Introduction
Chronic venous disease (CVD) constitutes a frequently underdiagnosed pathological condition that progressively diminishes patients’ quality of life and imposes an escalating strain on healthcare resources. The spectrum of CVD encompasses telangiectasias, reticular veins, varicose veins, chronic venous insufficiency (CVI), and chronic venous hypertension, with manifestations including pain, skin discoloration, oedema, and ulceration [1–3]. Primarily afflicting the lower extremity venous system, CVI entails an intricate venous pathology [2, 3]. Given the rising trends in longevity and obesity, the prevalence of CVD assumes heightened significance [4].
The global prevalence of CVI exhibits considerable variability, ranging from less than 1% to 17% in men and less than 1% to 40% in women. This divergence is attributed to disparities in the application of diagnostic criteria, availability of medical resources for diagnosis and treatment, and the distribution of risk factors across diverse global populations [5]. Commonly identified risk factors for CVI include advancing age, familial predisposition to venous disease, smoking, obesity, prolonged periods of standing or sitting, history of venous thrombosis, pregnancy, lower extremity trauma, or surgical interventions [6].
Varicose veins are defined as dilated veins exceeding 3 mm in diameter with characteristic bulging and tortuosity, with higher rates observed in the US and Western Europe [5]. They are classified into primary and secondary categories.
Primary varicose veins stem from a pathology in the superficial venous system, particularly the saphenous veins, characterised by structural damage to bicuspid valves, weakened vessel walls, and elevated luminal pressure. Risk factors for primary varicose veins include family history, aging, obesity, prolonged standing and sitting, hormonal therapy, and pregnancy [1].
On the other hand, secondary varicose veins emerge from insufficient or obstructed deep veins and/or perforator veins, leading to a retrograde flow of pressure into the superficial venous system [1]. This classification underlines the multifactorial aetiology of varicose veins, involving both the superficial and deep venous networks. Understanding these distinctions is crucial for accurate diagnosis, risk stratification, and informed decision-making regarding management strategies.
This study aims to comprehensively investigate the epidemiological landscape of varicose vein disease, examining age group distributions, gender patterns, residence influences, marital status correlations, weight considerations, educational impacts, and various aspects related to varicose veins. By exploring factors such as disease duration, vein location, genetic influences, occupation types, and patient perceptions, the research seeks to contribute valuable insights into the multifaceted nature of varicose veins, laying a foundation for informed interventions, and advancing our understanding of this prevalent vascular condition.
Material and methods
Ethics Board approval was waived for this analysis. This was a single-centre retrospective analysis conducted in Albania from May 2018 to September 2023. Data were collected retrospectively through hospital records. Varicose veins were defined as dilated veins exceeding 3 mm in diameter, diagnosed via ultrasound (U/S). Data collection involved administering a structured questionnaire to study participants, categorically organised into 3 sections. The first section focused on collecting demographic information, the second section involved self-perception of identifying risk factors associated with varicose veins, and the final section included inquiries about history of variceal surgery. This methodology was used to systematically investigate key aspects of varicose vein prevalence, risk perception, and surgical procedures within the patient population studied.
Results
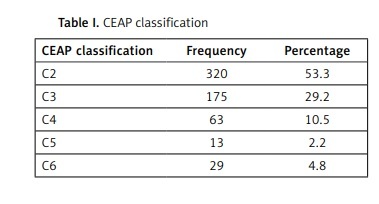
The CEAP classification distribution in our cohort revealed a predominant presence of C2 (varicose veins) in 53.3% of patients, followed by C3 (oedema) at 29.2%, and C4 (changes in skin and subcutaneous tissue secondary to CVD) at 10.5%, whereas C5 (healed venous ulcer) and C6 (Active venous ulcer) were less frequent [8] (Table I). The results showed a varied age distribution among the 600 varicose vein patients. The predominant age group was 41–65 years, constituting 45.5%, highlighting heightened susceptibility in middle-aged individuals (Table II). 67.5% (n = 405) consisted of females, with the remaining 32.5% represented by males. It was observed that 61.8% of the patients resided in urban areas, while 38.2% were from rural areas. The analysis of marital status among the 600 patients revealed that 16.2% were single, 73% were married, 7.2% were divorced, and the remaining 3.7% were widowed. Based on the body mass index (BMI) scale, data from patients indicated that 9.7% fall under the category of underweight, 54.8% had a normal BMI, and 35.5% were categorised as overweight (Table III). Phlebitis was reported by 69.7% of the patients. Only 3% of the patients reported experiencing a haemorrhage attributed to varicose veins. Females reported a higher incidence of haemorrhage from varicose veins, and statistical analysis using χ2 confirmed a significant association between gender and the occurrence of haemorrhage (p < 0.05). Diverse educational levels were reported. Specifically, 24.3% indicated a low educational level, 39.8% expressed a moderate educational level, and the remaining 35.8% affirmed having a higher educational background. Patients were queried about the duration of their diagnosed condition. Results indicated that 14.2% had been diagnosed within the past year, while the substantial majority, encompassing 85.8%, had been diagnosed for more than 1 year. The findings revealed that 86.3% reported the disease localised in the entire leg, 8.0% in the lower part of the leg, and 5.7% in the hip area. The majority (88.0%) of patients acknowledged inheritance as a potential factor for varicose veins, and a significant relationship (p = 0.001) was found between considering inheritance and educational level, with 1.9% of those with a high education level not attributing the condition to inheritance. Tobacco smoking was considered a potential factor for varicose vein disease by 7.8% of patients, while the majority (92.2%) held the opposite belief. Alcohol was perceived as a causative factor for varicose vein disease by 15% of the respondents, contrasting with 85% who responded negatively. Regarding hypertension (HTA), 58.2% of patients responded affirmatively, considering it a factor potentially contributing to varicose vein disease, while 41.8% responded negatively. Among the patients included in the study, 32.5% were identified with diabetes.
Table I
CEAP classification
| CEAP classification | Frequency | Percentage |
|---|---|---|
| C2 | 320 | 53.3 |
| C3 | 175 | 29.2 |
| C4 | 63 | 10.5 |
| C5 | 13 | 2.2 |
| C6 | 29 | 4.8 |
Table II
Age group distribution
Table III
BMI distribution
| BMI [kg/m2] | Frequency | Percentage | Valid percent | Cumulative percent |
|---|---|---|---|---|
| < 18.5 | 58 | 9.7 | 9.7 | 9.7 |
| 18.5–24.9 | 329 | 54.8 | 54.8 | 64.5 |
| 25–29.9 | 213 | 35.5 | 35.5 | 100.0 |
| Total | 600 | 100.0 | 100.0 |
Patients were asked about the risk factors. The findings revealed that 89.5% of respondents attributed varicose veins to pregnancy, while a minority (10.5%) held the opposite view. 57.5% of patients believed that pulmonary diseases contribute to varicose veins, while 42.5% disagreed. 42.2% of the selected patients considered tumour diseases as a contributing factor to varicose veins, while the majority (57.8%) thought otherwise. Pulmonary thromboembolism was not considered to be caused by varicose veins by 84.8% of the patients, while 15.2% believed otherwise. Venous insufficiency was believed to lead to leg oedema, as indicated by 88% of the patients, while 12% expressed disagreement. Varicose veins were believed to cause skin pigmentation, specifically a dark coffee colour, by 86.3% of the patients, with 13.7% expressing a contrary view. Only 5.2% of the patient’s attributed leg ulcers to venous diseases, while the majority (94.8%) disagreed. Out of the surveyed patients, only 30.8% reported undergoing surgical intervention for varicose veins, with the majority (69.2%) not opting for surgery. An additional analysis indicated a statistically significant correlation (p < 0.05) between those who underwent surgery and having been diagnosed with varicose veins for more than 1 year. Patients subjected to surgical intervention for varicose veins predominantly fell within the age bracket of 56–60 years. Furthermore, 43.5% of the respondents perceived surgery as a viable solution to their condition, and among this cohort, a substantial 66.7% had undergone the surgical procedure. Concerning the satisfaction level with the medical staff, the majority (64.4%) expressed varying degrees of contentment, with 18.2% reporting complete satisfaction.
Discussion
The lower extremity’s peripheral venous system plays a pivotal role in blood transportation, regulated by bicuspid valves and muscle contractions. Pathological disruptions, such as venous reflux, lead to venous valve incompetence, dilation, and inflammation, ultimately resulting in CVI. Varicose veins, both primary and secondary, are common manifestations, reflecting superficial and deep venous system pathology [7–10]. CVI progression involves deep venous system incompetence, categorised as primary or secondary, often stemming from thrombotic events. Venous leg ulcers (VLUs), prevalent complications of CVI, present challenges due to their recurrent nature, and prolonged healing times. The fibrin cuff theory, inflammatory trap theory, and dysregulation of proinflammatory cytokines contribute to VLU formation. VLUs, predominantly located on the lower leg, pose a significant burden on patients, with economic implications [11]. Understanding the intricate interplay of venous pathophysiology is crucial for effective management and prevention.
Effectively managing vascular insufficiency necessitates an individualised strategy, acknowledging patient-specific considerations, including mobility limitations and comorbidities like arterial disease and diabetes. The initial approach often involves conservative measures such as compression therapy, with various options available for different severity classes [12–15]. Pneumatic compression devices demonstrate comparability to compression stockings, especially in CVI cases [12, 13, 16]. Long-term compression therapy proves efficacious in CVI, particularly in patients presenting with oedema and venous stasis ulcers [17].
Addressing challenges related to non-adherence rates, pharmacological interventions offer viable alternatives. Micronised purified flavonoid fraction (MPFF), available as Diosmiplex, exhibits benefits in treating VLUs either independently or as an adjunct to compression therapy [18, 19]. Similarly, horse chestnut seed extract (HCSE) has demonstrated positive effects on signs and symptoms of CVI [20, 21]. However, comprehensive, well-reported studies are warranted to establish conclusive evidence, considering limitations such as small sample sizes and unreported adherence in existing research.
In advanced stages of CVI, interventional therapies play a crucial role. Sclerotherapy, while often used for cosmetic purposes, proves valuable in treating CVI, particularly when combined with surgical procedures [22]. Superficial endovenous ablation, employing various methods like thermal, chemical, and mechanical approaches, addresses symptomatic superficial venous disease. Thermal ablation methods, such as radiofrequency ablation (RFA) and endovenous laser ablation (EVLA), are preferred over traditional surgery due to reduced pain and shorter recovery periods [23–26]. Alternative techniques like saphenous vein ligation and cryostripping are explored, with studies demonstrating non-inferiority for cryostripping compared to conventional procedures [27–29]. Furthermore, venoplasty and stenting are recommended for cases of deep vein abnormalities contributing to obstructive disease, particularly in patients with CEAP classes C4–C6. This approach emphasises the importance of tailoring interventions based on the vessel anatomy, source of reflux, and overall severity of symptoms [29].
The findings in this study provide valuable insights into the demographic distribution and multifaceted aspects of varicose vein pathology. The predominant prevalence of C2 (varicose veins) in over half of the 600 patients underlines the clinical relevance of this manifestation. Notably, the concentration of cases in the 41–65-years age group emphasises the heightened susceptibility of middle-aged individuals. Gender-specific considerations reveal a higher incidence of haemorrhage in females, shedding light on potential variations in disease presentation. The association between patient perceptions, educational levels, and beliefs about varicose veins, particularly in relation to inheritance, highlights the need for tailored educational interventions.
Furthermore, the correlation between surgical intervention and prolonged diagnosis duration suggests a nuanced decision-making process among patients. The study’s comprehensive exploration of patient perspectives, risk factors, and treatment choices contributes to a more holistic understanding of varicose vein management. These findings underscore the importance of personalised approaches, considering demographic variations and patient beliefs, in enhancing the overall quality of care for individuals with varicose veins.
Retrospective study design: The retrospective nature of our study poses inherent limitations because it relies on data extracted from hospital records, which may not consistently capture all relevant variables of interest. This retrospective design restricts the availability of comprehensive information on certain factors such as lifestyle habits, genetic predispositions, and detailed clinical histories, which could potentially influence disease severity and progression. Consequently, our ability to conduct advanced statistical analyses, including predictive modelling and assessment of associations between variables, is constrained by the retrospective nature of the data collection process.
Lack of standardised diagnostic criteria: Another notable limitation is the absence of standardised diagnostic criteria for grading venous disease severity. The variability in diagnostic practices across healthcare settings and the absence of universally accepted criteria for staging varicose veins hindered our ability to accurately classify and analyse disease severity in a standardised manner.
Incomplete data collection: Despite efforts to collect comprehensive data from hospital records, the completeness and accuracy of the available information were subject to inherent limitations. Missing or incomplete data entries, variations in documentation practices, and the retrospective nature of data retrieval may have resulted in underreporting or misclassification of certain variables. For instance, detailed information on comorbidities, lifestyle factors, and family history of venous disease may not have been consistently documented, limiting our ability to comprehensively assess their impact on disease severity.
Limited generalisability: As a single-centre study conducted in Albania, the generalisability of our findings to broader populations may be limited. The demographic and clinical characteristics of varicose vein patients in our study setting may not fully represent the diversity observed in other geographic regions or healthcare settings. Variations in healthcare infrastructure, cultural practices, and genetic predispositions across different populations could influence disease presentation and management strategies, thereby restricting the generalisability of our findings beyond the study context.
Absence of prospective follow-up: The retrospective nature of our study precluded the possibility of conducting prospective follow-up assessments to track disease progression and treatment outcomes over time. Longitudinal data collection would have provided valuable insights into the natural history of varicose vein disease, the efficacy of different treatment modalities, and factors influencing disease prognosis. The absence of prospective follow-up limits our ability to draw conclusions regarding the long-term outcomes and trajectory of varicose vein patients in our study cohort.
Limited scope of variables: Lastly, the scope of variables included in our analysis was constrained by the available data and study objectives. While we aimed to comprehensively investigate the demographic and clinical characteristics of varicose vein patients, certain potentially relevant variables, such as socioeconomic status, occupational exposures, and dietary habits, were not systematically collected or analysed. The omission of these variables may limit the depth of our analysis and the comprehensiveness of our findings regarding the determinants of disease severity.
Conclusions: while our study provides valuable insights into the epidemiological landscape of varicose vein disease in Albania, it is important to acknowledge these limitations when interpreting the findings. Future research endeavours should aim to address these limitations through prospective study designs, standardised data collection protocols, and comprehensive assessment of relevant variables to enhance the validity, generalisability, and clinical relevance of findings in the field of venous disease epidemiology.
In conclusion, this study provides a comprehensive examination of varicose vein pathology, offering insights into its prevalence, demographic distribution, and patient perspectives. The predominant occurrence of C2 (varicose veins) highlights its clinical relevance, particularly among middle-aged individuals. Gender-specific variations, such as a higher incidence of haemorrhage in females, add nuance to disease presentation. The correlation between patient perceptions, educational levels, and beliefs about varicose veins underscores the necessity for tailored educational interventions. Additionally, the link between surgical intervention and prolonged diagnosis duration suggests intricate decision-making processes among patients. The study’s thorough exploration of patient perspectives, risk factors, and treatment choices contributes to a holistic understanding of varicose vein management, emphasising the importance of personalised approaches that account for demographic variations and individual beliefs.