Introduction
Breast cancer remains the most common malignancy in women worldwide [1], with prognosis influenced not only by tumor-intrinsic factors but also by the tumor microenvironment [2]. Adipokines – bioactive proteins secreted by adipose tissue – play a central role in tumor biology, influencing proliferation, invasion, angiogenesis, and immune modulation [3]. Among them, visfatin, lipocalin-2, adiponectin, and chemerin are particularly important due to their dual roles in metabolic regulation and cancer progression [4–10]. Visfatin is implicated in energy metabolism and inflammation [11, 12], lipocalin-2 regulates iron homeostasis and immune response [13], adiponectin exerts anti-inflammatory and anti-proliferative effects, whereas chemerin has emerged as a regulator of angiogenesis, immune cell recruitment, and tumor aggressiveness [4–10, 13–16].
This study investigates their expression in breast cancer and their associations with clinicopathological features, focusing on lymphovascular invasion (LVI), hormone receptor status, and proliferative activity.
Material and methods
Study population
Patients diagnosed with invasive ductal carcinoma in the period 2015–2018 at the University General Hospital of Patras were retrospectively included. All patients underwent surgical resection without prior neoadjuvant therapy. Clinicopathological data, including ER, PR, HER2/c-ERB2, Ki67, and LVI status, were obtained from pathology reports.
Results
The expression of visfatin, lipocalin-2, adiponectin, and chemerin was analyzed in invasive ductal carcinoma samples. The associations with ER, PR, c-ERB2, Ki67, LVI, and lymph node (LN) metastasis are summarized in the following Table I.
Table I
Correlation between adipokines and estrogen receptor (ER), progesterone receptor (PR), Ki67, and lymphovascular invasion (LVI)
As shown in Table I, visfatin and adiponectin showed associations with proliferative index (Ki67) and LVI, particularly in ER-negative tumors. Lipocalin-2 did not reach statistical significance, although borderline associations with ER and PR were observed. Chemerin expression was compartment-specific: while tumor cell staining did not correlate with classical markers, fibroblast and adipocyte staining was significantly associated with LVI and LN metastasis.
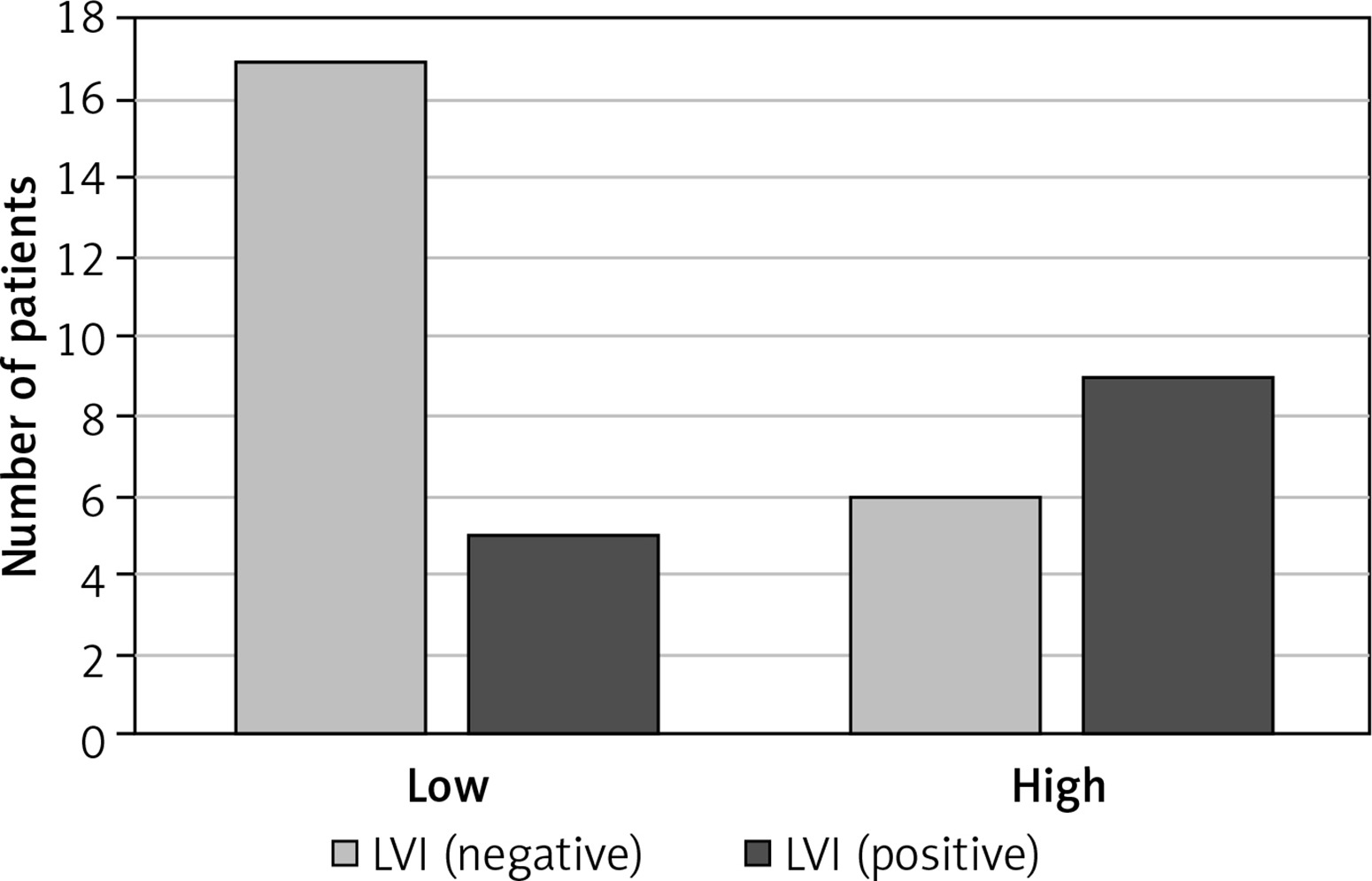
Figure 1 shows that patients with high Ki67 expression more frequently exhibit positive lymphovascular invasion (LVI); on the contrary, patients with low Ki67% are predominantly LVI negative. This finding supports the association between high proliferative activity and more aggressive tumor characteristics.
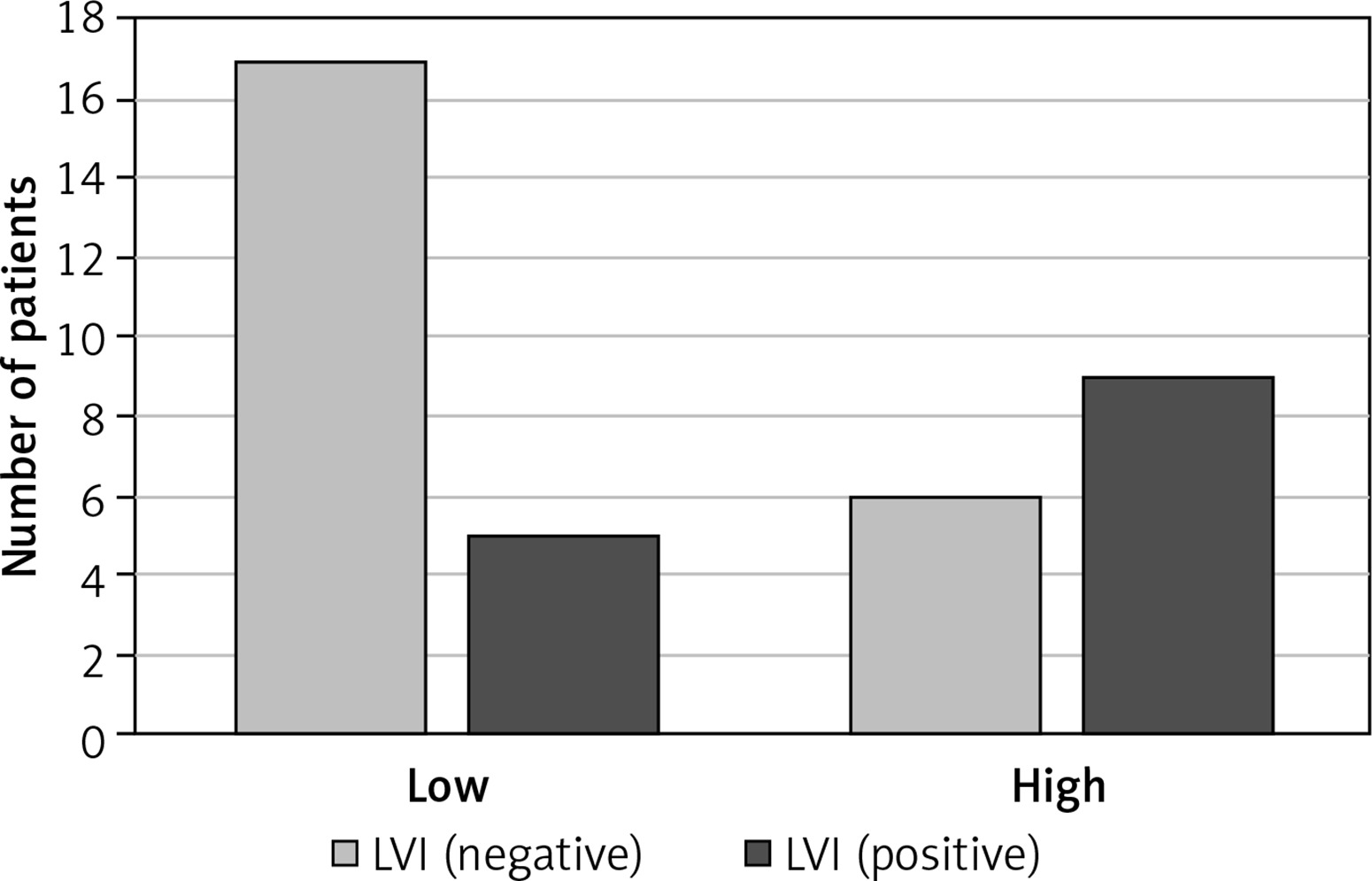
According to Figure 2, patients with low Ki67% show a predominance of LVI-negative cases, whereas in the high Ki67% group, the distribution shifts with more LVI-positive cases compared to negative ones. This may indicate a potential link between high proliferation index (Ki67) and visfatin-related LVI positivity.
As demonstrated in Figure 3, in the LVI-negative group, low Ki67% is markedly more frequent, while in the LVI-positive group, high Ki67% is more common than low. This trend suggests that elevated Ki67% may be associated with LVI positivity when considering lipocalin expression, reflecting an aggressive tumor phenotype.

Discussion
In this study, we observed that visfatin and adiponectin were both linked to higher proliferative activity (Ki67) and the presence of lymphovascular invasion, especially in ER-negative tumors. This pattern aligns with previous reports suggesting that adipokines can influence tumor invasiveness through metabolic and inflammatory pathways. The finding that two distinct adipokines converge on similar associations may indicate a shared impact on the tumor microenvironment, possibly involving pro-angiogenic signaling or immune modulation [12, 17–21].
Numerous preclinical and clinical reports link visfatin overexpression to enhanced proliferation, invasion and worse outcomes in breast cancer, consistent with our observation of associations with proliferative activity and LVI. Mechanistically, NAMPT can drive EGFR/AKT signaling, lipogenesis and migratory phenotypes [17, 20, 21].
Lipocalin-2, in contrast, showed no statistically significant associations in our cohort, although borderline p-values for ER and PR hint that its role might be more subtle or context-dependent. It is conceivable that lipocalin-2 influences tumor biology through mechanisms not directly captured by LVI or proliferative index, such as extracellular matrix remodeling or response to oxidative stress [13, 18]. LCN2/Lipocalin-2 is widely implicated in aggressiveness, including invasion, metastasis and poorer prognosis – especially in HER2-positive and triple-negative contexts. Our borderline trends for ER/PR align with literature suggesting subtype-specific effects and the need for adequately powered cohorts [18].
Chemerin, as was studied in this research and recent studies [5–10, 13–16], exhibits a dual role: acting as a pro-tumorigenic mediator by promoting angiogenesis, but also as a potential immune modulator capable of recruiting NK and T cells into the TME [22]. Prior studies report heterogeneous findings: higher tumor chemerin has been linked to poor prognosis in some series, whereas other work suggests immune-recruiting, anti-tumor roles via ChemR23/CMKLR1 signaling – differences that may reflect stromal vs epithelial localization and serum vs tissue measurements. Our compartment-specific observations are therefore biologically plausible and reinforce the need to analyze chemerin by cellular compartment [13–16, 22].
These results reinforce the concept that metabolic mediators from adipose tissue are not merely passive bystanders in breast cancer progression. Incorporating adipokine profiling into prognostic assessment could one day refine risk stratification, though this will require validation in larger, multi-center studies. Moreover, it is very important to view potential molecular profiling in risk stratification for breast cancer, in light of recent advancements in risk stratification which include complex molecular, genetic and clinical models that assist us in early screening [23, 24]. Finally, the interplay between adipokines and hormone receptor status deserves further investigation, as it may uncover new therapeutic opportunities or predictive biomarkers [12, 16, 22, 25].
This study has several limitations. First, it is a single-center retrospective analysis of a small cohort of patients diagnosed in a single calendar year, which limits external validity and increases the risk of selection bias. The exclusion of patients receiving neoadjuvant therapy may further bias the spectrum of disease biology captured. Second, although immunohistochemistry (IHC) is widely used, pre-analytical variation (fixation time, cold ischemia, antibody lot) and observer variability in semi-quantitative scoring can introduce measurement error; this is particularly relevant for Ki-67, where inter-laboratory reproducibility challenges are well described. Third, our composite IHC score (intensity × proportion) is pragmatic but not standardized across centers, and we did not employ digital image analysis, which might improve precision. Finally, multiple comparisons across several markers and clinicopathological endpoints raise the possibility of type I error; our findings should therefore be viewed as hypothesis-generating pending validation in larger, multi-center cohorts with prespecified adjustment and, ideally, survival endpoints.
In conclusion, visfatin and adiponectin were strongly linked to proliferative activity and lymphovascular invasion, especially in ER-negative tumors, highlighting their potential as biomarkers of aggressiveness. Lipocalin-2 requires further validation in larger cohorts. Chemerin, with its compartment-specific effects, may serve as a prognostic marker for lymph node metastasis and LVI. Future studies integrating multiple adipokines may uncover new avenues for biomarker-driven patient stratification and therapeutic targeting.