Open mitral valve repair (OMVR) is a well-established procedure for the management of mitral regurgitation. In the US, from 2014 to 2018, 165,405 mitral valve repair or replacement procedures were performed. Of these 86,488 were repairs (52.3%) [1]. 1061 procedures were performed in 2021/22 in the UK, with and without coronary artery bypass grafting (CABG), and the mortality rate for mitral valve repair alone was low at 1.1% for this period [2].
OMVR in octogenarians is less well researched, despite being associated with higher incidences of post-operative complications and peri-operative mortality than in younger patients [3]. However, evidence suggests that there is significant benefit for the elderly from such surgical procedures [4].
A previous study noted that renal impairment was strongly predictive of 30-day mortality in these patients, despite the choice of a procedure with lower risk than open surgery [4]. Acute kidney injury (AKI) following OMVR is a recognised complication [5]. AKI in octogenarians can carry significant risk to morbidity and mortality. The number of octogenarians being operated on has increased in recent years, and with an aging population, this is likely to rise. Identifying predictors for AKI in this patient population is of clinical use, to inform operative and peri-operative management, and this study aims to fill this void.
The study involved data taken from the National Inpatient Sample (NIS) database from the Healthcare Cost and Utilisation Project (HCUP) for hospitalisations between 1 January 2016 and 31 December 2020 [6]. The NIS is one of the largest public databases of hospitalised patients in the United States and currently encloses around 20% of all community hospital data, which can provide an estimate of 90% of the population. Due to the public nature of the databases, no consent was required.
Cases with a procedural code for OMVR as previously described by Ullah et al. were included [7]. Patients younger than 80 years and those older than 89 years were excluded. ICD-10 codes were applied, which identified several patient comorbidities and AKI based on past recommendations [8, 9].
For analysis, multivariable regression models were applied to estimate the various patient and hospital characteristics contributing to events of AKI. The results were expressed as adjusted odds ratios (aOR) along with their 95% confidence interval (95% CI) and their p-values. The statistical threshold was set at a p-value of less than 0.05 throughout the study. The analysis was performed using SPSS 29.0 (IBM Corp, Armonk, New York).
Between 2016 to 2020, an estimated 1120 procedures were performed among octogenarians in the United States, with 89.7% conducted in Urban teaching centres. Around 425 cases also resulted in AKI (37.9%). The baseline characteristics between AKI and non-AKI patients are given in Table I, with hypertension noted to be increased in patients with AKI as compared to without (34.5% vs. 18.8%; p < 0.01).
Table I
Characteristics of octogenarians with vs. without acute kidney injury
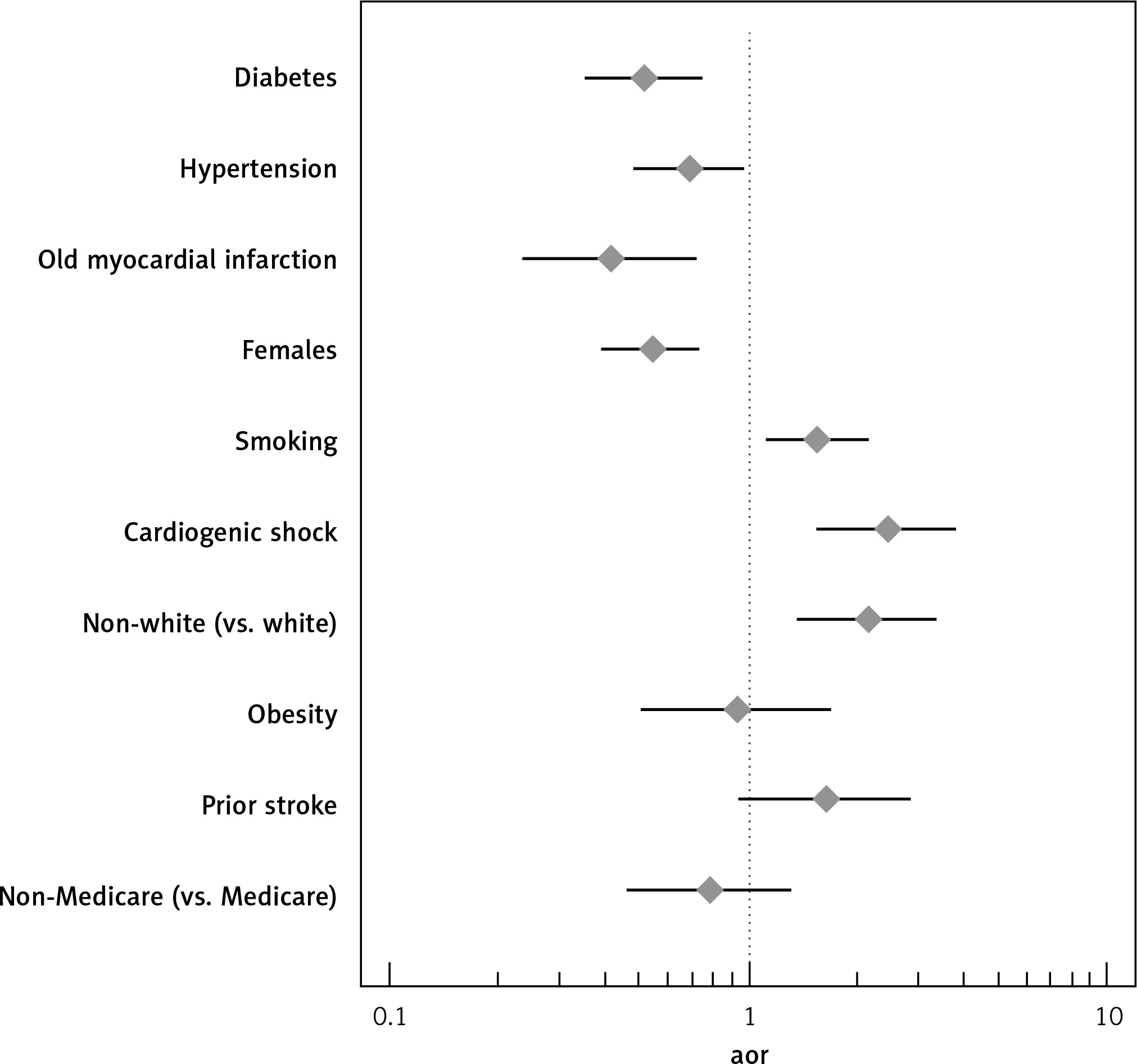
Lower odds of AKI were found among octogenarians who had diabetes (aOR = 0.515, 95% CI: 0.350–0.759), hypertension (aOR = 0.688, 95% CI: 0.480–0.986, p = 0.042), and a history of myocardial infarction (aOR = 0.416, 95% CI: 0.236–0.733, p < 0.01). In addition, the study demonstrated sex-based disparities, with females being less likely to experience AKI as compared to males (aOR = 0.539, 95% CI: 0.392–0.741, p < 0.01) (Table II).
Table II
Predictors of AKI in octogenarians undergoing open mitral valve repair
However, this study found higher odds of AKI among octogenarians who were smokers (aOR = 1.572, 95% CI: 1.123–2.199, p < 0.01) and patients who experienced cardiogenic shock (aOR = 2.472, 95% CI: 1.572–3.8886, p < 0.01). Racial disparities were also seen among non-Whites who showed higher odds of AKI (aOR = 2.162, 95% CI: 1.401–3.334, p < 0.01) (Figure 1).
Figure 1
Forest plot of adjusted odds ratio of predictors of AKI in octogenarians undergoing mitral valve repair
This study has found that octogenarians who were smokers, non-white, or with a history of concomitant cardiogenic shock were at higher risk of acute kidney injury in the post-operative period. Interestingly diabetes, hypertension, and a history of MI carried a lower risk of AKI in the post-operative period.
Current research notes that mitral valve repair outperforms replacement for postoperative mortality in the elderly, with minimally invasive surgeries gaining increased support as compared to the traditional sternotomy [10, 11]. Previous studies have noted that patients with diabetes and hypertension were at significantly higher risk for AKI after mitral valve surgery [4]. This differed from this study’s findings. One reason might be that, given their history, they were on adequate secondary prevention with ACE inhibitors, lifestyle changes, and closer surveillance, which may have reduced their risk of post-operative AKI. In the absence of this information being available, this explanation is at best a hypothesis. Previous literature has also noted significantly higher risk of AKI for patients with NYHA III and IV heart failure. This would align with the findings of the current study of higher risk in patients with cardiogenic shock [4, 12].
The incidence of AKI in the current study was 37.9%, which is slightly lower than in the report by Mao et al.’s, in which it was 46.8%; however, their data reported AKI in octogenarians after any cardiac valve surgery [13].
Smoking status has been linked to higher incidence of AKI post cardiac surgery [14]. Smoking has also been related to adverse renal function from previous research [15]. Multiple mechanisms have been linked to this. It may be related to smoking-induced proteinuria [16], and chronic nicotine exposure increasing enzyme activity related to oxidative stress in the kidneys [17]. Haemodynamic effects are noted, with nicotine increasing heart rate and blood pressure via sympathetic activity and vasopressin release [18]. This involves direct stimulation, by nicotine, of the adrenal medulla and peripheral sympathetic nerve endings.
There was a significantly higher risk of AKI in patients of non-white ancestry vs. white ancestry. Racial differences in rates of AKI have been seen in previous literature, with AKI significantly higher in the black ancestry population after cardiac surgery [19]. This may be related to higher incidences of hypertension and diabetes in these populations [18]. The findings here are hypothesis generating and warrant a thorough analysis of different ethnicities in a prospective study.
Patients with a history of cardiogenic shock have previously been demonstrated to have higher risks of short- and long-term mortality, and higher risks of readmission to hospital [20]. It is not surprising that these patients had a higher risk of AKI in the current study. Possible mechanisms may include higher risk of post-operative hypotension and continued endothelial dysfunction from previous events [21].
This current observational study had some limitations. It was a retrospective analysis of patients, the vast majority from urban teaching centres, which may not be representative of all octogenarians. Subgroups, for instance patients with cardiogenic shock, had small numbers and could not be further analysed. Findings of lower AKI rates in patients with diabetes and hypertension is discordant with expected results and may suggest that the sample size was too small. This analysis may be subject to confounding, for instance factors like surgical centre and intensity of post-operative monitoring could have influenced rates of AKI. Finally, the analysis also did not differentiate the level of AKI, for instance AKI stage 1 vs. stage 3.
In conclusion, nonetheless, it has been demonstrated that octogenarians with a history of smoking, who were male, or suffered previous cardiogenic shock were at higher risk of AKI after mitral valve surgery. Patients with diabetes, hypertension, or a history of MI had a lower risk of AKI. These findings are helpful to encourage closer patient monitoring post mitral valve surgery in higher-risk subgroups. Larger national and/or international reviews would be helpful also to collaborate the findings regarding low-risk subgroups.