
Introduction
Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system (CNS) characterized by demyelination and axonal degeneration resulting in significant neurological disability. According to the Atlas of MS, the global prevalence of the disease has risen, with 2.9 million people living with MS in 2023 [1, 2].
Symptoms among individuals with MS vary considerably. Most commonly, MS appears in its relapsing-remitting (RRMS) form, and it is usually followed by a state of continuous progression, i.e., secondary progressive MS (SPMS) [3]. Less frequently, patients present with the primary progressive (PPMS) type, whereby slow, progressive and persistent neurological impairment occurs [3]. The progressive phase is associated with great disability and limited response to treatment. Therefore, current available treatment aims at accelerating recovery after attacks, modifying disease progression, as well as managing symptoms [3].
Dyslipidemia and high-density lipoprotein cholesterol (HDL-C) level changes have been suggested to play a role in MS, although reports are inconclusive [4]; patients with MS exhibit altered lipoprotein levels (increased small HDL-C levels and oxidized low density lipoprotein (ox-LDL), larger triglyceride-rich very low-density lipoprotein) and function, which may increase cardiovascular disease risk, exert pro-inflammatory effects and, consequently, affect disease progression [5]. On the contrary, lipid-reducing treatments have been shown to impact the course of the disease [6, 7]. Pathophysiologically, it is not clear whether MS-related inflammation results from defective cholesterol metabolism or vice versa [4, 5].
The correlation between MS disease activity and lipid profile alterations has not yet been elucidated. This systematic review aims to assess the association between HDL-C and RRMS.
Material and methods
This systematic review has been registered in PROSPERO (ID number: CRD42023398000) and abides to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (PRISMA Statement, Ottawa, ON, Canada) [8].
The major objective was to evaluate the association between MS and HDL-C levels. Secondary outcomes included determination of the relationship between MS (RRMS type) and other lipoproteins, including low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and triglycerides (TGs).
Search strategy
A systematic literature search of English-only reports up to March 2023 was performed using Medline via PubMed, the Cochrane Controlled Trials Register and ClinicalTrials.gov databases. The following keyword combinations were used: (“High Density Lipoprotein Cholesterol” OR “HDL”) AND (“Multiple Sclerosis”). No year- or country-related restriction was imposed. References of included studies were examined for articles potentially missed by the initial database search. Abstracts from major scientific meetings were electronically searched (American Academy of Neurology Annual Meeting and the European Academy of Neurology conference).
Study design
A qualitative and quantitative synthesis of prospective and retrospective studies was performed in order to examine the role of HDL-C levels and other lipid profile constituents (LDL-C, TC, TGs) in MS.
Screening and eligibility
For deduplication purposes, Zotero reference management software was used. The potentially eligible studies were reviewed by two independent authors (NP and APA). Disagreements were discussed and consensus was reached. Eligibility criteria adhered to the PICOS (population, intervention, comparators/controls, outcomes, and study design) structure for research question wording, as follows population: patients with MS diagnosed using McDonald Criteria; intervention: measurement of lipid levels in RRMS patients; comparator: healthy participants; outcomes: mean differences of HDL-C and other lipid parameters between RRMS patients and healthy participants; study design: prospective or retrospective case-control studies. Studies not fulfilling the above criteria were excluded.
Data extraction
The extraction process for study characteristics was performed independently by two authors (NP and APA). First author, year of publication, country of origin, date of patient enrolment, and mean HDL-C concentration were recorded from each eligible study. Additionally, the following parameters were recorded for both MS patients and healthy controls (HC): gender, mean age, mean EDSS, percentage of patients with each disease type (RRMS, PMS, PPMS, and SPMS), as well as LDL-C, TC, and TG levels.
Methodological assessment of included studies
The Newcastle-Ottawa Scale (NOS) for case-control studies (CCS) was used for quality assessment purposes in each included study [9]. NOS encompasses three main categories, i.e. selection, comparability, and exposure, with the first two being divided into subcategories. A maximum score of 9 can be given to each study. A score of 7–9 is indicative of high-quality studies, a score of 4–6 denotes a high risk of bias, while a score of 0–3 indicates a very high risk of bias [9].
Statistical analysis and heterogeneity
When there were sufficient data and outcome measures were comparable, a quantitative analysis was performed. The pooled estimates were reported as continuous. Mean differences (MD) and 95 percent confidence intervals (CI) were determined for the continuous data. Where interquartile ranges were given for lipoproteins, a conversion to sample means and standard deviations was processed via the Box-Cox method by McGrath et al. [10]. Additionally, where data on standard error (SE) were available, standard deviation (SD) was obtained from the SE of a mean by multiplying by the sample size square root. Review Manager (RevMan) version 5.0 software was used for statistical analysis (The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark, 2008). A level of p-value < 0.05 was deemed as statistically significant. Heterogeneity of included studies was evaluated using the I2 test. A result of < 25%, 25–75%, or > 75% in the I2 test indicates low, moderate or high heterogeneity, respectively. The present meta-analysis used a random effects model for moderate or high I2.
Results
Eligible studies
Of the total 128 screened articles, we identified 13 eligible studies which fulfilled the inclusion criteria [11–23]. A PRISMA flowchart showing the study selection process was created (Figure 1). Excluded studies together with the reasons for exclusion, are shown in Table I [5, 24–32].
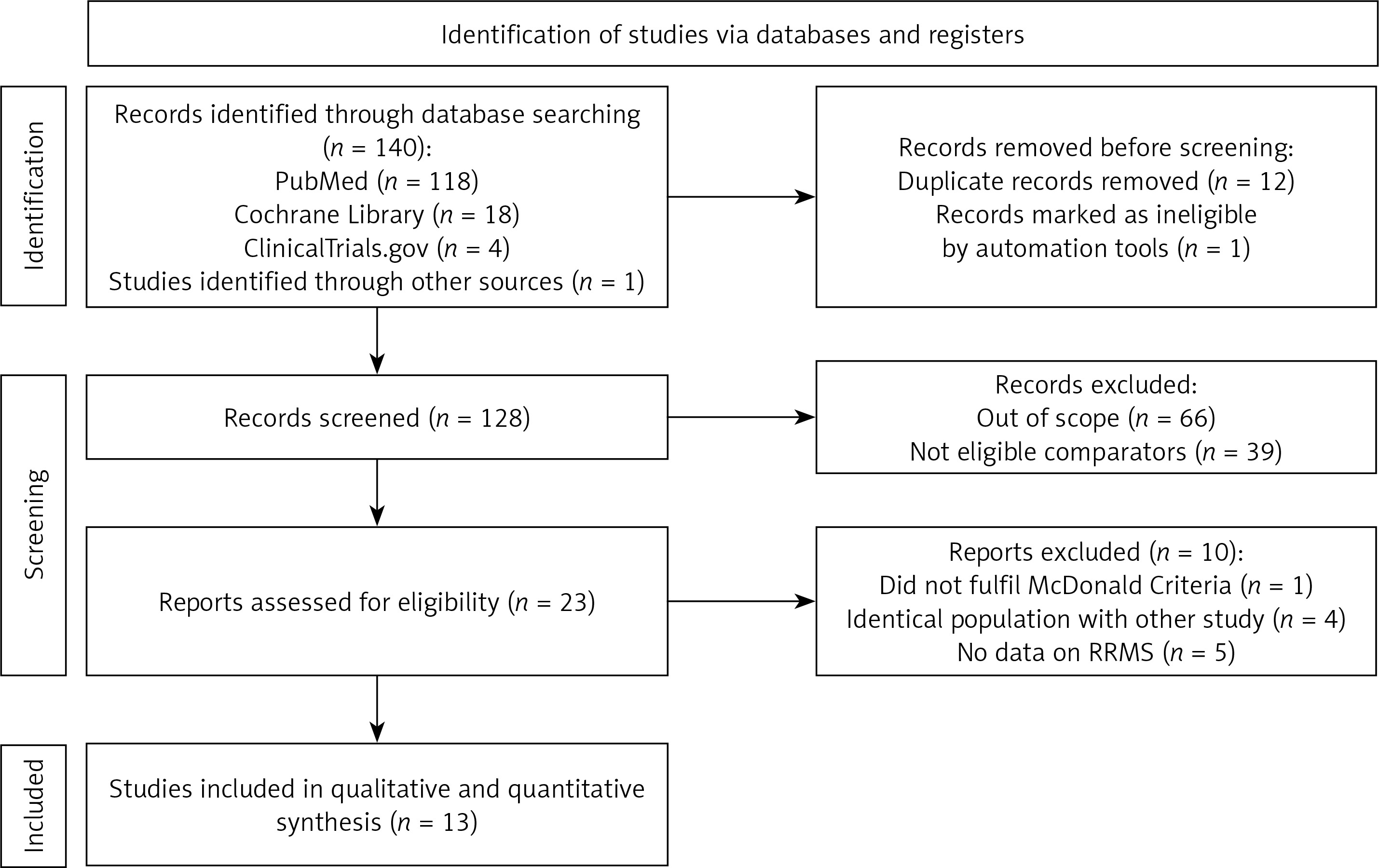
Table I
Excluded studies with reasons for exclusion
| Author | Year | Country | Study type/design | Reason for exclusion |
|---|---|---|---|---|
| F. Giubilei [24] | 2002 | Italy | CCS | Mc Donald’s criteria for diagnosis not fulfilled (WP) |
| G. Salemi [25] | 2010 | Italy | CCS | Not only RRMS (WP) |
| C. Keytsman [26] | 2017 | Belgium | CCS | Not only RRMS (WP) |
| Z. Radikova [27 | 2018 | Slovakia | CCS | Same study population as in Ďurfinová 2018 [19] (WP) |
| N. Murali [28] | 2020 | New York | CCS | Same study population as in Mukhopadhyay 2016 [17] (WP) |
| Ž. Rádiková [29] | 2020 | Slovakia | CCS | Same study population as in Ďurfinová 2018 [19] (WP) |
| E.K. Ulusoy [30] | 2020 | Turkey | CCS | Not only RRMS (WP) |
| L.S. Albuquerque [5] | 2021 | Brazil | CCS | Not only RRMS (WP) |
| I. Nieste [31] | 2022 | Belgium | CCS & CSS | Not only RRMS (WP) |
| K. Siddiqui [32] | 2023 | New York | CCS & CSS | Same study population as in Jakimovski 2020 [21] (WP) |
Characteristics of included studies
Table II presents the characteristics of the 13 studies which met the aforementioned eligibility criteria. In total, 1692 participants were included, 819 of which were RRMS patients, and the rest were HC. All 13 studies were published between 2005 and 2022. Two studies were conducted in the USA, 2 were conducted in Slovakia and the remaining ones were conducted in Italy, Poland, China, Iran, Portugal, Belgium, the UK, Turkey, and Egypt. From the included studies, HDL-C values of patients with MS ranged from 39.8 to 67.0 mg/dl, while HDL-C levels of HC ranged between 43.7 and 68.7 mg/dl.
Table II
Characteristics of the included studies
| Study | Year | Country | Study design | RRMS patients | Healthy controls | HDL-C [mg/dl] mean ± SD | |||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean age | HDL-C [mg/dl] mean ± SD | N | Mean age | |||||
| Ferretti [11] | 2005 | Italy | CCS | 24 | 38.2 | 50.3 ±3.6 | 89 | 31.5 | 58.3 ±3.0 |
| Jamroz-Wisniewska [12] | 2009 | Poland | CCS | 82 | 32.6 | 61.0 ±19.0 | 40 | 36.3 | 58.0 ±23.0 |
| Li [13] | 2010 | China | CCS | 53 | 36.9 | 51.0 ±14.7 | 54 | 36.5 | 51.0 ±10.8 |
| Moghtaderi [14] | 2011 | Iran | CCS | 63 | 32.3 | 39.8 ±8.7 | 63 | 42.3 | 43.7 ±6.7 |
| Palavra [15] | 2013 | Portugal | CS | 30 | 35 | 57.8 ±10.9 | 66 | 35.5 | 60 ±19 |
| Penesova [16] | 2015 | Slovakia | CCS | 19 | 30 | 57.2 ±13.5 | 19 | 29 | 53.0 ±15.9 |
| Mukhopadhyay [17] | 2016 | New York | CS | 221 | 44.4 | 66.8 ±14.0 | 203 | 45.6 | 68.7 ±16.0 |
| Jorissen [18] | 2017 | Belgium | CCS | 36 | 42 | 59.3 ±12.4 | 89 | 42 | 61.0 ±16 |
| Ďurfinová [19] | 2018 | Slovakia | CCS | 139 | 36 | 59.3 ±16.2 | 38 | 38 | 67.2 ±22.1 |
| Gafson [20] | 2018 | UK | CCS | 27 | 41.4 | 67.0 ±16.2 | 31 | 30.4 | 67.6 ±16.4 |
| Jakimovski [21] | 2020 | New York | Cohort | 64 | 50.1 | 58.8 ±13.0 | 41 | 50.4 | 59.3 ±17.0 |
| Gezmis [22] | 2021 | Turkey | CCS | 51 | 36.6 | 48.7 ±12.7 | 50 | 33.4 | 64.0 ±19.0 |
| Boshra [23] | 2022 | Egypt | CCS | 50 | 32 | 47.0 ±6.3 | 50 | 29 | 49.8 ±3.5 |
Study outcomes
High-density lipoprotein cholesterol
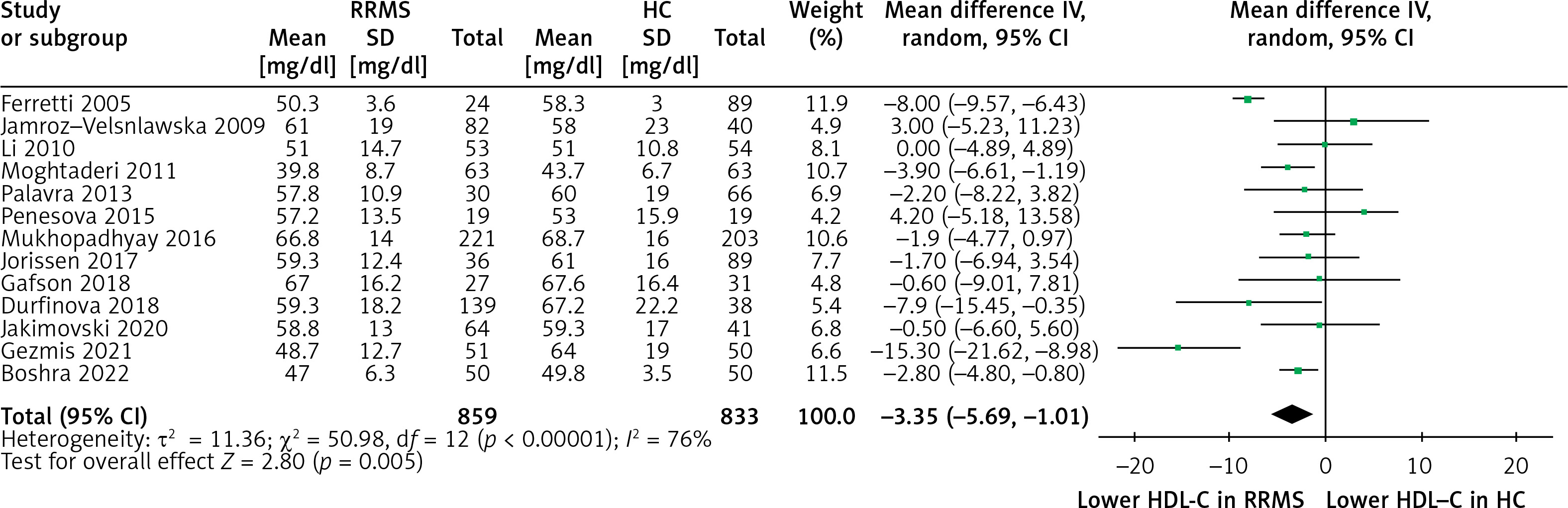
Our meta-analysis included data from 859 RRMS and 833 HC from 13 studies. Pooled results showed statistically significant differences between RRMS versus HC regarding HDL-C (MD = –3.35 mg/dl, 95% CI: (–5.69, –1.01), p = 0.005, I2 = 76%) (Figure 2).
Low-density lipoprotein cholesterol and total cholesterol
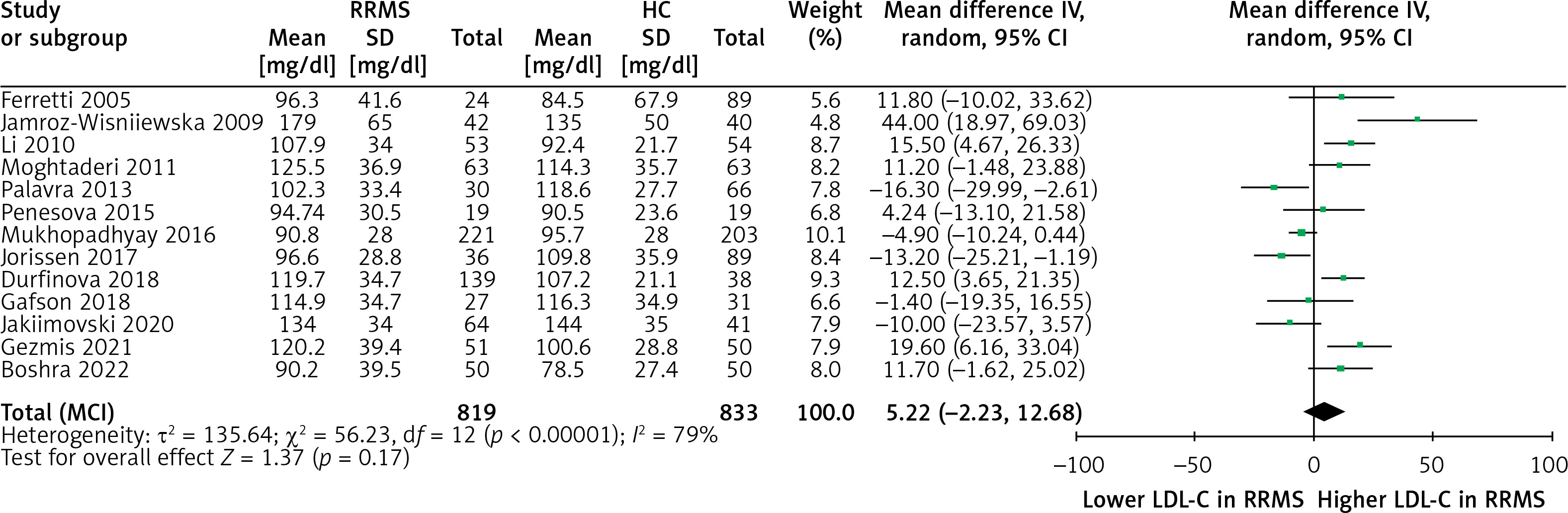
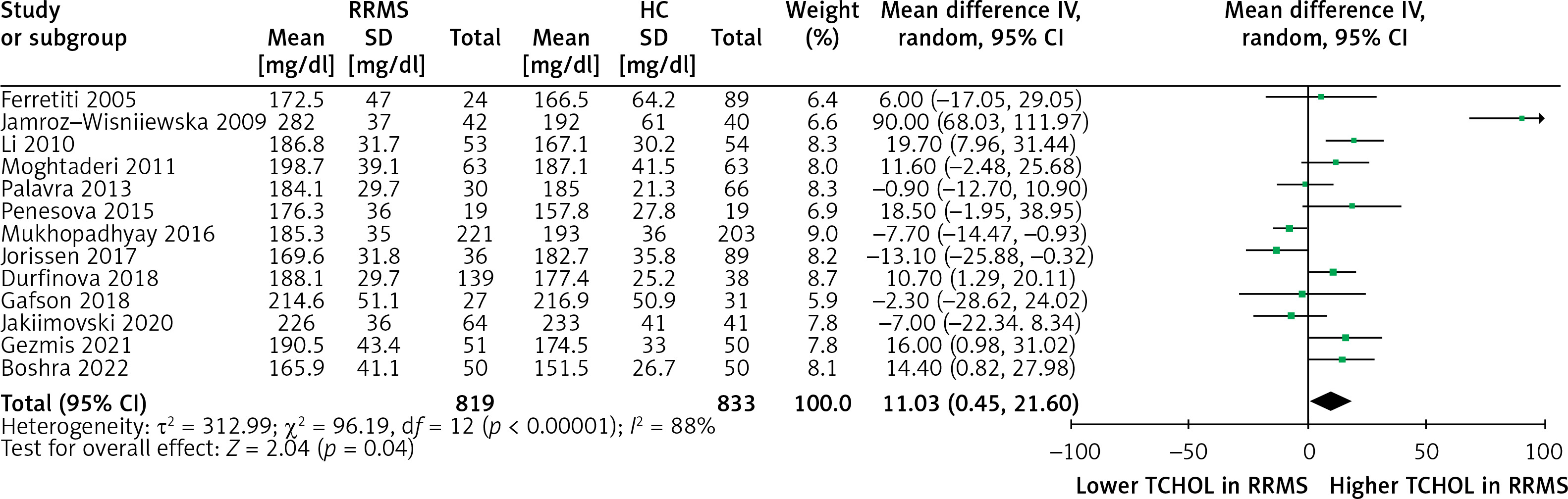
Regarding the secondary outcome of LDL-C, a non-significant higher LDL-C concentration in the RRMS population compared with that of the HC group (MD = 5.22, 95% CI: (–2.23, 12.68), p = 0.17, I2 = 79%) was observed (Figure 3). Regarding TC levels, the RRMS group exhibited slightly significantly higher concentrations compared to the HC group (MD = 11.03, 95% CI: (0.45, 21.60), p = 0.04, I2 = 88%) (Figure 4).
Triglycerides
Subgroup meta-analysis was also performed among RRMS and HC regarding TG levels for 534 RRMS and 589 HC from 11 studies. Pooled results showed significant differences between RRMS and HC in terms of TGs (MD = 26.33, 95% CI [15.03, 37.62], I2 = 62%) (Figure 5).
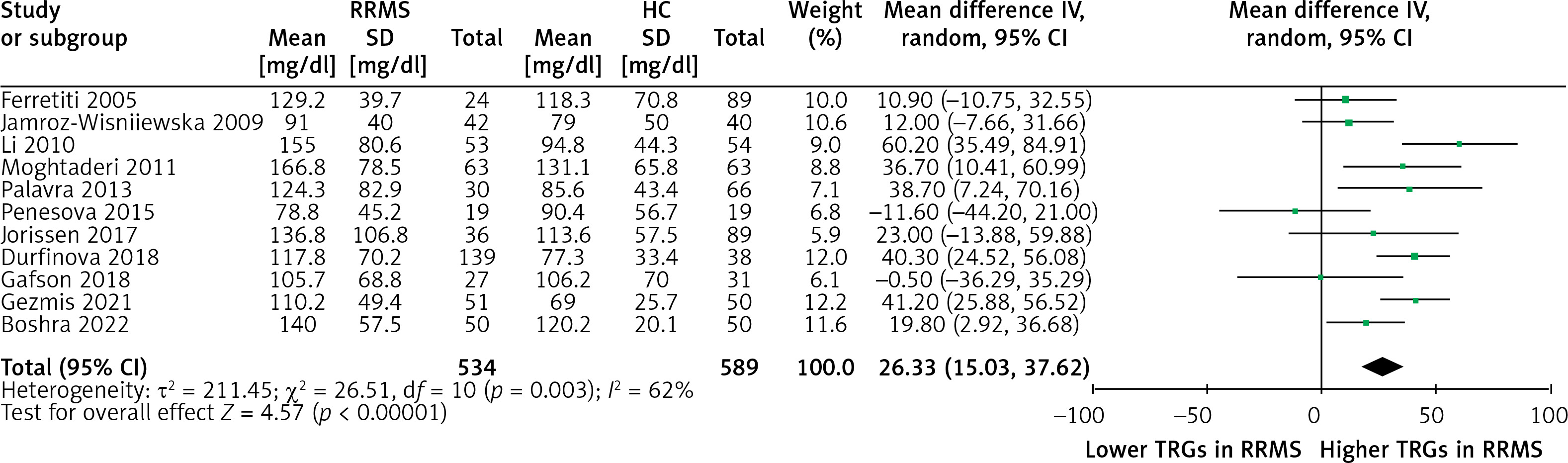
Concerning the study by Jamroz-Wisniewska et al. [12], lipid profile values used in the meta-analysis referred to RRMS patients in remission.
Quality appraisal
From the quality assessment of the 13 included studies using the NOS, the mean score was 8.4 points (8 studies with 9 points; 3 studies with 8 points; 2 studies with 7 points). Based on the aforementioned scoring system, this result indicates an overall high quality of included studies (Table III).
Table III
Quality appraisal of the included studies using the Newcastle-Ottawa Scale (NOS) for case-control studies
Discussion
The present systematic review and meta-analysis investigates the link between HDL-C levels and MS. Our results suggest that patients with RRMS have significantly lower HDL-C levels when compared with HC. Regarding the rest of the lipid profile parameters, TG and TC were higher in RRMS patients, while only LDL-C did not differ significantly between RRMS patients and HC.
Importantly, some of the included studies [19, 20, 23] investigated the correlation between lipoprotein levels and cholesterol subfractions with MS disability status, concluding that altered lipid metabolism may contribute to immune activation and, consequently, clinical deterioration. Of importance, in the study by Jakimovski et al. [21], MS patients with higher lipoprotein(a) [Lp(a)] levels (≥ 30 and ≥ 50 mg/dl) had significantly larger major extracranial arteries when compared with those with lower Lp(a) levels. According to recent guidelines, Lp(a) is a new atherosclerotic cardiovascular disease (ASCVD) factor, and every individual should have it measured once in their lifetime [33, 34].
Pathophysiology
In general, cholesterol is important for the cell membrane structure and function. As mentioned previously, it remains unclear whether MS-related inflammation is a consequence of dyslipidemia or vice versa [4, 5].
HDL-C is hypothesized to have a neuroprotective role in MS as a modulator of blood-brain barrier (BBB) breakdown [35]. The BBB protects the brain from potentially harmful blood-borne factors, which may induce inflammation and neurodegeneration [3, 36]. Therefore, low HDL-C concentrations promote BBB breakdown, allowing passage of pro-inflammatory cytokines and chemokines into the CNS, with subsequent attraction of leukocytes. This inflammatory state leads to demyelination characterized by oligodendrocytes loss, gliosis, and neuro-axonal degeneration [35].
On the other hand, the chronic inflammation seen in MS may contribute to the observed low HDL-C levels. Potential mechanisms contributing to this association include the inflammation-induced suppression of liver-derived apoA-I, the increments in secretory phospholipase A2 and endothelial cell lipase, the effect of cytokines, and the dysfunction of Lecithin:cholesterol acyltransferase [37]. The above HDL-reducing mechanisms have also been shown to contribute in other infectious and inflammatory conditions like leishmania and SARS-CoV-2 infections [38–41], as well as malignancies such as multiple myeloma [38, 42].
Multiple sclerosis and atherosclerotic cardiovascular disease
The pooled analysis findings of lower HDL-C levels and higher TC and TG levels in RRMS individuals suggest that such patients may also have a higher ASCVD burden [43].
Recent data indicate an increased ASCVD risk in MS patients. In a population-based matched cohort study of 84,823 people, 12,251 of which had MS, it was shown that MS was correlated with a 47% increased risk of ASCVD, as well as with a 59% increased risk of cerebrovascular disease [44]. Interestingly, statin treatment was associated with lower mortality rates among MS patients [44]. A randomized, double-blind, phase II trial demonstrated that high doses of simvastatin (80 mg/day) resulted in brain atrophy delay in SPMS patients when compared to those receiving placebo, indicating an additional beneficial effect of hypolipidemic treatment apart from ASCVD reduction [45]. Similarly, in a Mendelian randomization study including 115,803 individuals, the authors provided genetic evidence for the causal associations of MS with the increased risk of coronary artery disease, myocardial infarction, heart failure, and ischemic stroke. Finally, a recent Danish cohort study demonstrated an increased risk of ASCVD in patients with MS treated with fingolimod, attributing this finding to hypertension [46].
Limitations
To our knowledge, this is the first systematic review investigating the association between lipid profile parameters and MS. However, several limitations must be considered when interpreting the results presented herein. The small sample size and the retrospective, observational design of most studies increased the risk that observations could be due to chance. Moreover, our meta-analysis suffers from relatively high heterogeneity, as indicated by the I2 tool (76%, 79%, 88% and 62% for HDL-C, LDL-C, TC, and TGs, respectively, for the comparison of RMMS with HC). This may be potentially explained by discrepancies in lipoprotein measurement, as well as by patient-to-patient variability concerning MS type, disease activity, and treatment status. A meta-analysis comparing HDL-C levels between RRMS patients in remission versus PMS patients was not feasible due to insufficient data. Not all studies reported on potentially confounding comorbidities (e.g. disorders of lipid metabolism, diabetes, alcohol use disorder, thyroid, liver or renal disease), use of lipid-lowering agents or steroids, while anthropometric measurements were largely similar between groups. However, one study included patients with thyroid disorders [20], while 2 other studies included patients who received statins [15, 21]. Finally, reported mean BMI of either group was > 25 in 3 studies [17, 21, 23]. Data on physical activity were scarcely provided. The present meta-analysis focuses on RRMS patients, which also poses limitations regarding generalizability.
In conclusion, our meta-analysis suggests that RRMS patients have significantly lower HDL-C levels compared with HC. Lipid profile assessment is suggested in MS patients both as a potential biomarker of the disease, but also for ASCVD prevention purposes. Future MS research may be directed toward investigating the role of lipids as MS biomarkers, as well as potential indicators of disease burden and treatment response.