Introduction
Aortic stenosis (AS) has been the commonest form of valvulopathy, particularly in developed countries. It generally affects around 2–7% of the elderly population (> 65 years) [1, 2]. Transcatheter aortic valve replacement (TAVR) has been mostly recommended for subjects with severe symptomatic AS who have a considerable surgical risk [3]. Moreover, recent studies have suggested that TAVR might even serve as a more reliable method compared with surgical replacement [4]. It is well known that use of contrast media has been an essential part of TAVR, and enables optimal valve implantation and detection of potential complications during the procedure. However, it might also lead to contrast-induced nephropathy (CIN), which has been a fundamental cause of kidney injury in the hospital setting [5]. Furthermore, CIN evolution following TAVR particularly worsens the prognosis. In this context, several studies have been conducted to identify risk factors for CIN evolution following TAVR [6–8].
The Charlson Comorbidity Index (CCI) has been regarded as a validated tool for the prediction of mortality [9]. The CCI quantifies mortality risk related to a variety of comorbidities such as cerebrovascular disease, pulmonary disease, congestive heart failure, and diabetes, which all can be regarded as factors of poor prognosis in the setting of TAVR. The CCI score has previously been found to have a strong association with disease severity and death in diverse cardiovascular scenarios [10–16]. However, the implications of CCI in CIN prediction have yet to be determined in detail. Therefore, in this study we investigated whether CCI is associated with the development of CIN following TAVR.
Material and methods
Study population
The present study included 118 patients undergoing TAVR in Trakya University Hospital between June 2013 and March 2023. The Society of Thoracic Surgeons (STS) score and the Logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) have been routinely harnessed to evaluate the eligibility for TAVR. Thus, the surgical risks of subjects were assessed using the logistic EuroSCORE together with the STS score. Accordingly, subjects with a EuroSCORE of > 20% or an STS score of >10% were regarded as high-risk subjects [17]. Importantly, subjects receiving dialysis preceding TAVR, those having a creatinine value of > 2.5 mg/dl and those with permanent pacemakers were excluded from the analysis. Presence of severe valvular involvement other than the aortic valve (excluding tricuspid regurgitation), left ventricular ejection fraction value of ≤ 30%, and New York Heart Association (NYHA) functional class IV were also regarded as exclusion criteria. Therefore, 118 subjects were eventually included in the analysis. Subjects were categorized into two groups based on CIN evolution (CIN+ vs. CIN−). CIN was defined as an absolute increment in serum creatinine value of > 0.5 mg/dl or a relative increment of > 25% within 48–72 h following TAVR [18]. The CCI constitutes certain components: history of myocardial infarction, peripheral vascular disease, congestive cardiac failure, pulmonary disease, dementia, peptic ulcer, connective tissue disease, renal disease, hemiplegia, diabetes, lymphoma, solid tumour, leukaemia and liver disease. The study protocol was endorsed by the Local Ethical Committee of the Trakya University Hospital. Written informed consent was acquired from all participants.
TAVR procedure
In all subjects, clopidogrel 75 mg, aspirin 100 mg, and intravenous antibiotherapy were initiated before the procedure. Iohexol (Omnipaque; GE Healthcare), a non-ionic, low-osmolar, and monomeric contrast medium, was preferred as the contrast medium. The amount of contrast agent used was also recorded during TAVR. Diagnostic modalities including computed tomography and coronary angiography that necessitate the administration of contrast agent were planned at least 72 h earlier. The procedures were performed under general anaesthesia or deep sedation using the CoreValve (Medtronic, Minneapolis, Minnesota, United States) or ACURATE neo aortic valve (Boston Scientific, Marlborough, MA, USA) via the transfemoral route in all subjects. Initially, a temporary pacemaker was placed for rapid pacing and also as a backup strategy against a possible iatrogenic complete atrioventricular block. Thereafter, two Proglides were placed preceding the insertion of the vascular sheath. Following the deployment of the device, contrast agent was injected to evaluate the presence as well as the degree of paravalvular leak. Repeat angiography of the access vessel was also performed to evaluate the patency of the vessel and potential complications including bleeding. Following the procedure, echocardiographic examination was also performed to evaluate the bioprosthesis function and potential mechanical complications.
Statistical analysis
Statistical analyses were performed using the IBM SPSS Statistics software, version 21. A value of p < 0.05 was regarded as statistically significant. Continuous variables approximating the normal distribution were recorded as mean ± standard deviation (SD), whereas variables characterized by a skewed distribution were recorded as median (interquartile range: 25–75). Frequencies and percentages were used in the setting of categorical variables. Comparisons of baseline features between the groups were made using the independent t-test in the setting of normally distributed variables and the Mann-Whitney U test in the setting of non-normally distributed variables along with Fisher’s exact or chi square (χ2) test in the context of categorical variables. Univariate and multivariate logistic regression analyses were conducted to analyse the hypotheses. The CCI in isolation and all potential variables were used for the prediction of CIN. Lastly, receiver-operating characteristic (ROC) curve analysis using logistic regression was performed along with calculation of the area under the curve (AUC), as well as sensitivity and specificity values, to evaluate the performance of CCI in the prediction of CIN evolution.
Results
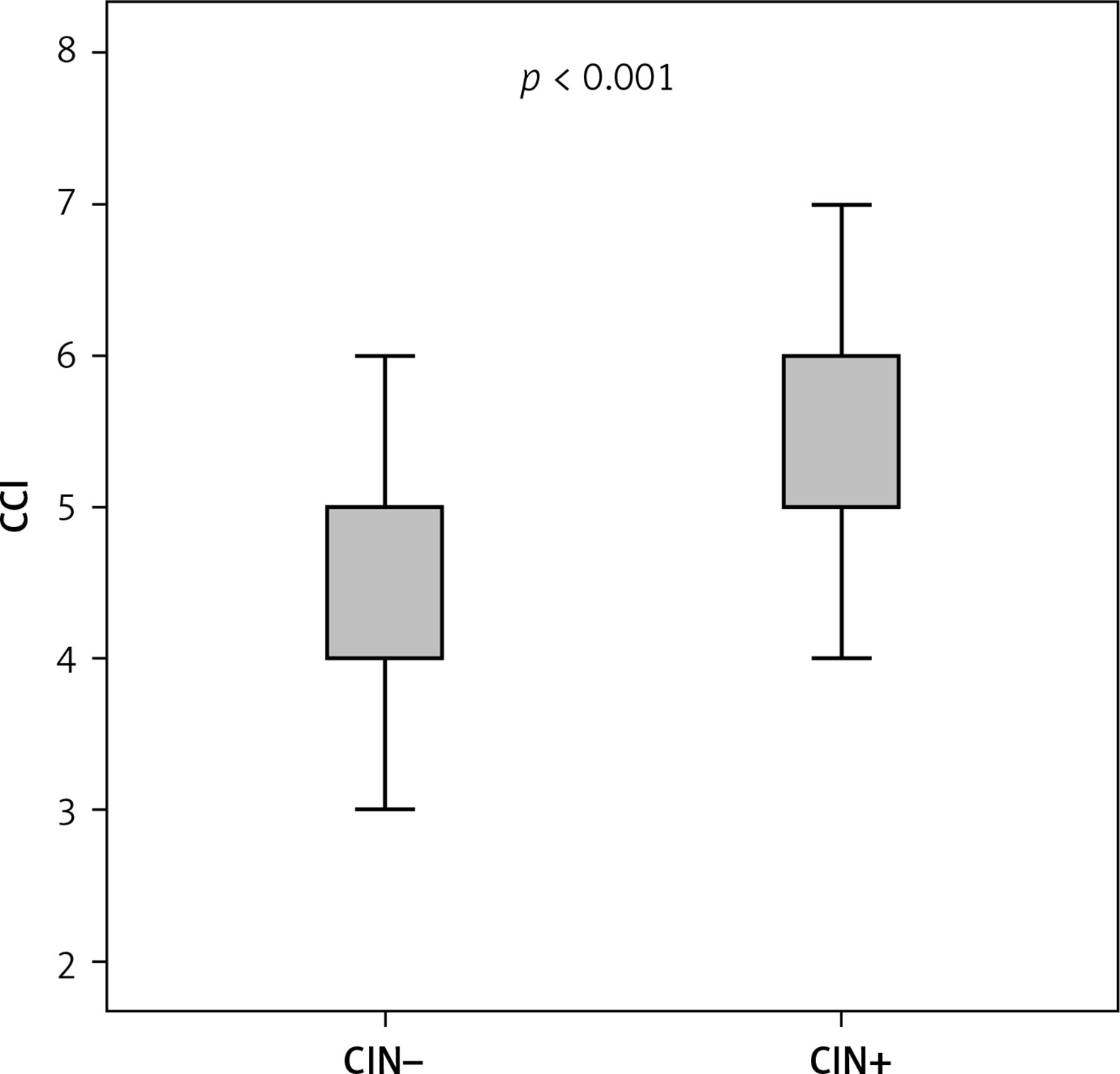
The analysis included a total of 118 patients undergoing TAVR. The percentage of CIN within 72 h was found to be 21.2% (n = 25). The percentage of female subjects was 62.7% (n = 74). The comparison of groups (CIN− and CIN+) in terms of demographics and baseline features is presented in Table I. There were no significant differences between the groups as regards to risk factors including diabetes, hypertension, chronic obstructive pulmonary disease, and cerebrovascular disease. However, the incidence of co-existing coronary artery disease was found to be higher in the CIN+ group (p = 0.034). The CCI value was higher in the CIN+ group (5.80 ±1.15 vs. 4.56 ±1.25, p < 0.001) (Figure 1). No significant differences emerged between the groups as regards age, gender, left ventricular ejection fraction, amount of contrast media used, moderate-severe aortic regurgitation, and atrial fibrillation. However, the logistic EuroSCORE, baseline creatinine and WBC levels appeared to be significantly higher in the CIN+ group. The percentage of all-cause mortality during the hospitalization was found to be 16.1% (n = 19). The mortality rates were significantly higher in those with CIN (60%, n = 15 vs. 4.3%, n = 4; p < 0.001).
Table I
Demographics and baseline clinical characteristics between CIN− and CIN+ groups
In univariate analysis, diabetes mellitus, concomitant coronary artery disease, CCI, white blood cells, logistic EuroSCORE, and baseline creatinine were found to be associated with CIN evolution following TAVR (p < 0.1). In multivariate logistic regression analysis, CCI was independently and positively associated with CIN evolution (odds ratio [OR] = 1.845, 95% CI: 1.053–3.233, p = 0.032) together with logistic EuroSCORE (OR = 1.152, 95% CI: 1.063–1.248, p = 0.001). Univariate and multivariate analyses are presented in Table II.
Table II
Multivariate logistic regression analysis of potential predictors of contrast-induced nephropathy
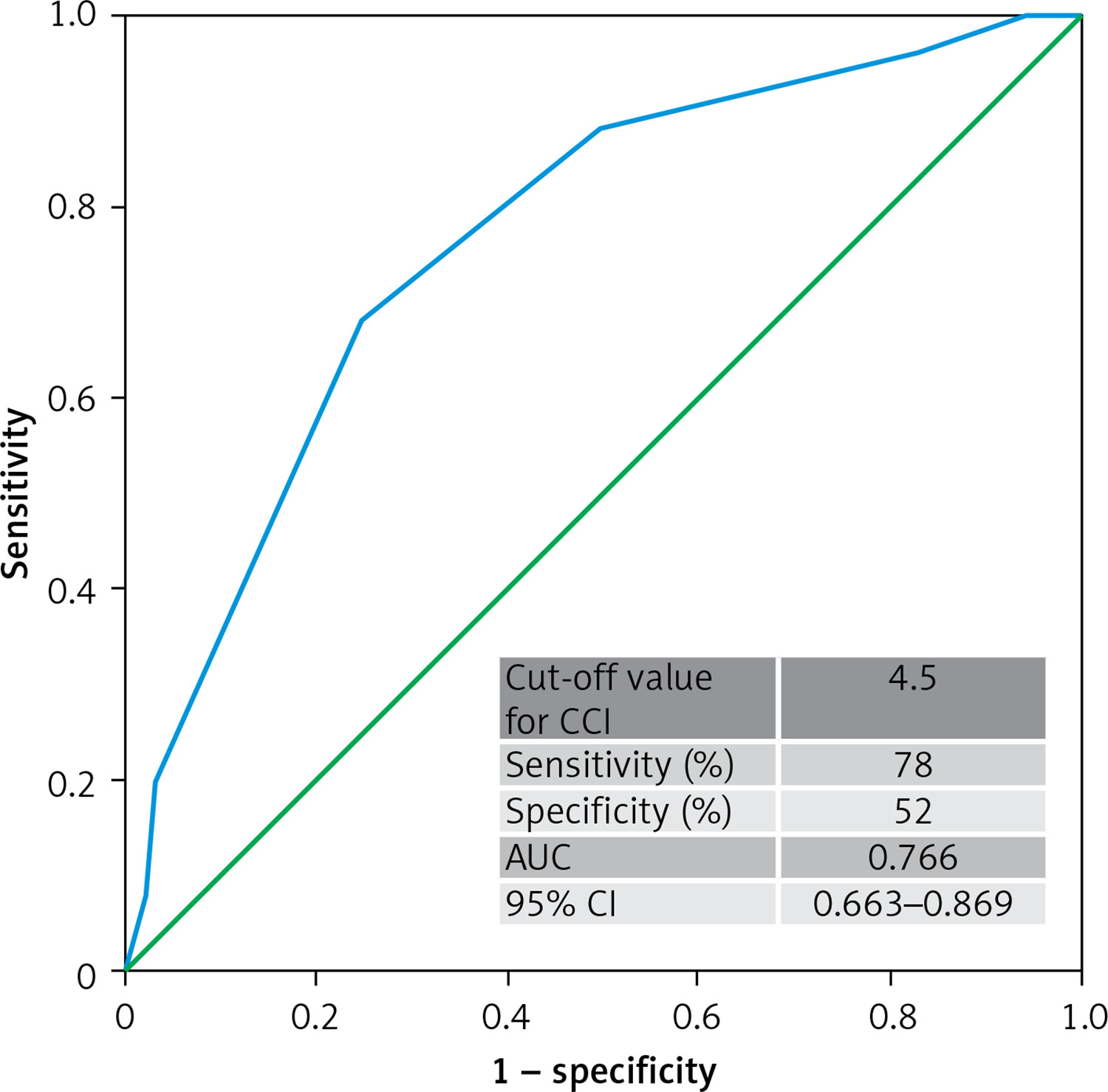
The area under the ROC curve for CCI in the prediction of CIN was 0.766 (95% CI: 0.663–0.869; p < 0.001), and the sensitivity and specificity were found to be 78.0% and 52.0%, respectively, in the setting of an optimum cut-off value of 4.5. The results of ROC analysis are displayed in Figure 2. When subjects were stratified into two groups based on a cut-off value of CCI (> 4.5 or ≤ 4.5), those with higher CCI values were found to have a greater likelihood of CIN evolution in comparison to those with a lower CCI on multivariate logistic regression analysis. (adjusted Model II: OR = 7.493, 95% CI: 2.098–26.759, p = 0.011, p for trend = 0.002).
Discussion
Significant comorbidities have been quite common in patients with symptomatic AS and have been associated with complications in the setting of interventional procedures. The CCI has been the widely recognized score of comorbidity. Accordingly, the current study evaluated the link between CCI and CIN evolution following TAVR. Importantly, patients with a higher CCI score exhibited a significant increase in CIN evolution following the procedure.
The mechanisms of renal damage following cardiovascular interventions still need to be illuminated. Certain factors, such as diabetes, age, amount of contrast medium, haemodynamic disturbances, and renal dysfunction at baseline may significantly facilitate CIN evolution [8]. Notably, CIN has been the fundamental cause of hospital-acquired renal dysfunction, with a ratio of 10–30% following TAVR [7, 19]. In the present analysis, the percentage of patients with CIN was found to be 21.2%, a value in accordance with the previous literature.
On the other hand, CCI reflects the comorbidity burden, and hence quantifies the prognostic impact of various conditions potentially rendering this index as a strong prognosticator indicator in patients with diverse clinical conditions [20]. Moreover, it is a simple and easily applicable index, and may be easily acquired from electronic medical records [21]. More importantly, CCI is a robustly validated index of outcome, particularly in the context of cardiovascular interventions such as percutaneous coronary intervention, coronary bypass grafting as well as in cardiovascular conditions such as heart failure, aortic stenosis and acute coronary syndromes [10–16]. Using the CCI might also gain significant popularity in the prediction of TAVR outcomes. It was previously reported that high CCI values may be associated with increased mortality at 1 month following TAVR [22]. Similarly, higher CCI was also reported to be associated with late mortality after TAVI as well [23]. Conversely, another study demonstrated that CCI score and mortality were not independently associated in patients undergoing TAVI [24]. However, only a few studies have employed the CCI to evaluate the risk of CIN evolution in these patients. Therefore, we devised the present study to further analyse the predictive power of the CCI for CIN evolution in the setting of TAVR. These findings suggest that CCI > 4.5 is strongly associated with CIN evolution following TAVR. Mechanistically, a multifaceted impact of existing co-morbidities on CIN evolution is quite likely in patients undergoing TAVI. Besides the potential association of co-morbidities with reduced renal reserve, it can also be speculated that co-morbidities may also necessitate complex management strategies that might potentially facilitate CIN evolution in this group of patients. Finally, in line with previous reports [25, 26], a higher logistic EuroSCORE, another major score for the evaluation of co-morbidities, was also found to have an association with CIN evolution in the present study.
First, this study was retrospective, with potential biases related to the study design. Second, survival analysis was not possible due to the absence of follow-up data for the overwhelming majority of subjects. Third, residual confounding factors including medications as well as other obscure confounders could not be avoided owing to the retrospective as well as observational features of the analysis.
In conclusion, the burden of comorbid conditions appears to be significant in patients undergoing TAVR. On the other hand, CIN has been associated with unfavourable prognosis in the setting of cardiovascular interventions. The present study demonstrated the independent association of baseline CCI with postprocedural CIN in patients undergoing TAVR. Our findings suggest that CCI may help identify patients who are at higher risk for CIN in the setting of TAVR.