Cardiovascular disease (CVD) is the leading cause of death and disability in the United States (US) and worldwide. The Global Burden of Disease (GBD) study in 2019 showed that total incidence of cardiovascular disease doubled from 271 million in 1990 to 523 million in 2019, and the number of cardiovascular deaths steadily increased from 12.1 million in 1990, reaching 18.6 million in 2019, representing approximately 32% of all worldwide deaths. Of these deaths, 85% were due to heart attack and stroke. Out of 17 million premature deaths (under the age of 70) due to non-communicable diseases in 2019, 38% were caused by CVD [1, 2]. If current trends persist, experts predict over 23 million people will die from CVD in 2030 [3].
Modifiable risk factors for primary and secondary prevention of deaths due to CVD include hypertension, high blood cholesterol levels, smoking, diabetes, obesity, sedentary lifestyle, unhealthy diet, and stress. Conventional risk factors include advancing age, male sex, family history, and race. Although clinical signs of CVD are usually present in adulthood, early atherosclerotic changes can begin to occur early in life and through adolescence [4]. The prevalence of modifiable CVD risk factors can initiate early onset of atherosclerosis. Modifiable risk factors for CVD identified in adolescents, show that early intervention programs have potential to reduce CVD risk on individual and population levels. The existing evidence indicates that primary prevention of atherosclerotic disease should begin in childhood [5]. Identification of children at risk for atherosclerosis may allow early intervention to decrease the atherosclerotic process, thereby preventing or delaying CVD [4, 6]. The prevention of CVD in adolescents is critical to preventing premature death from CVD in adults and should be a focus for health professionals and policy makers. Past studies have demonstrated a rise in sedentary lifestyles and other modifiable risk factors among adolescents [7]. We aim to provide an up-to-date representation of the prevalence of multiple cardiovascular risk factors amongst adolescents in the US.
Hospitalization records of adolescents, aged 10–19 years (inclusive), were interrogated from the 2016–2020 National Inpatient Sample, a set of de-identified records provided by HCUP, AHRQ, and partners. We applied the International Classification of Diseases 10th Revision (ICD-10) codes to identify the co-existence of prediabetes, hypertension, diabetes, obesity, smoking, and a family history of ischemic heart disease (IHD) or CVD [8, 9]. Their presence was reported per 100,000 hospitalizations (number of cases with a particular variable divided by the total number of patients, multiplied by 100,000). Since the ICD-10 code for prediabetes was introduced in 2016, and it did not cover all the months of that particular year, we focused on the 2017–2020 data for our prediabetes group. We also estimated the incidence of acute myocardial infarction (AMI) and acute ischemic stroke (AIS) over these 5 years [10, 11]. Linear-by-linear analyses, as per past studies of the NIS, were used to estimate trends [12].
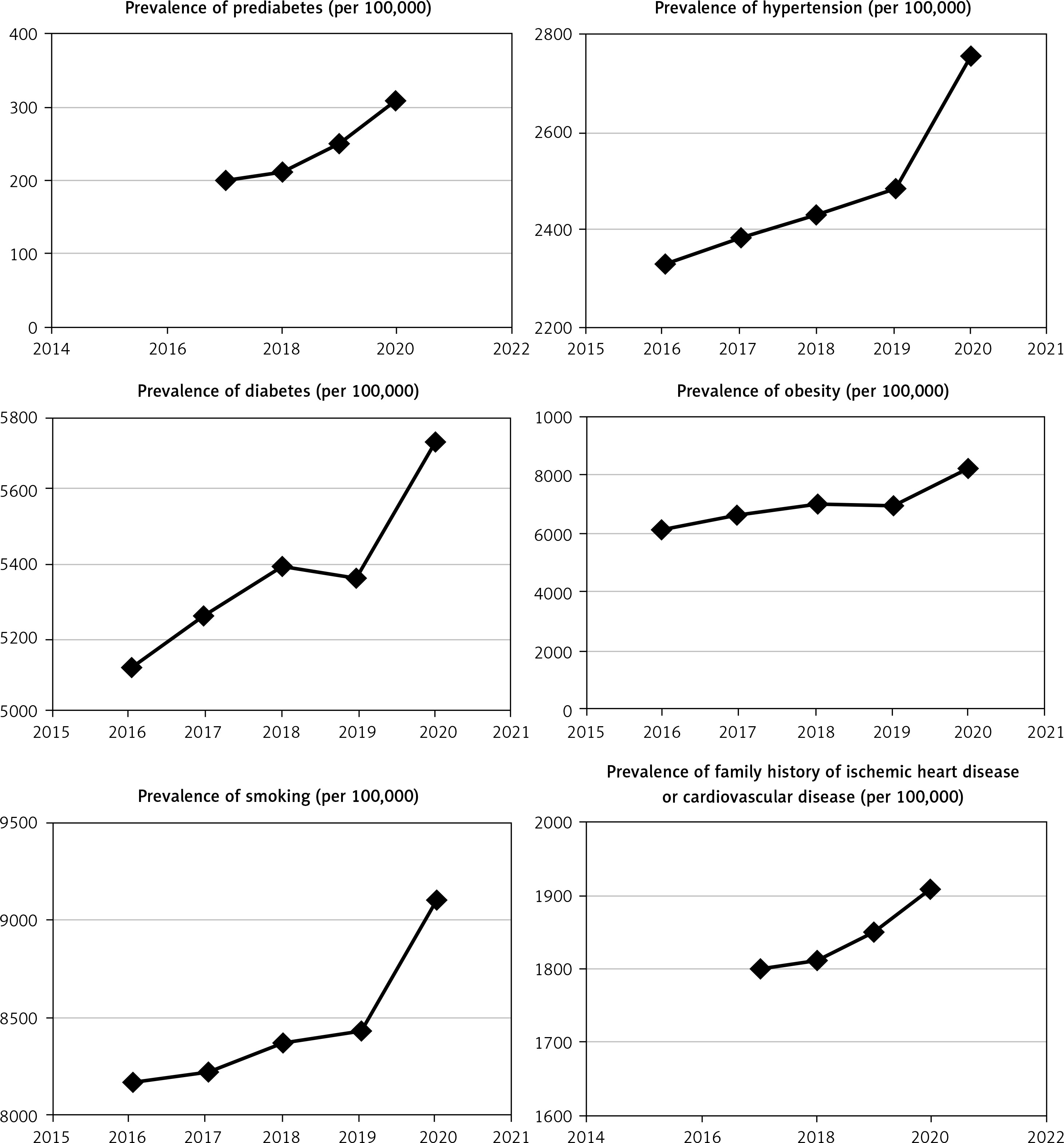
Our study found that the number of adolescents with prediabetes has increased from 199 per 100,000 in 2017 to reach 309 per 100,000 in 2020. Similarly, we also found an increasing trend in hypertension (2334 per 100,000 in 2016 to reach 2756 per 100,000 in 2020, ptrend < 0.01), diabetes (5119 per 100,000 in 2016 to reach 5733 per 100,000 in 2020, ptrend < 0.01), obesity (6153 per 100,000 in 2016 to reach 8221 per 100,000 in 2020, ptrend < 0.01), smoking (8166 per 100,000 in 2016 to reach 9117 per 100,000 in 2020, ptrend < 0.01), and family history of ischemic heart disease or cardiovascular disease (1687 per 100,000 in 2016 to reach 1922 per 100,000 in 2020, ptrend < 0.01, ptrend < 0.01) (Figure 1). In addition, the incidence of AMI rose from 34 per 100,000 in 2016 to reach 68 per 100,000 in 2020 (ptrend < 0.01). A similar rise in events of AIS was seen with 123 cases per 100,000 reported in 2016, and this increased to 156 per 100,000 in 2020 (ptrend < 0.01) (Figure 1).
Figure 1
Trends in risk factors (per 100,000) for cardiovascular disease among adolescents in the United States between 2016–2020
Our findings, involving the largest national in-patient database from the US, bring forward several critical results and potential correlations. As previously reported, we were able to confirm the rising prevalence of prediabetes [13], hypertension [14], diabetes [15], obesity [16], and smoking [17] among adolescents. In addition, while there is paucity of data on trends in AMI in that particular age group, our analysis confirms a rising trend that may correlate with the rise of multiple risk factors [5], which were also seen in our sample. The incidence of AMI almost doubled among adolescents during this period, along with an increase in the incidence of AIS. Our data identified potentially higher risk patients in hospitalised population and we acknowledge that this is not the normal population but we need to target those at the highest risk.
Without appropriate measures, these trends in CVD-associated morbidity and mortality will continue to rise over the coming years [18]. Early introduction of primary, secondary and tertiary prevention measures and intervention strategies including both pharmacologic and non-pharmacologic approaches are essential to reduce the risk by managing modifiable risk factors [19]. The potential association we talk about is thus far based in those deemed higher risk due to hospitalised in-patient data, So we at present cannot generalise to the more general population until more controlled, randomised studies are conducted. We therefore encourage broader and longer studies to improve our understanding and confirm the potential association.
In conclusion, this study not only showed a rise in various risk factors associated with future cardiovascular disease among adolescents in the selected inpatient population, with a worrying rise in AMI and AIS but also highlights an area of potential research to apply to the more general population. Stronger health-related sensitization campaigns promoting healthier lifestyles should be prioritized. The use of social media and influencers, which may have a better appeal to adolescents, should also be considered [20]. The urgent need to screen and treat the at-risk groups will help reduce the impending burden on individuals, their carers and healthcare providers [13, 18].