Introduction
Cardiac involvement in systemic sclerosis (SSc), also known as scleroderma, can be either primary or secondary. Primary involvement stems directly from the disease’s vascular pathology, while secondary involvement is due to complications such as pulmonary arterial hypertension (PAH) or interstitial lung disease. In the early phase of SSc, vascular injury leads to capillary loss and abnormal vascular remodeling, despite elevated levels of vascular endothelial growth factor (VEGF) [1]. This paradoxical impairment of angiogenesis is due to endothelial dysfunction, reduced number and function of endothelial progenitor cells (EPCs), and increased levels of anti-angiogenic isoforms such as VEGF165b [2]. The resulting tissue hypoxia plays a key role in triggering and sustaining fibrotic processes. As SSc progresses, the inflammatory phase gives way to fibrosis, characterized by vascular remodeling with intimal thickening and adventitial fibrosis, leading to vessel narrowing and obliteration [3]. Despite ongoing hypoxia, angiogenesis remains insufficient, and anti-angiogenic factors are upregulated, perpetuating vascular damage and fibrosis.
SSc can lead to various heart conditions, including myocardial fibrosis, pericardial effusion, arrhythmias, conduction system defects, and valvular impairments such as mitral regurgitation, aortic regurgitation, and aortic stenosis.
Additionally, SSc may cause myocarditis, diastolic dysfunction, myocardial ischemia, and myocardial hypertrophy. Some medications used in SSc treatment, such as cyclophosphamide, can also induce cardiac toxicity. Managing heart disease in individuals with SSc requires a collaborative approach between cardiologists and rheumatologists who are familiar with the complexities of the disease. The prevalence of primary cardiac involvement in SSc is challenging to determine due to the wide range of cardiac symptoms, the occurrence of subclinical phases, the variety of diagnostic methods used, and the heterogeneity of patient populations. When cardiac involvement becomes clinically apparent, it is considered a significant prognostic factor. The disease’s pathophysiology involves immune dysregulation, vasculopathy, and fibrosis, contributing to various cardiac manifestations [2].
Imaging techniques such as computed tomography (CT), magnetic resonance imaging (MRI), and echocardiography have shown that SSc progresses from reversible vasospastic abnormalities to structural changes in arterioles and coronary vessels, leading to ischemia, fibrosis, and, ultimately, impaired systolic and diastolic function [1]. While premature atherosclerosis is known to contribute to cardiovascular issues in diseases such as systemic lupus erythematosus and rheumatoid arthritis, its role in SSc remains unclear, though endothelial dysfunction, vasculopathy, and systemic inflammation, combined with traditional cardiovascular risk factors, are hypothesized to contribute [3]. This review aims to offer an in-depth examination of the pathophysiology, classification, and diagnostic guidelines – particularly imaging techniques – along with the latest management approaches for both primary and secondary cardiac complications associated with SSc. Understanding these cardiovascular issues is vital because they significantly impact patient outcomes, contributing to morbidity and mortality in SSc. Given the complexity and severity of these complications, it is crucial for clinicians to grasp the full scope of potential comorbidities and work in close coordination with cardiologists. Such collaboration ensures more accurate diagnoses, timely interventions, and optimized treatment plans, ultimately improving the quality of care and long-term prognosis for affected patients.
Prevalence and prognosis
Cardiac involvement in SSc occurs early in the disease, with a prevalence of 15–35%, and cardiovascular complications account for about 27.2% of reported deaths. Major risk factors include male gender, advanced age, African American ethnicity, diffuse cutaneous SSc, tendon friction rubs, abnormal nail-fold capillaroscopy, and poor quality of life scores. While primary cardiac involvement can occur in both limited and diffuse forms, it is typically more severe in diffuse SSc [4]. Rapidly progressing skin disease, positive anti-U3-RNP antibodies, and skeletal myopathies indicate a high risk of cardiac damage. Subclinical cardiac impairment is estimated to exceed 70%, depending on the screening and diagnostic tools used [5].
Valvular heart disease SSc remains underexplored. Most available data stem from autopsy studies that reveal endocarditis-like changes in the mitral, tricuspid, or aortic valves. Observations include aortic regurgitation and mitral valve prolapse due to nodular thickening, but no comprehensive population-based studies have been conducted. Tricuspid regurgitation is the most frequently noted valvular issue, often linked to pulmonary hypertension. Although valvular vegetations are generally rare in SSc, a study of 28 autopsied SSc cases identified such lesions in 5 instances, affecting the mitral and tricuspid valves, the chordae tendineae [6], or the aortic valve [7]. Additionally, nodular thickening of the mitral and aortic valves, along with regurgitation and mitral valve prolapse, has also been reported.
Increased cardiovascular and macrovascular disease prevalence in SSc is linked to a worse prognosis, with heart failure being a significant prognostic factor [3]. In a cohort of 953 patients with diffuse cutaneous SSc, cardiac involvement was observed in 15% through clinical presentation and various diagnostic tools [6]. Valvular vegetations are rare, but nodular thickening can lead to regurgitant and prolapsed valves. Additionally, the development of PAH is considered a poor prognostic sign and is associated with a higher mortality rate in SSc patients compared to idiopathic PAH (IPAH), as shown in the Johns Hopkins Cohort from 2001 to 2005 [8]. High-risk findings include clinical heart failure, decreased right ventricular (RV) function, PAH, low cardiac index, high mean right atrial pressure, and ventricular arrhythmia [9]. Pericardial involvement, while common at autopsy (33–72%), is clinically symptomatic in only 5–16% of cases [10].
Pathophysiology
In SSc, initial microvascular injury – resulting from endothelial cell damage, loss of capillaries, and defective angiogenesis – leads to diminished blood flow in affected organs such as the heart and lungs [1]. Prolonged oxygen deprivation leads to endothelial cell dysfunction and a reduction in the density of myocardial capillaries, a process known as capillary rarefaction [3]. This impaired microvascular network decreases myocardial perfusion, which in turn promotes myocardial stiffness and diastolic dysfunction – a common cardiac manifestation in SSc [4]. Additionally, chronic hypoxia triggers maladaptive remodeling of the pulmonary vasculature, increasing pulmonary vascular resistance and contributing to the development of PAH. PAH is a serious and often fatal complication in SSc patients, associated with high morbidity and mortality rates. Therefore vascular damage in SSc, characterized by endothelial dysfunction, inflammation, and oxidative stress, impairs vascular tone and leads to tissue ischemia. This hypoxia also increases VEGF production, resulting in dysfunctional angiogenesis and fibrosis during both inflammatory and non-inflammatory stages. Consequently, vasculopathy, immune dysregulation, and fibrosis contribute to large vessel disease and cardiac dysfunction [2]. The pathophysiology of cardiac involvement in SSc is complex and not fully understood, but endothelial dysfunction is a key factor, leading to vasospasm, microvascular damage, and ischemia [11]. This tissue injury triggers an inflammatory response, activating fibroblasts and increasing extracellular matrix proteins such as collagen, which drives fibrosis. Autoantibodies against angiotensin II type I receptor (AT1R) and endothelin-1 type A receptor (ETAR) also play a crucial role by affecting collagen production and angiogenesis [12]. Recent studies highlight interleukin-1 as a significant player in inflammation, which will be discussed further in this article [13].
Primary cardiac involvement in SSc
Cardiac involvement in SSc was initially observed in 1926 by Heine, who discovered abnormalities involving the coronary arteries, pericardium, and myocardium during an autopsy of a patient with SSc [14]. It is reported in about 20% to 35% of patients, varying with the diagnostic methods employed [15]. Using advanced imaging modalities such as echocardiography and cardiac MRI, studies have detected subclinical myocardial abnormalities in up to 30–40% of patients, emphasizing the frequent presence of cardiac complications even in those without symptoms [16]. Myocardial involvement, typically manifesting as fibrosis and microvascular ischemia, is the most common cardiac complication in SSc and is closely linked to higher morbidity and mortality, primarily due to heart failure and arrhythmias. Pericardial disease, which includes conditions such as pericarditis and pericardial effusion, is less common but can still lead to significant clinical issues [17]. Arrhythmogenic complications, involving conduction abnormalities and various arrhythmias, also play a critical role in patient prognosis and are a leading cause of sudden cardiac death in SSc.
In fact, SSc-related cardiac involvement is a major cause of death in these patients, accounting for up to 25% of deaths [1]. Early detection and timely management of cardiac involvement are vital to improve patient outcomes.
Biomarkers
Several biomarkers have been investigated to detect cardiac involvement in SSc [15], including:
Elevated levels of cardiac troponin (cTn) in blood have been correlated with an increased risk of cardiovascular complications in SSc patients.
Elevated levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) is found in both myocarditis and heart failure caused by scleroderma.
Elevated levels of endothelin-1 (ET-1) have been associated with PAH and cardiac involvement.
Elevated levels of serum matrix metalloproteinases (MMPs) have also been associated with cardiac involvement and fibrosis in SSc.
Interleukin (IL)-6 is a proinflammatory cytokine produced by various cells, including endothelial cells, dendritic cells, macrophages, and lymphocytes, in response to tissue injury or infection. In the heart, IL-6 promotes leukocyte recruitment, proliferation, and collagen production, leading to cardiac remodeling. Elevated serum IL-6 levels in SSc patients, compared to healthy controls, correlate with high-resolution computed tomography (HRCT) scores and peak pulmonary artery pressures [16].
IL-17, elevated in serum and skin of SSc patients, promotes collagen production and fibrosis [17]. High IL-17 levels are associated with reduced left ventricle ejection fraction (LVEF), increased right ventricular pressures, and more severe interstitial lung disease and skin symptoms [18].
In SSc, elevated serum levels of angiotensin II type 1 receptor (anti-AT1R) and anti-endothelin type A receptor (anti-ETAR) autoantibodies have been associated with an increased risk of lung fibrosis, PAH, and higher mortality, as documented in previous studies. These autoantibodies promote fibrosis by inducing the expression of transforming growth factor-β (TGF-β) in human microvascular endothelial cells (HMEC-1). Furthermore, the roles of the angiotensin and endothelin systems in SSc pathogenesis are well recognized. SSc patients show raised serum levels of angiotensin II (Ang II) and ET-1, with elevated ET-1 detected in fibrotic lung tissue, highlighting the importance of these pathways in disease progression [18]. Anti- AT1R and anti-ETAR autoantibodies have also gained attention as valuable biomarkers, as their presence correlates with disease severity and complications such as PAH and lung fibrosis. Detecting these autoantibodies in patients’ sera can facilitate early identification of those at higher risk for vascular and fibrotic complications, allowing for timely diagnosis and closer clinical monitoring. Additionally, monitoring their levels may provide important information on disease activity and therapeutic response, underscoring their potential role in personalized management of SSc [15].
Given the central roles of the renin-angiotensin-aldosterone system (RAAS) and the ET system in cardiovascular disease, it is expected that autoantibodies against the AT1R-AAs and ETAR-AAs contribute to cardiovascular pathologies [18]. Their vasoconstrictive and proinflammatory actions may be key drivers in various cardiac conditions where inflammation and vascular constriction are critical factors, including pulmonary arterial hypertension, atrial fibrillation, heart failure with preserved ejection fraction, and coronary microvascular dysfunction. Nonetheless, the available data remain limited, highlighting the need for further research to better understand their precise role in cardiovascular disease.
It is important to note that while these biomarkers may be useful in detecting cardiac involvement in SSc, they are not specific to SSc and can also be raised in other cardiac and non-cardiac disorders. Therefore, they should be interpreted in conjunction with the patient’s clinical presentation and other diagnostic tests.
In the following section, we discuss different ways SSc can affect the heart.
Myocardial involvement and arrhythmias
The myocardium is frequently affected in SSs, with both the left and right ventricles being involved. Autopsy findings in SSc patients have revealed focal pathological changes in myocardial tissue, including contraction band necrosis and fibrosis. Segmental fibrosis, resulting from ongoing ischemia and/or immuno-inflammatory damage, is a hallmark of myocardial involvement [14]. Myocardial fibrosis not only contributes to ischemic damage but also leads to conduction defects. Myocarditis, often regulated by interleukin-1, is associated with acute and severe cardiac manifestations [19].
Conduction abnormalities and arrhythmias arise from myocardial or conduction system fibrosis. Myocardial fibrosis leads to atrial and ventricular ectopias and tachyarrhythmias, such as atrial flutter, atrial fibrillation, supraventricular tachycardia, and ventricular tachycardia, while bradyarrhythmias, including atrioventricular blocks, are due to conduction system fibrosis [15]. Supraventricular arrhythmias are more common in SSc patients, with about two-thirds experiencing these compared to a lower prevalence of ventricular tachyarrhythmias [20]. Right bundle branch block is linked to a more than five-fold increase in mortality risk [21]. In a study by Follansbee et al., among 50 SSc patients, common electrocardiogram abnormalities included left anterior fascicular block (16%) and first-degree atrioventricular heart block (8%) [22]. The Scleroderma Arrhythmia Clinical Utility Study (SAnCtUS) assessed 150 consecutive scleroderma patients using Holter monitoring and cardiac magnetic resonance imaging (CMR) to identify predictors of arrhythmias. The study developed the SAnCtUS score, which found that patients with the highest scores were 3.86 times more likely to experience sustained ventricular tachycardia or sudden cardiac death within 1 year compared to those with lower scores, regardless of ejection fraction or initial Holter findings [23].
Left ventricular (LV) involvement
Left ventricular dysfunction in SSc primarily causes diastolic dysfunction but can also result in systolic dysfunction and restrictive cardiomyopathy. Diastolic dysfunction is more frequently associated with an increased risk of death than LV systolic dysfunction [24]. In cases of cardiac involvement related to scleroderma, no correlation has been found between the fibrotic areas and pathological changes in a single coronary artery. Additionally, hemosiderin deposits in the myocardium, commonly seen in atherosclerosis, are not present in the myocardial pathology associated with SSc, emphasizing that atherosclerosis is not the primary mechanism dictating myocardial involvement [1] (Table I [25]).
Table I
Features of myocardial involvement in systemic sclerosis distinct from coronary atherosclerotic disease [25]
Guidelines recommend that asymptomatic patients with SSc undergo a yearly echocardiogram using a standardized Scleroderma Doppler Echocardiogram Protocol. Patients with SSc and LV involvement exhibit higher LV filling pressures (larger E/e ratios) and longer isovolumetric relaxation periods. This is linked to the duration of the disease in months, as well as the mean duration of Raynaud’s phenomenon, suggesting a temporal relationship in SSc-related fibrosis [26].
Conventional echocardiographic techniques are ineffective at detecting early LV systolic failure [27]. A study by Allanore et al. demonstrated that innovative echocardiographic speckle-tracking strain analysis can successfully identify mild myocardial dysfunction. Decreased global longitudinal strain (GLS), a measure of LV systolic dysfunction, has been associated with reduced functional capacity and the development of arrhythmias [28].
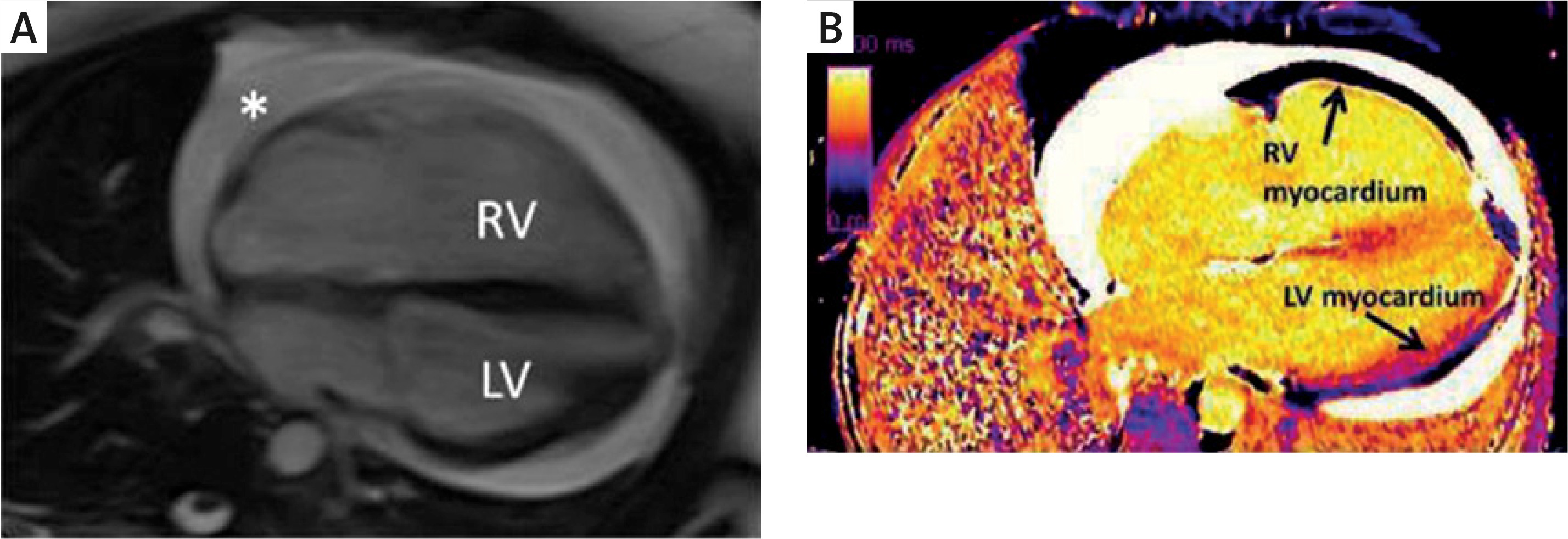
CMR imaging can identify diffuse fibrosis (Figure 1), even in patients with normal echocardiograms and without any evidence of late gadolinium enhancement. The study by Tzelepis et al. found that mesocardial late gadolinium enhancement (LGE) in a linear pattern located in the basal and mid cavity segments of the LV was associated with a prolonged duration of Raynaud’s phenomenon and abnormal Holter monitor results, indicating an association between fibrosis and arrhythmias [29]. Cardiac MRI with LGE identifies myocardial fibrosis by highlighting areas where gadolinium contrast accumulates in damaged or scarred heart tissue. This technique provides a visual representation of structural damage and remodeling within the myocardium. Meanwhile, serum biomarkers such as NT-proBNP and cardiac troponins are released into the bloodstream in response to cardiac stress and injury [30]. Elevated NT-proBNP levels typically reflect increased cardiac wall stress or strain, often caused by fibrosis and impaired diastolic function, whereas troponins indicate ongoing myocardial cell damage [29]. Research has demonstrated a correlation between the extent of fibrosis detected by LGE and higher concentrations of these biomarkers, implying that patients with greater myocardial fibrosis also show more pronounced biochemical signs of cardiac injury and dysfunction. This interplay highlights the value of combining imaging and biomarker assessment for a more precise evaluation of cardiac involvement in SSc. Stress CMR may exhibit greater sensitivity than rest CMR in detecting subclinical disease, justifying the hypothesis that hypoperfusion in SSc may be attributable to microvascular disease rather than epicardial coronary artery disease [15].
Figure 1
Diffuse interstitial fibrosis of the right ventricle using cardiovascular magnetic resonance imaging. A – Four-chamber cine showing enlarged right ventricle and circumferential pericardial effusion (*). B – Increased T1 time (diffuse fibrosis) in right ventricular myocardium compared to left ventricular myocardium RV – right ventricle, LV – left ventricle.
The use of vasodilators, such as calcium channel blockers (e.g. nicardipine), and ACE inhibitors, has been shown to improve myocardial perfusion and limit the progression of complications in scleroderma-related heart involvement [28]. In nearly all cases of myocarditis causing LV dysfunction, the administration of immunosuppressants, such as corticosteroids, cyclophosphamide, and azathioprine, has resulted in significant clinical improvement, normalization of cardiac enzymes, and improvement in MRI findings [29].
Pericardial involvement
Pericardial involvement is a common occurrence in scleroderma patients, affecting 15–19% of patients [31]. It can range from pericardial inflammation, fibrinous pericarditis, pericardial effusion, and pericardial adhesions, to rarely constrictive pericarditis or tamponade. It is more prevalent in patients with the limited cutaneous subtype (30%) compared to 16% in those with diffuse skin involvement [32]. Scleroderma pericardial effusion is characterized by non-inflammatory pericardial fluid without the presence of autoantibodies, immunological complexes, or complement depletion. The limited efficacy of corticosteroid treatment supports this idea [33]. Small pericardial effusions do not carry significant prognostic implications, but large symptomatic pericardial effusions are associated with unfavorable outcomes [34].
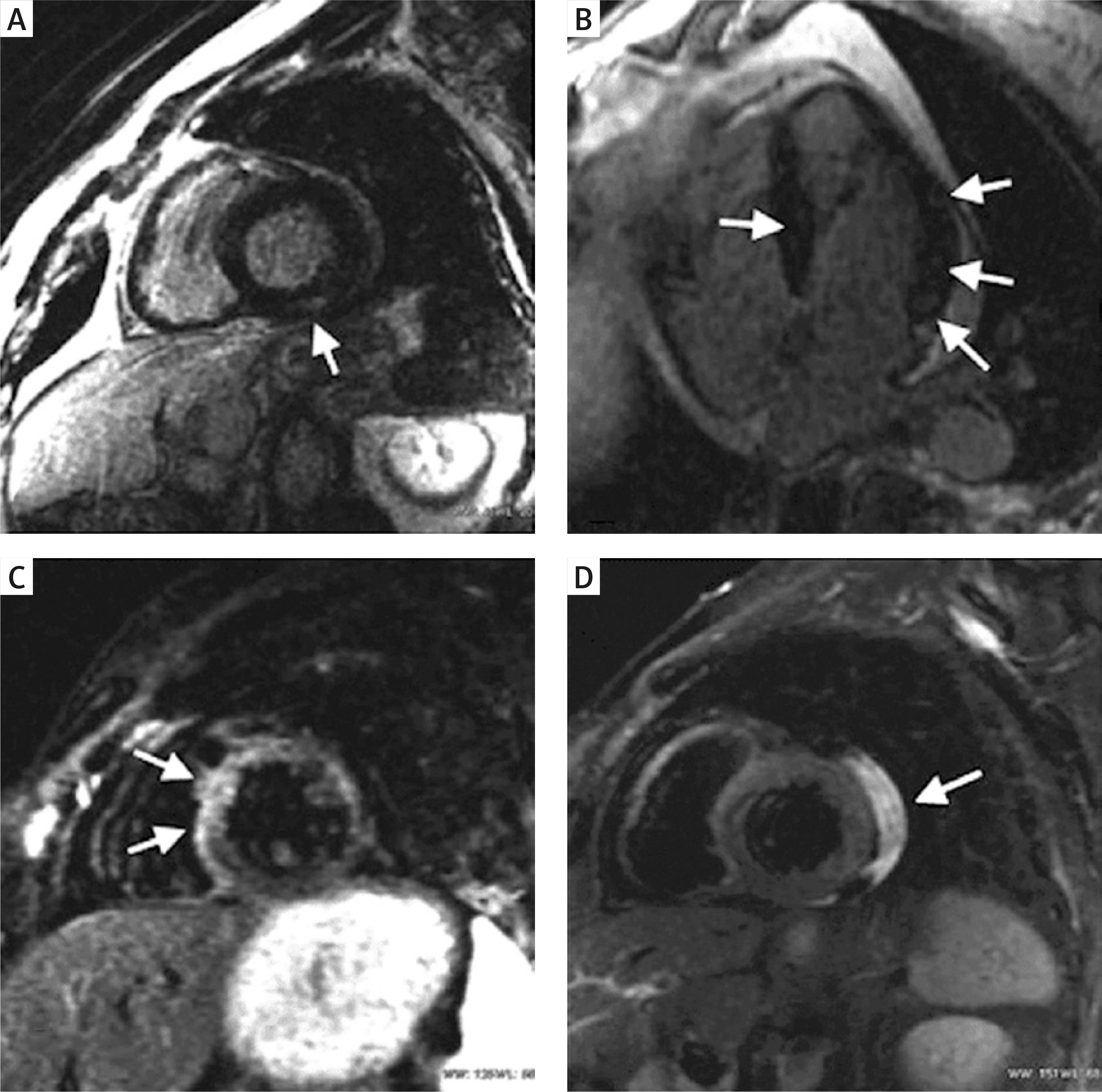
In assessing pericardial disease, a multimodality imaging approach is crucial. While two-dimensional echocardiography (2DE) can identify the existence of effusion or tamponade (evidenced by diastolic collapse of right-sided chambers, noticeable alterations in blood flow across the mitral and tricuspid valves during respiration, and unusual ventricular septal motion during inspiration), three-dimensional echocardiography (3DE) proves valuable in outlining the degree of pericardial thickening and precisely determining the dimensions, positioning, and extent of stranding within the pericardial effusion. CMR imaging should be considered when there is strong suspicion of pericarditis, especially when initial tests such as echocardiography and electrocardiography (ECG) yield negative results or when symptoms persist or recur over an extended period. CMR can identify pericardial thickening, edema, and inflammation, and it can also aid in steroid therapy for recurrent pericarditis (Figure 2). Constrictive pericarditis can be diagnosed using CMR imaging, with respiratory flow variation across the mitral valve and increased relative septal excursion being reliable indicators of constriction. Myocardial fibrosis identified by cardiac MRI, especially using LGE and T1 mapping techniques, has been linked to a higher risk of arrhythmias and sudden cardiac death in SSc patients [35]. These imaging methods offer a non-invasive approach to detect fibrotic tissue, which can act as a substrate for potentially life-threatening ventricular arrhythmias, highlighting their important prognostic role in this patient group.
Figure 2
Cardiac magnetic resonance findings in patients with SSc. A – Evidence of subepicardial delayed enhancement. B – Patchy intramural septal and lateral delayed enhancement. C – Diffuse hyperintensity due to edema in anterior septum and anterolateral segment. D – Pericardial effusion
Treatment typically involves the use of nonsteroidal anti-inflammatory drugs. A trial of corticosteroids can be considered in cases of recurrent pericarditis and can be life-saving when underlying myocarditis is present [36]. Pericardiocentesis is only indicated if there is evidence of tamponade physiology or hemodynamic instability [13].
Table II provides an overview of the effectiveness of each imaging modality, along with their advantages and limitations, for the most common cardiac complications of SSc [37].
Table II
Summary of each imaging modality for the most common cardiac complications seen in systemic sclerosis
[i] SSc – systemic sclerosis, echo – echocardiography, CT – computed tomography, cMR – cardiovascular magnetic resonance, ECG – electrocardiography, RHC – right heart catheterization, RV – right ventricle, TV – tricuspid valve, E/A – peak velocity in early diastole (E wave) to peak velocity flow in late diastole (atrial contraction – A wave), TAPSE – tricuspid annular plane systolic excursion, FAC – fractional area change, EF – ejection fraction, 3DE – three-dimensional echocardiography, RVSP – right ventricular systolic pressure, LV – left ventricle, ECV – extracellular volume, RVH – right ventricular hypertrophy, PAH – pulmonary arterial hypertension, PASP – pulmonary artery systolic pressure, PA – pulmonary artery, WHO – World Health Organization, MV – mitral valve, LVEF – left ventricular ejection fraction, LGE – late gadolinium enhancement, LVH – left ventricular hypertrophy, PVH – pulmonary venous hypertension, PVC – premature ventricular contractions, ILD – interstitial lung disease, CTEPH – chronic thromboembolic pulmonary hypertension, PH – pulmonary hypertension, STE – speckle-tracking echocardiography.
Therefore, it is advisable for all SSc patients to undergo a screening ECG to identify conduction abnormalities, signs of hypertrophy, and chamber enlargement. In cases where an abnormal ECG or symptoms such as palpitations, dizziness, presyncope, or syncope are present, consideration of Holter monitoring and the placement of an implantable loop recorder is warranted. The use of exercise treadmill electrocardiogram may aid in detecting arrhythmias that manifest during physical activity.
Prevention/management of primary SSc cardiac complications
SSc affects multiple organ systems, requiring a multidisciplinary team for optimal care. Effective management involves early diagnosis, ongoing monitoring, and targeting organ-specific issues. Although there is no cure, treatment focuses on alleviating symptoms and preventing further damage. Due to its rarity and diverse symptoms, a thorough pretreatment evaluation is essential to assess organ involvement and risk. Treatment should address active issues, ideally with therapies that impact multiple systems or overlapping conditions.
Biomarkers play a pivotal role in the assessment and prognostic evaluation of cardiac involvement in SSc, offering critical insights into underlying disease mechanisms, progression, and clinical outcomes. Established cardiac biomarkers such as NT-proBNP and high-sensitivity troponins are particularly effective in identifying subclinical myocardial dysfunction and in predicting future cardiovascular complications [33]. In addition, novel biomarkers including galectin-3 and growth differentiation factor-15 (GDF-15) have emerged as potential indicators of myocardial fibrosis and inflammatory activity, although their clinical applicability requires further investigation. Integrating these biomarkers into standard clinical practice holds promise for enhancing early diagnosis, informing therapeutic strategies, and refining risk stratification in patients with SSc-related cardiac involvement [34].
Continuous rhythm monitoring using 24–48-hour Holter electrocardiography or implantable loop recorders plays an important role in the early detection of subclinical arrhythmias in SSc. These rhythm disturbances including ventricular ectopy, conduction abnormalities, and atrial arrhythmias are frequently asymptomatic but carry significant prognostic implications, including an increased risk of sudden cardiac death [36]. Identifying such abnormalities before clinical symptoms arise enables earlier intervention and may enhance both risk stratification and overall management of cardiac involvement in this patient population.
Treatment options for SSc include cyclophosphamide (CYC), mycophenolate mofetil (MMF), methotrexate (MTX), azathioprine (AZA), and hydroxychloroquine (HCQ), though large trials are lacking. Corticosteroids are typically avoided due to the risk of inducing scleroderma renal crisis, especially with high doses or prolonged use.
Emerging evidence suggests that IL-1 plays a central role in the inflammatory cascade associated with myocarditis, including in the context of SSc. IL-1-mediated myocardial inflammation contributes to cardiomyocyte injury, fibrosis, and adverse remodeling, all of which are hallmarks of cardiac involvement in this disease. Targeted inhibition of IL-1 signaling, particularly through the use of IL-1 receptor antagonists such as anakinra, offers a promising therapeutic avenue. Anakinra has demonstrated efficacy in other forms of inflammatory myocarditis and heart failure with inflammatory components, supporting its potential utility in SSc-related myocarditis [38]. Although clinical data specific to SSc remain limited, preliminary case reports and small studies suggest favorable outcomes with IL-1 blockade. Given the potentially severe consequences of unchecked myocardial inflammation, consideration of IL-1-targeted therapies, even in an investigational or adjunctive context, may be warranted in selected patients, particularly those with biomarker or imaging evidence of active myocardial inflammation [37].
Management of cutaneous lesions
The modified Rodnan skin score (mRSS) is used to assess cutaneous sclerosis in both clinical and research settings. Most trials focus on early diffuse cutaneous systemic sclerosis (dcSSc), where immunomodulatory treatments may reduce disease severity. Randomized controlled trials have shown that CYC [28], MMF [38], and hematopoietic stem cell transplantation (HSCT) [39] improve cutaneous sclerosis, with MMF preferred as a first-line therapy due to its better safety profile. HSCT is reserved for severe, treatment-resistant cases and can lead to significant improvement despite its high risks.
Management of interstitial lung disease
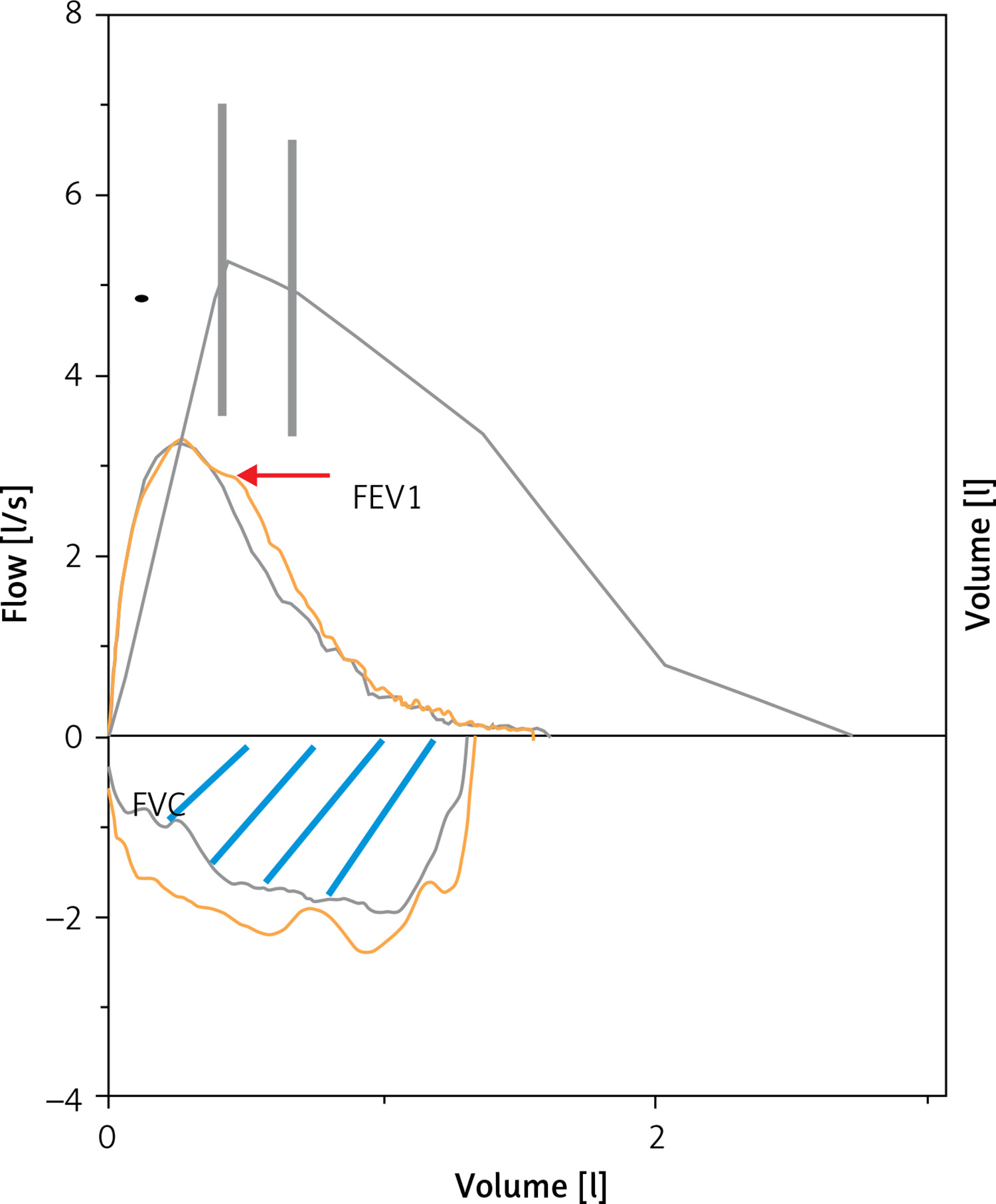
In trials for SSc-related interstitial lung disease (SSc-ILD), forced vital capacity (FVC) is often used as a key outcome measure since reduced FVC is linked to higher morbidity and mortality (Figure 3).
Figure 3
Flow-volume curve showing a decrease in FVC (blue lines showing the area under the curve) by 59% and FEV1 (red arrow) by 53%
Two pivotal studies, SLS-I [40] and SLS-II [39], demonstrated that CYC and MMF are effective disease-modifying treatments for SSc patients with active ILD. In SLS-I, CYC treatment showed significant improvements in FVC%-predicted, total lung capacity (TLC)%-predicted, and radiographic fibrosis compared to placebo after 12 months [39]. In SLS-II, both MMF (over 24 months) and CYC (over 12 months) resulted in notable improvements in FVC%-predicted over a 24-month period. Additionally, MMF and CYC treatment were associated with better outcomes in radiographic fibrosis and reduced self-reported dyspnea.
Raynaud phenomenon
Treatment aims to prevent digital ischemia and ulcers. Conservative measures include keeping extremities warm, avoiding smoking and stress, and discontinuing sympathomimetic medications. β-blockers should be avoided if they exacerbate symptoms. First-line vasodilators are dihydropyridine calcium channel blockers such as nifedipine and amlodipine. Additional options include pentoxifylline, nitroglycerin, sildenafil, and, for severe cases, iloprost and bosentan. A small randomized crossover study with primary and secondary Raynaud’s phenomenon (RP) patients compared fluoxetine 20 mg to nifedipine 40 mg daily. Fluoxetine showed no effect on blood pressure but a statistically significant decrease in the RP attack severity and frequency from onset to end of trial [41]. Another meta-analysis of seven placebo-controlled trials evaluated the use of topical nitrates for RP, combining various outcome measures into a single treatment effect size scale. Subgroup analysis for secondary RP demonstrated a statistically significant benefit in favor of topical nitrates [42].
Cardiac involvement
Arrhythmias are generally managed with antiarrhythmic drugs and, occasionally, pacemakers. There is no current evidence that immunosuppressive or vasodilator therapies are effective for cardiac issues associated with scleroderma. Treatment for SSc should be individualized due to potential multi-organ involvement and concomitant medications. Some drugs may cause conduction abnormalities or arrhythmias. High-dose intravenous corticosteroids can lead to tachyarrhythmias, while methotrexate (MTX) may rarely cause right bundle branch block or ventricular arrhythmias. Hydroxychloroquine (HCQ) is safer than chloroquine regarding cardiac conduction issues. Epidemiological studies have linked domperidone to serious ventricular arrhythmias and sudden cardiac death. Implantable cardioverter defibrillators (ICDs), which monitor heart rhythm and deliver pacing stimuli or shocks, have been effective in preventing malignant ventricular arrhythmias in selected patients. Although no specific guidelines exist for SSc, ICDs should be considered for high-risk patients – both for secondary prevention and primary prevention in those with left ventricular ejection fraction < 30% (or < 35% if ischemic) and symptomatic ventricular tachyarrhythmia. ICD implantation is recommended only for patients without advanced non-cardiac organ failure. In a study of 10 SSc patients with cardiac involvement, mainly diastolic dysfunction, ICDs detected and treated ventricular tachycardia in 3 patients over 36 months.
Scleroderma renal crisis
ACE inhibitors are the only proven treatment for scleroderma renal crisis and should be administered at the earliest signs, using the maximum tolerated dose. Captopril is preferred due to its flexible dosing. The use of ACE inhibitors in this condition has reduced the 1-year mortality rate from 85% to 24%. Scleroderma renal crisis requires hospitalization and prompt ACE inhibitor therapy, starting with short-acting agents such as captopril to lower systolic BP by ~20 mm Hg in 24 h and reach 120/70 mm Hg within 72 h. Once stable, switch to a long-acting ACEI. If BP remains uncontrolled, add a dihydropyridine calcium channel blocker. Avoid diuretics unless needed for volume management to prevent RAAS activation. Angiotensin receptor blockers and renin inhibitors lack supporting evidence. While initial renal function may worsen, continued use of ACE inhibitors can lead to significant improvement over time. Prophylactic use is not advised, as it does not prevent the crisis and may increase morbidity and mortality.
Secondary cardiac complications
Coronary artery disease and atherosclerosis
Atherosclerosis is a key driver of cardiovascular disease and the leading cause of global mortality. While microvascular disease in SSc is well documented, the presence of macrovascular disease and atherosclerosis in SSc remains debated [9]. In SSc, calcification, vasculopathy, and endothelial damage are prominent features that can contribute to an elevated risk of atherosclerosis and cardiovascular disease [2].
In the early stages of SSc, endothelial cell (EC) damage and apoptosis can trigger perivascular inflammation, oxidative stress, and tissue hypoxia. Many clinical symptoms of SSc, including Raynaud’s phenomenon, hand edema, digital ulcers, pulmonary hypertension, erectile dysfunction, scleroderma renal crisis, and cardiac damage, are primarily linked to endothelial cell dysfunction. Endothelial activation is driven by cell adhesion molecules such as E-selectin, vascular cell adhesion molecule 1 (VCAM-1), and intercellular adhesion molecule 1 (ICAM-1) [3]. Elevated expression of these molecules on the endothelium can result in their release into the bloodstream. Additionally, increased levels of circulating soluble adhesion molecules are associated with peripheral microvascular abnormalities in SSc and the progression from neovascularization to fibrotic plaques in atherosclerosis within the general population [11].
Both subtypes of SSc impact the cardiovascular system. Disease duration and renal damage in SSc are independent risk factors for coronary heart disease. While microvascular functional and structural changes are characteristic of SSc-associated vasculopathy, macrovascular atherosclerotic disease significantly worsens prognosis and contributes to mortality in 20–40% of SSc cases [15]. Thickening of the intima-media complex in the common carotid artery is observed in 64–65% of SSc patients [43]. In addition to frequent atherosclerotic lesions in coronary arteries, SSc patients may experience coronary spasms (Raynaud’s cardiac syndrome), particularly those with coronary thrombosis. The microvascular lesions in SSc, including endothelial damage and smooth muscle cell migration into vessel intima, bear similarities to the atherosclerotic process. Endothelial dysfunction is a key factor in both SSc and atherosclerosis. A recent prospective study by Cassius et al. found that 76% of SSc patients had hemodynamic abnormalities, and 28% had increased vascular stiffness in the lower limb arteries [44]. Accelerated atherosclerosis in SSc is thought to result from various factors, including viral infections, immune system activation, anti-endothelial antibodies, and ischemia-reperfusion injury. Elevated levels of markers linked to atherosclerosis – such as C-reactive protein, homocysteine, von Willebrand factor, and vascular adhesion molecules – have been observed in individuals with SSc. Lipid levels in these patients have been reported as either increased or normal.
Pulmonary arterial hypertension
Recent updates to the definition of PAH now include patients with a mean pulmonary artery pressure > 20 mm Hg, as measured by right heart catheterization, and a pulmonary vascular resistance > 2.0 Wood units. These changes aim to improve early detection and diagnosis, which is crucial as delayed diagnosis is linked to higher morbidity and reduced lifespan [44]. Hereditary forms, including familial and simplex PAH, are typically diagnosed around age 34.9 ±14.9 years [45]. Connective tissue diseases, such as systemic lupus erythematosus, mixed connective tissue disease, and SSc, are common causes of PAH [46]. In SSc, PAH affects > 10% of patients, with prevalence rising to > 26% depending on the diagnostic methods [47]. PAH in SSc can stem from arterial fibrosis or arterial lumen narrowing (Figure 4).
Figure 4
Cellular mechanisms of SSc-PAH. A – Cross-section of pulmonary artery from a control. B, C – Pulmonary artery cross section showing early and advanced PAH with medial hypertrophy and adventitial thickening
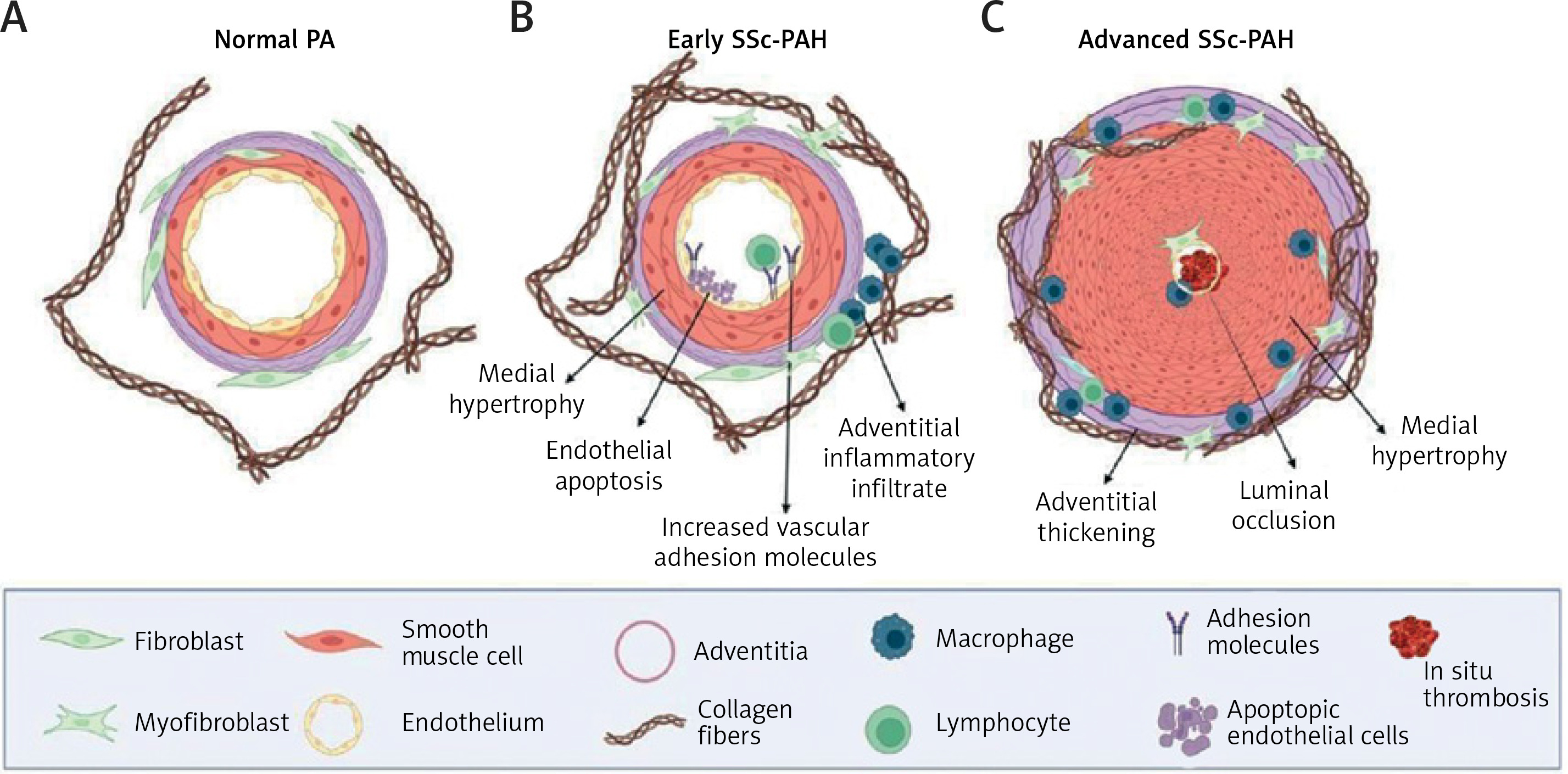
In pulmonary fibrosis, PAH generally progresses moderately due to increased pulmonary vascular resistance. However, in SSc with limited fibrosis, PAH is severe due to vessel narrowing from media hypertrophy, intimal hyperplasia, inflammation, and thrombosis [48]. Symptoms, notably dyspnea, typically worsen over 6–12 months, with an average survival of 2 years; fibrosis-related PAH progresses more slowly, over 2–10 years [6].
PAH is a major determinant of morbidity and mortality in SSc. Screening for PAH is essential for early diagnosis and treatment, which improves survival [49]. Echocardiography should be conducted if PAH is suspected, although tricuspid regurgitation may be absent in 15–20% of patients [6]. Carbon monoxide diffusing capacity (DLCO) is a crucial screening marker for vascular disease. Further imaging, such as CT and MRI, can assess right ventricular function [50]. Right heart catheterization (RHC) is the gold standard for diagnosing PAH, measuring pulmonary wedge pressure to rule out other causes [6].
Management of pulmonary hypertension
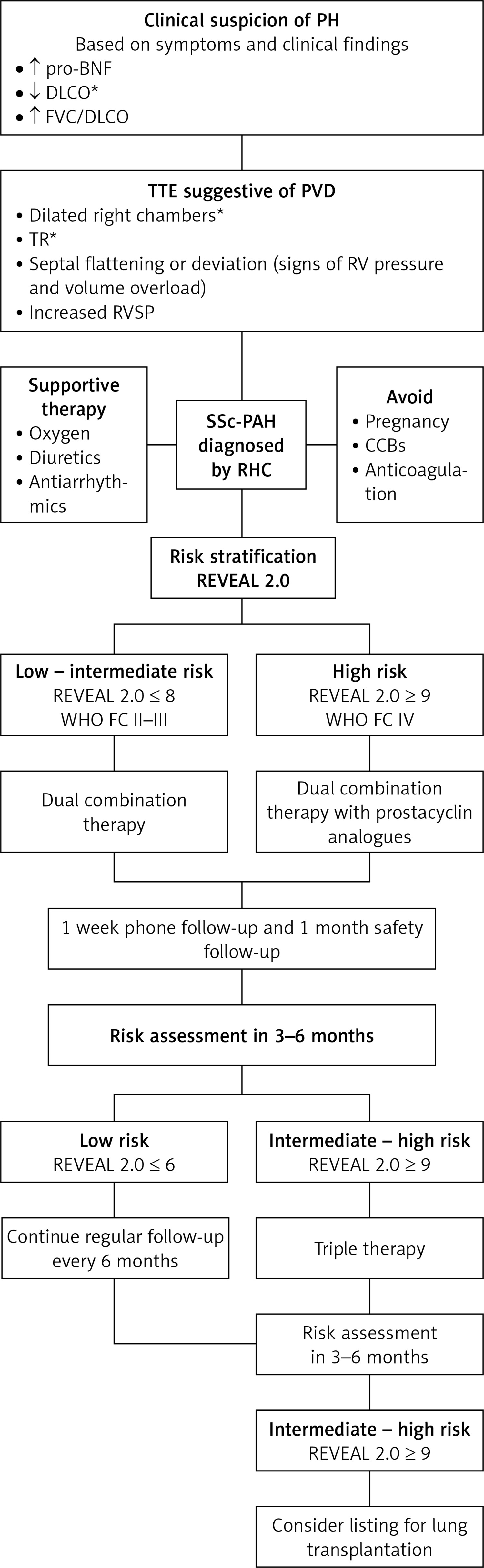
Management of PAH involves a multidisciplinary approach and response to vasoreactivity testing [51]. Treatments include calcium channel blockers (CCBs), phosphodiesterase 5 inhibitors, endothelin receptor antagonists, and prostacyclin pathway modifiers [6, 44]. The treatment algorithm for SSc-PAH used in the Johns Hopkins pulmonary hypertension program helps guide the management [52] (Figure 5).
Figure 5
Treatment algorithm for SSc-PAH used in the Johns Hopkins pulmonary hypertension program
PH – pulmonary hypertension, proBNP – pro–brain natriuretic peptide, DLCO – diffusing capacity of the lung for carbon monoxide, FVC – forced vital capacity, TTE – transthoracic echocardiography, PVD – pulmonary vascular disease, TR – tricuspid regurgitation, RV – right ventricular function, RVSP – right ventricular systolic pressure, SSc-PAH – systemic sclerosis-associated pulmonary arterial hypertension; CCBs – calcium channel blockers.
PAH can impact every aspect of daily life, making lifestyle changes crucial for managing symptoms and improving prognosis. To manage PAH effectively, it is important for patients to quit smoking and avoid exposure to secondhand smoke. Additionally, they should avoid hot tubs, saunas, and high-altitude areas to minimize strain on the lungs and heart.
Maintaining a healthy diet by limiting saturated fats, trans fats, cholesterol, and salt is also vital. For those with PAH, pregnancy carries significant risks and should be discussed with healthcare providers before planning. For patients with pulmonary hypertension (PH) secondary to heart failure with preserved ejection fraction who remain symptomatic despite strict salt and fluid restrictions, diuretics, mineralocorticoid receptor antagonists, and sodium-glucose transport protein-2 inhibitors are advised [53].
Vasoreactivity testing during right heart catheterization (RHC) uses inhaled nitric oxide, intravenous adenosine, or epoprostenol. A positive response is defined as a drop of more than 10 mm Hg in mean pulmonary arterial pressure (mPAP) to below 40 mm Hg with increased or unchanged cardiac output [6, 11, 54].
Calcium channel blockers
CCBs were among the first vasodilators for PAH and are effective primarily in “responders” who show a significant immediate hemodynamic response. They benefit fewer than 10% of PAH patients, with long-term efficacy in less than 5%, and are less effective in non-idiopathic PAH. For patients with a positive vasoreactivity test, CCBs should be initiated at the maximum tolerated dose and adjusted gradually, with regular monitoring via echocardiography and right heart catheterization every 3–6 months. CCBs should not be used in “non-responders” due to potential adverse effects. Those who do not benefit from CCBs should be treated with newer “advanced PAH therapies” [6, 52].
Endothelin receptor antagonists
Pulmonary vasoconstriction and proliferation are initiated by the binding of endothelin-1 to endothelin receptors A and B on smooth muscle cells. Selective or non-selective blocking of A and/or B receptors has shown comparable efficacy. Ambrisentan, macitentan, and bosentan are some of the widely used endothelin receptor antagonists and have been shown to enhance exercise capacity and reduce the worsening of PAH. In the BREATHE-1 trial, bosentan helped prevent the worsening of walking distance in the 6-minute walk test, with a notable effect in patients with IPAH (a 46-meter improvement in IPAH vs. 3 meters in SSc-PAH).
Nevertheless, different adverse effects have also been identified, such as peripheral edema with ambrisentan and an increase in liver function tests seen with bosentan and macitentan [44, 55, 56].
Phosphodiesterase 5 inhibitors and adenylate cyclase inhibitors
Smooth muscle relaxation in the pulmonary vasculature is mediated by nitric oxide, which activates guanylate cyclase to increase cyclic guanosine monophosphate (cGMP) production [51, 57].
Current therapies target adenylate cyclase and phosphodiesterase type 5 (PDE-5). PDE-5 inhibitors, such as tadalafil and sildenafil, prevent the degradation of cGMP, enhancing smooth muscle relaxation and vasodilation [48, 58]. These medications significantly improve exercise capacity, hemodynamics, and symptoms, whether used alone or as adjunctive therapy [1].
Riociguat, a cGMP stimulator that works with or without nitric oxide, offers similar benefits and side effects as PDE-5 inhibitors [50, 59]. The concomitant use of PDE-5 inhibitors and riociguat is contraindicated due to an increased risk of adverse effects, including headache, hypotension, dizziness, vomiting, and even death, as demonstrated in the PATENT Plus trial.
Prostacyclin analogs and prostacyclin receptor antagonists
The prostacyclin pathway is often not regulated in patients with PAH. Its role is to induce vasodilation, prevent platelet aggregation, and inhibit proliferation. Some of the most widely used medications in this category include epoprostenol, iloprost, treprostinil, beraprost, and selexipag [6, 55]. Epoprostenol is administered intravenously because of its short half-life. Treprostinil can be given intravenously, subcutaneously, orally, or via inhalation. In the US, iloprost is only available for inhalation, although an intravenous formulation is offered in Europe.
Initiating inhaled prostacyclin therapy is a reasonable option for patients with ILD and PAH, especially when pulmonary vascular resistance (PVR) exceeds 4.0 Wood units. This recommendation is supported by a randomized clinical trial that demonstrated an average improvement of 33 m in the 6-minute walk test compared to placebo. The most common side effects of these medications include hypotension, flushing, headache, and diarrhea [1, 6]. Prostaglandins are frequently used to treat ischemic digital ulcers in patients with SSc.
Oral soluble guanylate cyclase (sGC) stimulators (e.g., riociguat)
Despite treatment advances and improved survival rates, patients with pulmonary hypertension often continue to face significant limitations in exercise and functional capacity, severely affecting their quality of life. The nitric oxide (NO)- sGC-cyclic guanosine 3′,5′-monophosphate (cGMP) pathway is crucial for cardiovascular health, particularly in regulating vasodilation and pulmonary vascular tone. Riociguat, an oral sGC stimulator, enhances this pathway through two mechanisms: it directly stimulates sGC independently of NO and also increases sGC sensitivity to the body’s own NO [44].
Winrevair (sotatercept)
Winrevair is an activin signaling inhibitor that modulates vascular proliferation by targeting activin A and TGF-β superfamily ligands. It offers a novel treatment for adults with Group 1 PAH. In the PULSAR trial, 24 weeks of sotatercept significantly reduced pulmonary vascular resistance, improved exercise capacity, and lowered NT-proBNP levels compared to placebo [60].
Future prospects
Several medications are being investigated for the treatment of SSc-related PAH. One of these is ifetroban, a thromboxane A2/prostaglandin H2 receptor antagonist, which works by reducing blood vessel constriction, promoting vasodilation, and ultimately lowering PAH [61].
Another potential treatment is rituximab, a monoclonal antibody targeting CD20, a protein present on B-cell surfaces. Rituximab is believed to slow lung fibrosis progression by decreasing antibodies against platelet-derived growth factor. Currently, rituximab is undergoing a Phase 2 clinical trial for this purpose in SSc-PAH patients, although preliminary results have not shown significant improvement in the 6-minute walk distance [62].
Bardoxolone methyl is also being studied for PAH, including in connective tissue disease-related PAH. This drug works by activating nuclear factor erythroid 2-related factor 2 (Nrf2) and inhibiting nuclear factor-kB (NF-kB), and is thought to target multiple cell types involved in SSc-PAH, including smooth muscle cells, endothelial cells, and macrophages [63].
History and clinical presentation
The clinical presentation at the beginning can be non-specific, characterized by dyspnea on exertion, fatigue, weakness, malaise, and lightheadedness. A thorough history taking and physical examination, along with a high degree of suspicion, are usually the first steps leading to a diagnosis. Most of these symptoms may also be related to any underlying connective tissue disorder (CTD), lack of exercise, or deconditioning. Dyspnea with exertion, paroxysms of nocturnal dyspnea, and/or orthopnea are among the most common complaints in patients with signs of pulmonary congestion and elevated left-sided heart pressures, as seen in left heart failure. If chronic, these symptoms may also be accompanied by ascites and pedal edema. On the other hand, individuals with pulmonary hypertension and subsequent right heart failure typically experience gradually worsening symptoms, including shortness of breath, ascites, pedal edema, and/or congestive hepatomegaly. In cases of right heart failure without left heart involvement, patients usually do not report orthopnea or paroxysms of nocturnal dyspnea. In severe cases of pulmonary hypertension, syncope and sudden cardiac death can occur, often attributed to arrhythmias or acute right ventricular failure.
During a physical examination, it is possible to appreciate an accentuated pulmonic component of the second heart sound, coupled with the presence of a tricuspid regurgitation murmur. Moreover, in cases of advanced disease, signs and symptoms related to right heart failure may become noticeable.
Imaging, such as chest X-ray, can be remarkable for pulmonary artery enlargement and pulmonary vascular congestion on the periphery. On an electrocardiogram, characteristics of right atrial enlargement can be identified, such as P waves with an amplitude > 2.5 mm on the inferior leads (II, III, and AVF) and/or > 1.5 mm on V1 and V2.
Additional signs and symptoms of cardiac involvement in SSc can resemble those of myocardial ischemia, such as dyspnea and chest pain. In SSc, chest pain may exhibit atypical characteristics, but it is crucial to consistently consider the possibility of coronary artery disease in this group of patients. Individuals with arrhythmias may encounter palpitations, which can arise from either bradycardia or tachycardia or simply a perceived pounding of the heartbeat in the presence of sinus rhythm, a common occurrence. The presence of cardiac involvement generally portends poorly for the patient [64]. Systolic dysfunction is often clinically occult, but overt congestive heart failure can occur in advanced disease.
Among four studies that used radionuclide ventriculography to assess left ventricular ejection fraction (LVEF), only nine out of 85 (11%) patients had an abnormal LVEF under resting conditions [65]. As expected, there is a significant difference in symptoms and hemodynamics during exertion. In one study, 46% of patients showed a reduced LVEF during exercise, whereas only 15% of this group exhibited reduced function at rest [66]. Sometimes, pericardial effusion may present as the initial manifestation of pulmonary hypertension in individuals with scleroderma [46].
Diagnostic and treatment modalities
Cardiac involvement can often remain clinically silent, especially in the early stages of SSc [67]. Various diagnostic modalities are available for assessing the diverse cardiac manifestations of SSc, including laboratory markers and imaging techniques. To evaluate macrovascular damage, methods such as pulse wave velocity (PWV), ankle-brachial pressure index (ABPI), pulse wave analysis (PWA), and Doppler ultrasound are used [3]. For sensitive detection of microvascular damage, procedures such as coronary angiography, pharmacologic stress testing, radionuclide myocardial perfusion imaging, PET scans, and thallium-201 SPECT are employed [6].
Patients with pericardial involvement and heart failure primarily undergo electrocardiograms and echocardiography for evaluation. Echocardiography, a non- invasive imaging modality, is frequently employed for cardiac screening in SSc. Recent advancements have enhanced the diagnostic capabilities of echocardiography, including the application of three-dimensional echocardiography and strain imaging. When echocardiography is inconclusive, CMR imaging provides detailed heart and artery images using magnetic fields and radiofrequency waves. CMR is crucial for detecting myocardial inflammation and fibrosis, and it should be used for various cardiovascular conditions, including coronary artery disease, ischemia, non- ischemic cardiomyopathy, valvular heart disease, cardiac masses, pericardial disease, arrhythmias, and congenital heart defects. It is also valuable for evaluating aortic diseases and anomalous coronary or pulmonary veins.
CMR surpasses transthoracic echocardiography (TTE) in assessing wall motion abnormalities and left ventricular ejection fraction (EF) with high-quality cine imaging. It provides additional insights through T1 and T2 mapping, extracellular volume (ECV) assessment, and myocardial perfusion imaging. CMR is preferred over radiation-based tests and iodine-based dyes due to its non-invasive nature and comprehensive tissue characterization. Newer techniques such as mapping and emerging technologies such as MR spectroscopy and fingerprinting offer deeper understanding of myocardial conditions.
CMR can evaluate diffuse interstitial myocardial fibrosis (DMF) alongside traditional late gadolinium enhancement (LGE) methods. While LGE is effective for detecting replacement fibrosis in conditions such as myocardial infarction and hypertrophic cardiomyopathy, it is less effective for DMF due to limited normal myocardium for comparison [68]. T2 mapping and ECV values are key predictors of cardiovascular complications, and advanced imaging techniques such as SPECT and PET show promise in detecting early cardiac involvement in scleroderma patients.
Laboratory investigations, including pro-BNP, cardiac troponins, and creatine kinase MB (CK- MB), are also assessed as they may indicate acute coronary syndrome or heart failure.
Autoantibodies such as antibodies to RNA polymerase III and topoisomerase I may be associated with more extensive myocardial damage. Myocardial strain imaging is employed in both CMR imaging and echocardiography [64]. For diagnosing pulmonary hypertension in patients with SSc, invasive tests such as right heart catheterization are used [69]. 24-hour Holter electrocardiogram recordings are essential for detecting conduction defects and should be performed in all symptomatic patients when a conclusive 12-lead electrocardiogram is not obtained [70].
Nailfold video-capillaroscopy (NVC) is a cost-effective method for evaluating microcirculation, particularly in the nailfolds, where it provides detailed visualization of capillary loops (Figure 6). This technique is valuable in understanding microvascular dysfunction in cardiovascular diseases, potentially revealing new therapeutic targets. NVC is especially effective in rheumatological conditions such as SSc, where it aids in diagnosis and monitoring. Most supporting evidence comes from its use in connective tissue diseases, notably PAH. Patients with PAH show reduced capillary density and increased capillary dimensions, consistent across different causes. Controlled hypertension patients also exhibit reduced baseline capillary density [71], suggesting that antihypertensive drugs may not improve microvascular function. A meta-analysis of six observational studies in SSc patients found a nonsignificant decrease in capillary density (mean difference –1.0 loops/mm; 95% CI: –2.0 to 0.0) and a significant increase in capillary width (mean difference +10.9 µm; 95% CI: 2.5–19.4) in PAH patients [46].
Figure 6
A – Early signs showing giant capillaries and hemorrhages. B – Active SSc showing hemorrhages and dilated capillaries C – Late SSc showing neoangiogenesis and areas of avascularity. D – SSc-like pattern showing giant capillaries, neoangiogenesis and dilated capillaries
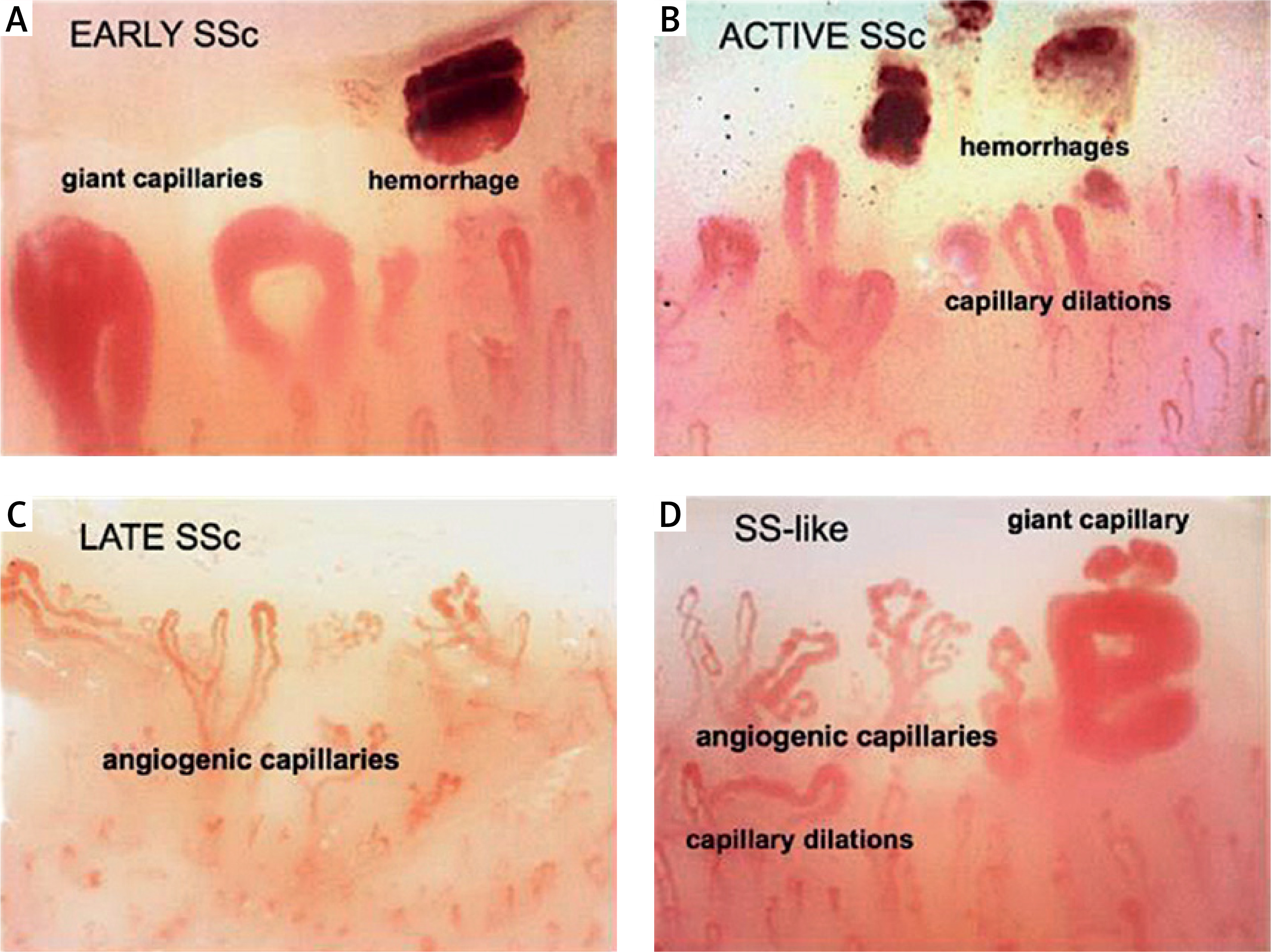
Capillary density was further reduced (mean difference –1.2 loops/mm; 95% CI: –2.3 to –0.1) in studies using right heart catheterization.
Treatment for cardiovascular manifestations primarily relies on conventional options used to manage cardiac disorders. For microvascular angina, patients should receive anti-anginal drugs, mainly including calcium channel blockers, nitrates, and aspirin [72, 73]. The use of vasodilators such as ACE inhibitors and calcium channel blockers has been associated with a positive impact on myocardial perfusion, leading to a reduction in complications [74]. Beta-blockers (excluding carvedilol) can induce Raynaud’s phenomenon and are generally avoided. NSAIDs, colchicine, and pericardial fluid drainage are employed in the treatment of pericarditis and pericardial effusion. Sodium restriction and diuretics serve as the cornerstone for managing heart failure induced by SSc [75].
Immunosuppressive therapy in the form of low-dose steroids, cyclophosphamide, or mycophenolate may be employed for SSc-induced myocarditis [32]. Endothelin receptor antagonists, proteinoids, and phosphodiesterase inhibitors, in combination with vasodilators, have improved survival in patients with pulmonary hypertension secondary to SSc. The treatment of conduction abnormalities resulting from SSc typically follows standard guidelines, involving anti- arrhythmic therapy and potentially automatic implantable cardioverter-defibrillator (AICD) implantation for patients with inducible ventricular tachycardia or reduced LVEF [35, 76].
Conclusions
Patients with SSc can exhibit many cardiac manifestations, although many cardiac issues, when present, often go unnoticed. Those with evident cardiac complications tend to have a poor prognosis. This review emphasizes the importance of early detection and management of diverse heart conditions in SSc patients. While contemporary imaging and biomarkers enhance early detection, there is ongoing development of effective therapies for cardiac complications. Timely diagnosis and intervention are critical for achieving favorable outcomes.