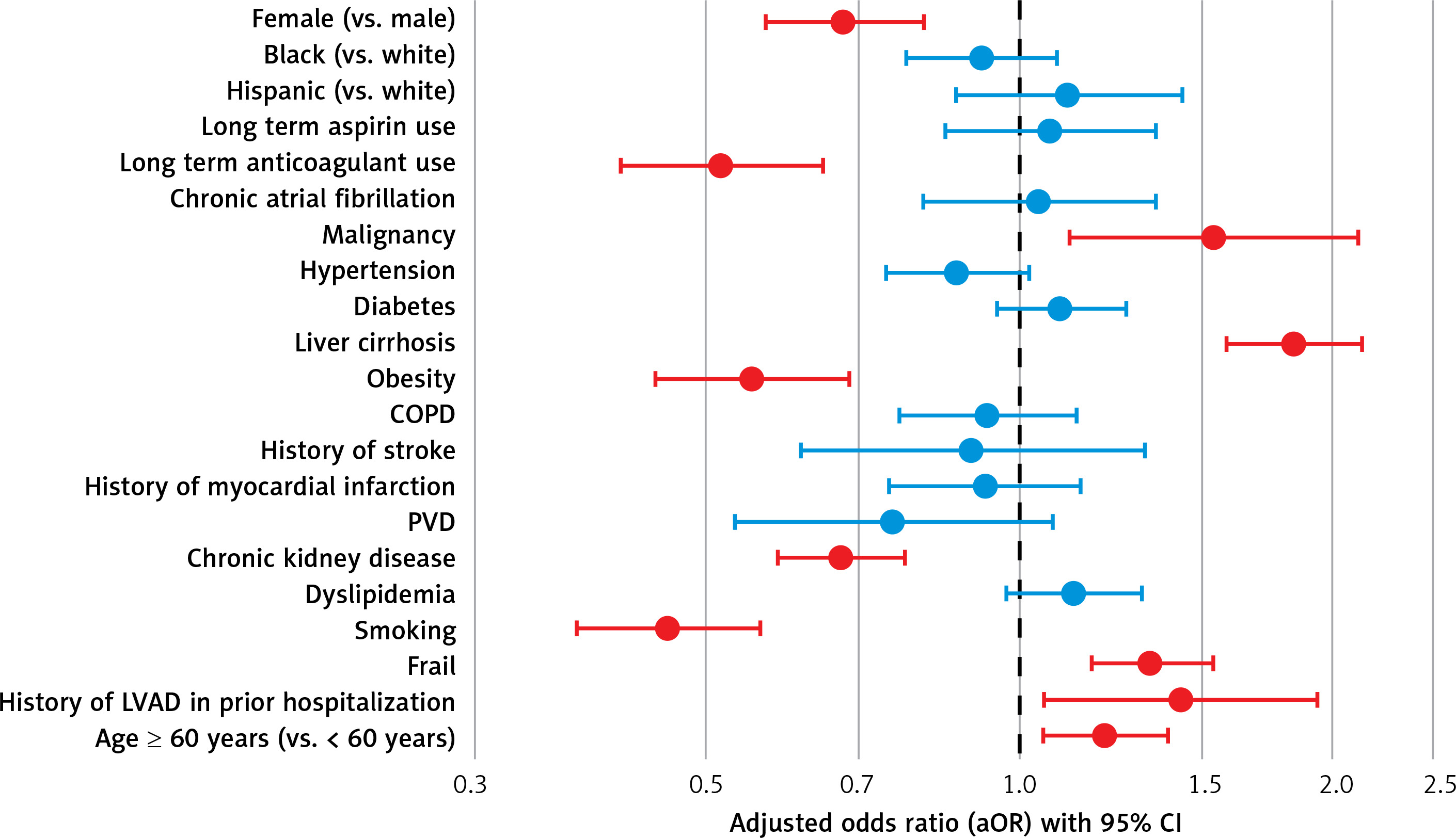
Our study included a total of 20,195 patients who underwent LVAD implantation at UTCs between 2016 and 2021. Among these, ischemic strokes occurred in 5.0% (1,015 patients), while hemorrhagic strokes were noted in 1.5% (305 patients). Females were significantly less likely to develop ischemic stroke compared to males (adjusted odds ratio [aOR] = 0.677, 95% confidence interval [CI]: 0.568–0.807, p < 0.001). Predictors of increased odds of ischemic strokes included malignancy (aOR = 1.537, p = 0.008), liver cirrhosis (aOR = 1.832, p < 0.001), frailty (aOR = 1.337, p < 0.001), prior LVAD hospitalization (aOR = 1.428, p = 0.02), and age ≥ 60 years (aOR = 1.208, p = 0.008). Conversely, long-term aspirin use (aOR = 0.516, p < 0.001), obesity (aOR = 0.553, p < 0.001), chronic kidney disease (aOR = 0.673, p < 0.001), and smoking (aOR = 0.459, p < 0.001) were less likely to predict ischemic stroke (Table I, Figure 1).
Table I
Predictors of ischemic stroke
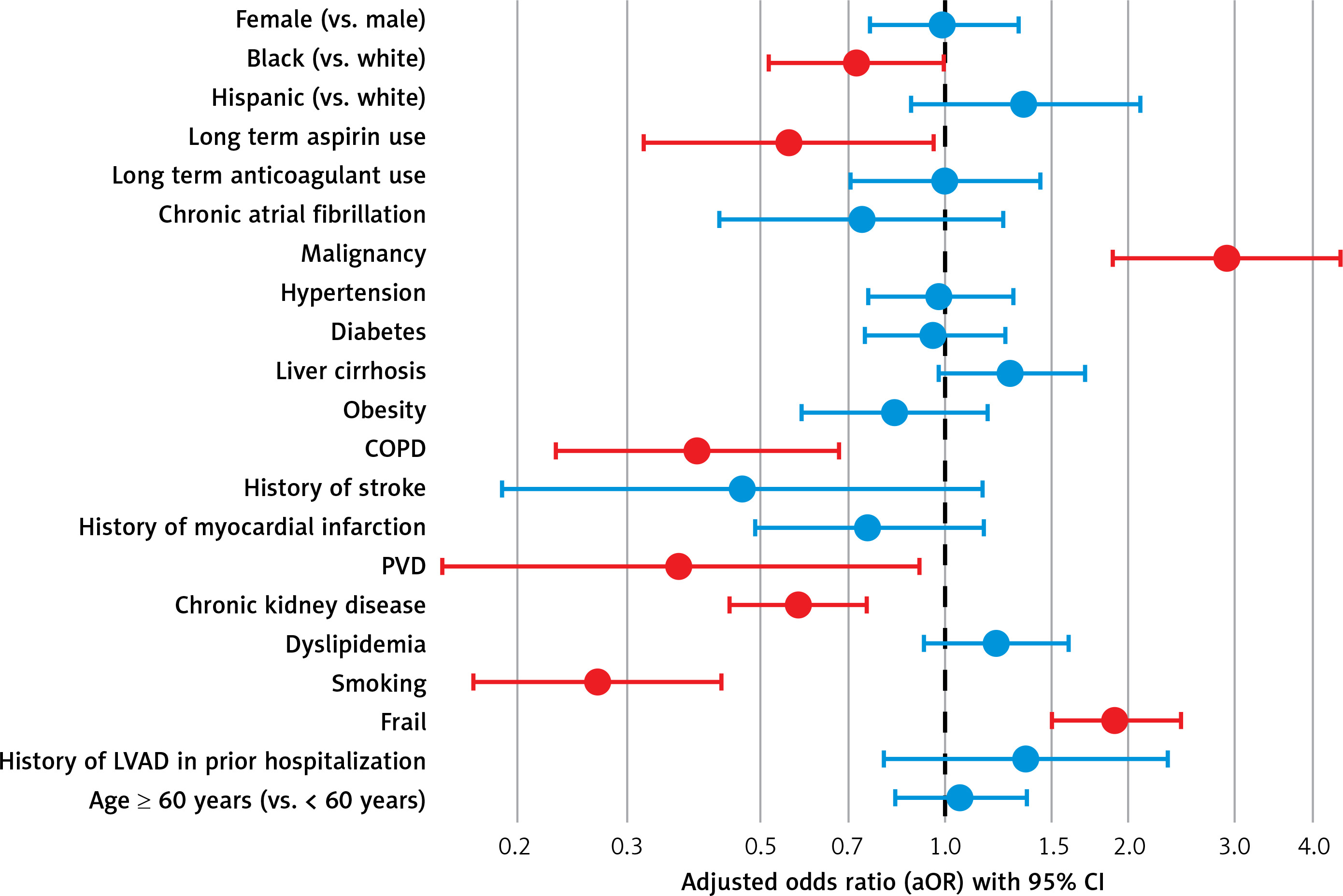
For hemorrhagic strokes, malignancy (aOR = 2.886, p < 0.001) and frailty (aOR = 1.896, p < 0.001) were associated with increased risk. In contrast, long-term aspirin use (aOR = 0.553, p = 0.033), chronic obstructive pulmonary disease (COPD) (aOR = 0.390, p < 0.001), peripheral vascular disease (aOR = 0.367, p = 0.029), chronic kidney disease (CKD) (aOR = 0.573, p < 0.001), and smoking (aOR = 0.269, p < 0.001) were associated with reduced odds. Notably, Black patients had significantly lower odds of hemorrhagic stroke compared to White patients (aOR = 0.713, p = 0.044) (Table II, Figure 2).
Table II
Predictors of hemorrhagic stroke
Both ischemic and hemorrhagic strokes were independently associated with an increase in in-hospital mortality. Patients with hemorrhagic stroke had increased odds of death (aOR = 13.487, 95% CI: 10.394–17.501, p < 0.01), followed by those with ischemic stroke (aOR = 3.990, 95% CI: 3.409–4.670, p < 0.01) (Table III).
Table III
Adjusted odds ratio of all-cause mortality among patients with either ischemic or hemorrhagic strokes
| Type of stroke | P-value | aOR | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|
| Hemorrhagic stroke | < 0.01 | 13.487 | 10.394 | 17.501 |
| Ischemic stroke | < 0.01 | 3.990 | 3.409 | 4.670 |
In our retrospective study of patients who underwent LVAD implantation at UTCs between 2016 and 2021, we observed lower rates of perioperative ischemic (5.0%) and hemorrhagic (1.5%) strokes compared to prior reports. For example, Flexman Yen et al. reported a 12.8% stroke rate among 172 LVAD recipients, with most events occurring within the first week after surgery [3]. Similarly, Molina et al., using data from the STS Intermacs National Database, reported a 5.9% stroke rate, with nearly half occurring within the first 7 days [4]. Tsiouris et al. reported a 13% rate, evenly divided between ischemic and hemorrhagic strokes [5]. Several factors may explain why our observed rates are lower. Our sample was drawn exclusively from UTCs, where standardized procedural protocols and advanced treatment strategies may have contributed to fewer complications. In addition, our study period, i.e., 2016 to 2021, coincides with the widespread use of newer generation assist devices, such as the HeartMate 3, which have demonstrated superior hemocompatibility and lower thrombotic risks. We also focused on in-hospital perioperative events, while the other studies in the literature included post-discharge and outpatient events. Moreover, differences in patient profiles between the various studies may also play a critical role; the earlier studies included a broader and higher-risk group of patients, such as the elderly, frail, or those undergoing re-do surgery. Our study relied on ICD-10 coding, which is vulnerable to miscoding and underdetection of less severe or transient neurological events.
Our multivariable analysis revealed several factors associated with increased odds of ischemic stroke. These included malignancy, liver cirrhosis, frailty, prior LVAD admission, and age ≥ 60 years. These conditions are known contributors to pro-thrombotic states and systemic vulnerability, which may exacerbate thromboembolic risks during the perioperative phase. Similar findings were reported by Izzy et al., who noted higher ischemic stroke risk among elderly and comorbid LVAD patients. The paradoxically lower association in patients with CKD and obesity may reflect more intensive monitoring or a more cautious approach to anticoagulation in these higher-risk groups [6]. In addition, the CKD patients selected for LVAD implantation may have been those who were in a more stable condition, as physicians likely weighed the risks and benefits when evaluating their preoperative eligibility. Unfortunately, data regarding their post-discharge complications are not covered by the NIS. This is an important limitation that can be addressed through more extensive studies in the future. We further found an inverse association between smoking and ischemic stroke. Similar inverse associations have been observed in prior cardiovascular studies. However, this may be linked to selection bias, with smokers representing a younger cohort, or to various confounders such as medication use or increased physician monitoring, which could affect the incidence of such adverse events.
For hemorrhagic strokes, malignancy and frailty were independently associated with elevated risk. Malignancy may contribute to platelet dysfunction or coagulopathy, while frailty reflects diminished physiological reserve and vulnerability to bleeding under surgical stress. Meanwhile, long-term aspirin use, COPD, peripheral vascular disease (PVD), CKD, and smoking were associated with lower odds of hemorrhagic stroke. These inverse associations, although counterintuitive, likely reflect clinical decision-making where antithrombotic therapy is tailored or restricted in high-risk groups. Van der Horst et al. suggested that careful risk assessment and anticoagulation adjustments could help reduce bleeding complications in frail or comorbid patients [7]. Thus, the strong association of hemorrhagic stroke and frailty calls for more careful perioperative planning in this patient population.
Our findings showed that in-hospital mortality was 13.5 times higher for patients who experienced a hemorrhagic stroke and about 4 times higher for those with an ischemic stroke, compared to patients without stroke. These mortality rates are notably higher than those reported in previous studies. For instance, Izzy et al. reported that stroke-related mortality was 2.5 times higher among LVAD patients [6], while Flexman et al. reported that in-hospital mortality rates were 2.9–3.1 times higher after stroke in the same population [3]. Our findings demonstrated a strong association between stroke type and in-hospital mortality. The greater mortality associated with hemorrhagic strokes, compared to ischemic strokes, is likely due to their more severe physiological impact. This disparity highlights the urgent need to focus on perioperative risk factors that may be underrecognized in the current LVAD stroke literature.
Our study has several limitations. First, since the NIS relies on administrative coding, there is a risk of misclassification or underreporting of diagnoses, which could introduce bias. Second, the dataset does not provide information on stroke timing, severity, or imaging confirmation, which limits clinical interpretation. Third, we were unable to assess long-term outcomes such as out-of-hospital mortality or stroke recurrence. Additionally, because the study population was limited to UTCs, the findings may not be generalizable to community or rural healthcare settings. Further prospective studies are needed to validate our results and to better understand long-term outcomes, including overall mortality.
Stroke remains a serious and relatively common complication following LVAD implantation. In our study, ischemic strokes were associated with a fourfold increase in the risk of in-hospital death, while hemorrhagic strokes were linked to a thirteenfold increase. Our analysis identified high-risk features that can help clinicians better stratify patients and provide more tailored perioperative care to reduce the likelihood of these devastating outcomes.