Introduction
Amyloidosis is a pathological condition characterized by the accumulation of insoluble fibrils in the extracellular matrix of healthy tissue [1]. Cardiac participation may ensue, resulting in a cardiomyopathy characterized by a restrictive pattern. Cardiac amyloidosis (CA) encompasses several distinct subtypes, including light-chain (AL), mutated or wild-type transthyretin (ATTRm, ATTRwt), and the less frequently encountered serum amyloid A (SAA) [2]. These subtypes are characterized by the deposition of fibrils in various cardiac locations, such as the atria, ventricles, perivascular regions, or within the cardiac valves. The preservation of ventricular function persists until the advanced stages of the ailment. CA is an infrequent and grave pathology that results from the anomalous accumulation of amyloidogenic proteins within the myocardial tissue. The condition in question has the potential to induce significant morbidity and mortality, with a median survival rate of 1–2 years after diagnosis [3]. The presence of atrial arrhythmias, specifically atrial fibrillation (AF) and atrial flutter (AFL), is common in cases of CA. The co-occurrence of these cardiac arrhythmias has the potential to exacerbate concurrent heart failure (HF) and represents a frequently encountered complication of CA. It has been reported that a substantial proportion of individuals diagnosed with CA, up to 80%, may manifest atrial arrhythmias [4]. The presence of such arrhythmias has been associated with an increased likelihood of experiencing adverse outcomes, including stroke, heart failure, and mortality [5].
In CA, the onset of diastolic dysfunction is often signaled by a diminished ability of the heart to tolerate the reduction in the atrial contribution to ventricular filling. This issue can lead to clinical decline and frequent hospital readmissions. Diastolic dysfunction in this context is frequently associated with the development of both atrial and ventricular arrhythmias and irregularities in the heart’s electrical conduction system [6]. These complications arise from the accumulation of amyloid tissue in the heart, which can interfere with the regular electrical conduction pathways and stimulate expansion of the atrial wall. This, in turn, can stimulate growth of fibrotic tissue in the heart muscle or myocardial fibrosis. The resulting changes create a cardiac environment that is more prone to the development of arrhythmias [7].
The management of atrial arrhythmias in patients afflicted with CA poses a significant challenge, primarily due to the notable diastolic dysfunction and elevated rates of atrial thrombus that are commonly observed in this population. The efficacy of atrial arrhythmia ablation, a widely accepted therapeutic intervention for ameliorating symptoms in patients with normal cardiac function or non-CA-related acquired heart disease, may not be a feasible course of action for patients afflicted with CA. Despite the limitations, the implementation of therapeutic interventions such as chemotherapy and bone marrow transplantation has significantly altered the inherent progression of the disease, underscoring the significance of proficient arrhythmia management in individuals afflicted with CA [8].
Catheter ablation has emerged as a promising therapeutic modality for patients suffering from atrial arrhythmias refractory to pharmacological interventions [9]. Presently, the safety and efficacy of catheter ablation in individuals with CA remain uncertain. Based on the existing data, it appears that patients diagnosed with CA who undergo catheter ablation may be subject to a heightened susceptibility to complications, such as pericardial effusion, tamponade, and stroke [10].
The effectiveness and safety of catheter ablation as a treatment for atrial arrhythmias in patients with cardiac amyloidosis are not fully understood. This study aimed to address this knowledge gap by reviewing existing literature and conducting a proportional meta-analysis. The goal was to provide a better understanding of the benefits and risks of catheter ablation for patients with cardiac amyloidosis. The results of this study are crucial for improving clinical practice and outcomes for those with this challenging condition.
Methods
This study was conducted following the guidelines established by Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [11].
Data sources and search strategy
Two reviewers (MA and ZZ) independently searched PubMed/Medline, Cochrane Central, and Embase databases. The researchers systematically searched for all relevant articles from the inception of these databases to May 2024. The objective was to identify studies that evaluated the efficacy and safety of catheter ablation for atrial arrhythmias in patients with cardiac amyloidosis. The search strategy consisted of the following keywords and Medical Subject Headings (MeSH) “((((Catheter ablation) OR (Ablation)) AND (Atrial arrhythmias)) AND (Amyloidosis)) OR (Cardiac amyloidosis).” The detailed search strategies used for each database are given in Supplementary Table SI.
Study selection and outcomes
The studies were considered eligible for inclusion in our meta-analysis if they fulfilled the following eligibility criteria: (a) were published randomized controlled trials (RCTs) or observational studies; (b) included adult male or female patients (≥ 18 years of age) with cardiac amyloidosis; (c) evaluated safety of catheter ablation; (d) reported at least one of the pre-specified clinical outcomes.
The outcomes included: (i) recurrence rate, (ii) re-ablation rate, and (iii) all-cause mortality.
Data extraction and quality assessment
Two reviewers (JB and ZZ) reviewed eligible articles, and only those that satisfied the predetermined inclusion criteria were selected. The disagreements were resolved by discussion with the third reviewer (MA). Redundant studies were excluded from the analysis employing Endnote X7 (Clarivate Analysis, PA). First, researchers reviewed articles based on the title and abstract, followed by a review of the full text. The data were extracted for various study characteristics, including the last name of the first author, year of publication, study design, patient groups, diagnosis and/or treatment, mean age of patients, proportion of males, total sample size, number of ablations, immediate success rate, recurrence rate, repeat ablation, complications, median follow-up, hospitalizations, mortality, survival and median time to recurrence.
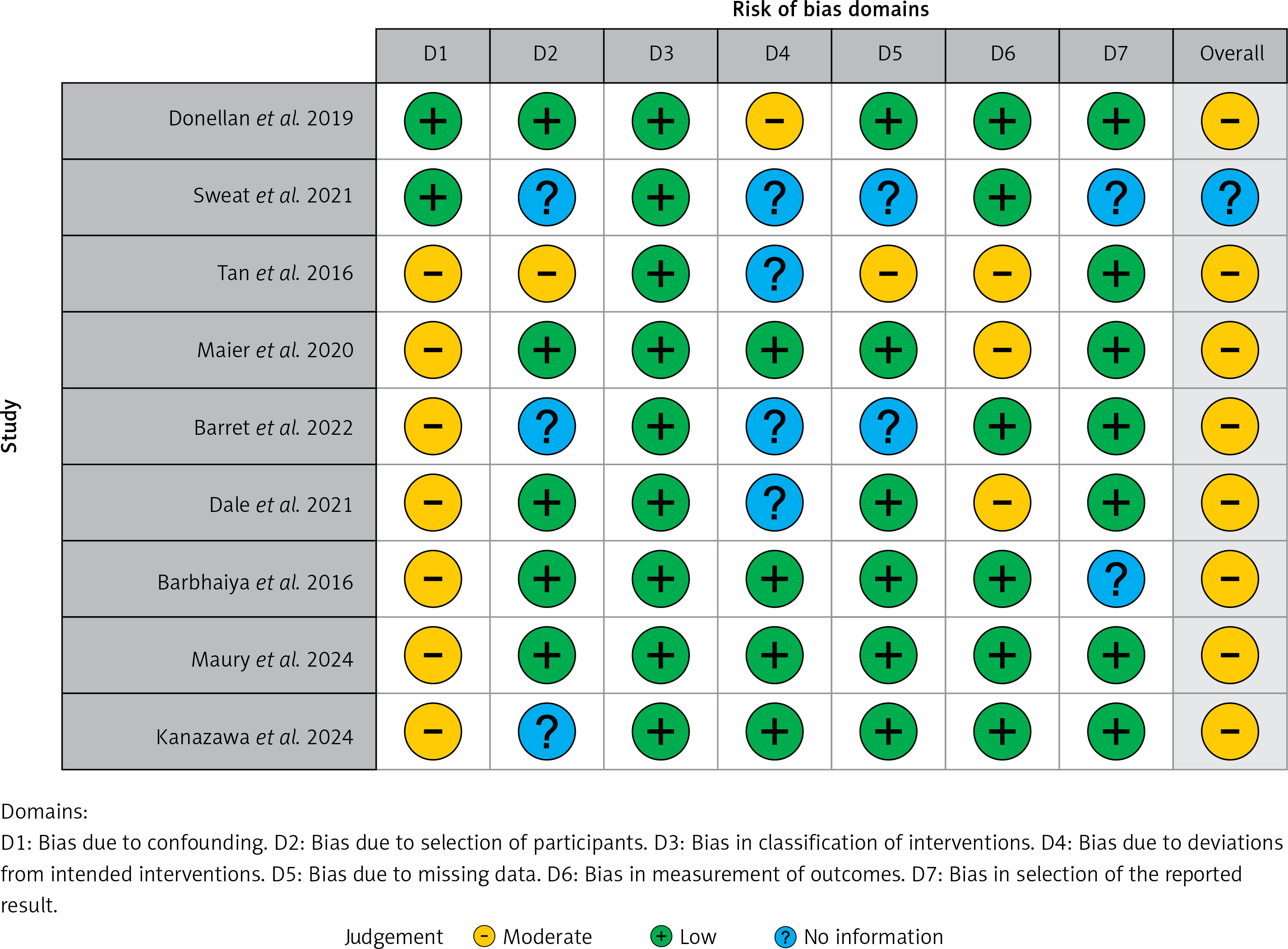
The quality assessment of the studies was performed using the Cochrane Risk of Bias in Non-randomized Studies – of Interventions (ROBINS-I) tool [12]. The ROBINS-I tool uses seven domains to determine overall bias in each non-randomized clinical trial. Studies were classified as having low, moderate, serious, or critical risk of bias. Studies that had information missing in one or more domains were classified as NI (no information).
Statistical analysis
The statistical analysis was conducted using OpenMetaAnalyst to pool untransformed proportions (PRs) along with the corresponding 95% confidence intervals (CIs). The analysis was conducted using a random effects model. Higgins I² values were used to assess heterogeneity due to variations in study methodologies and populations. A p-value of less than 0.05 was considered significant in all cases.
Results
Results of screening
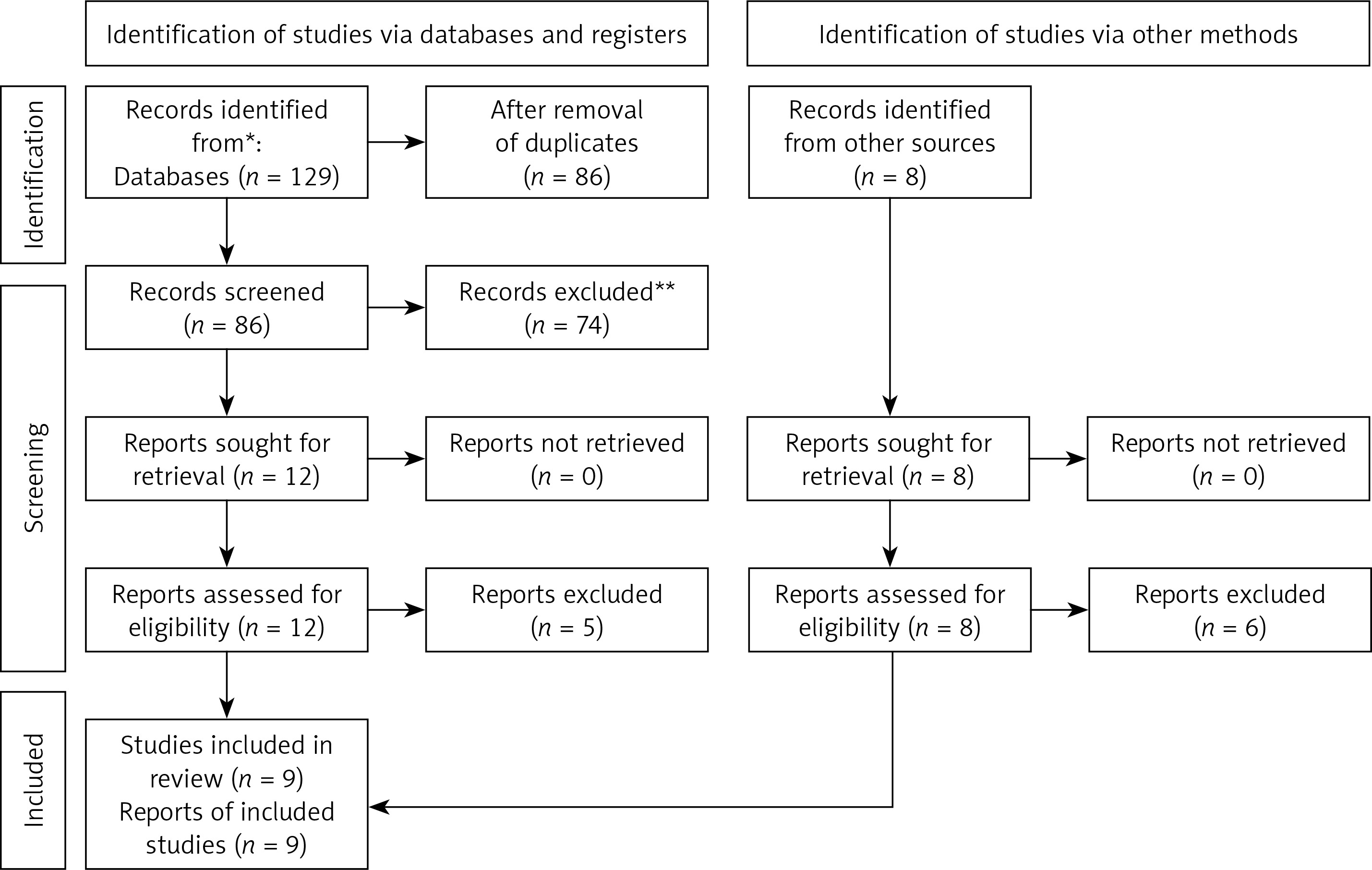
The literature search of databases yielded a total of 126 records. Eight additional studies were also identified through citation analysis and hand screening of relevant literature. A total of 134 studies were screened for eligibility. The screening was first performed based on study title and abstract, followed by full-text review. Nine studies that fulfilled the inclusion criteria were included in our meta-analysis. The details of the article screening process are provided in the PRISMA flowchart (Figure 1). The reason for exclusion of some studies that met the inclusion criteria but were still excluded from the analysis are given in Supplementary Table SII.
Characteristics of included studies
A total of nine cohort studies [13–21] were included in this systematic review and meta-analysis. The included studies had a total population size of 283 patients, of whom 77% were male. The studies were published between 2016 and 2024. The mean age of patients ranged from 67.6 to 76.5 years. The median follow-up period for the included studies ranged from 13 to 60 months. The details of the included studies and patients’ characteristics are provided in Table I.
Table I
Baseline characteristics of included studies and patients
The quality assessment of the included studies was performed using ROBINS-I, which showed an overall moderate risk of bias. The traffic light plots for ROBINS-I are given in Figure 2. The funnel plot for the primary outcome of recurrence rate is given in Supplementary Figure S1.
Recurrence and re-ablation rates
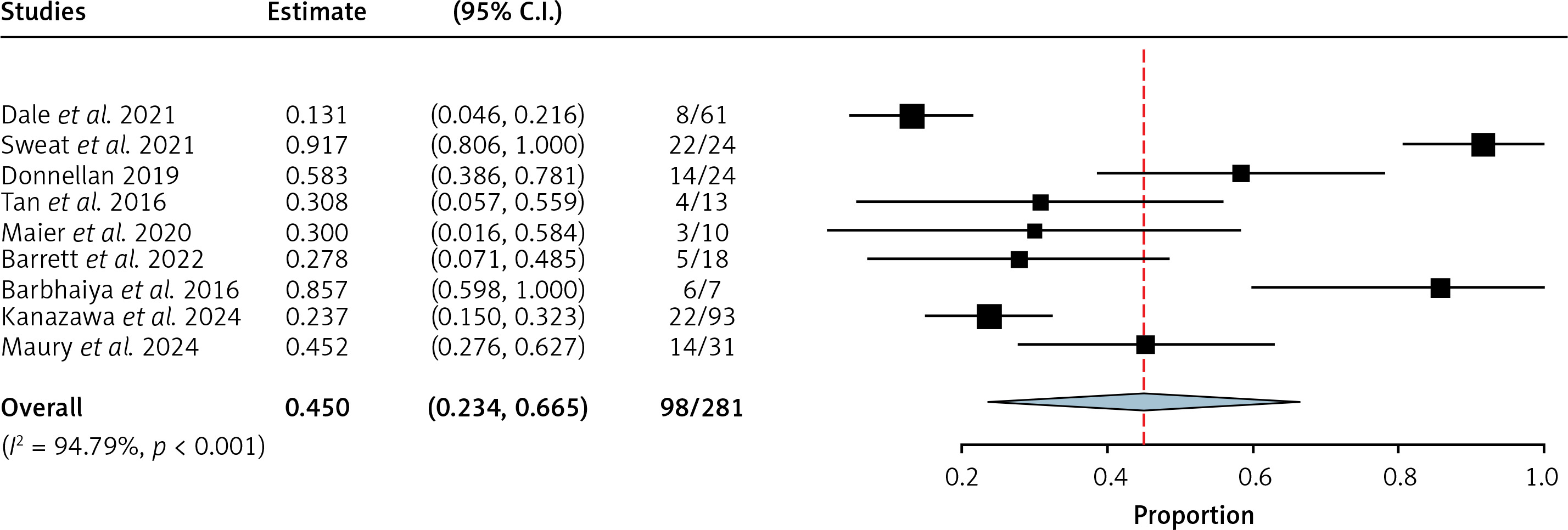
Data for recurrence were reported by 9 studies (n = 281). The pooled incidence of recurrence of cardiac arrhythmia following catheter ablation was 45% (95% CI = 23.4% to 66.5.%, I2 = 94.79%, Figure 3).
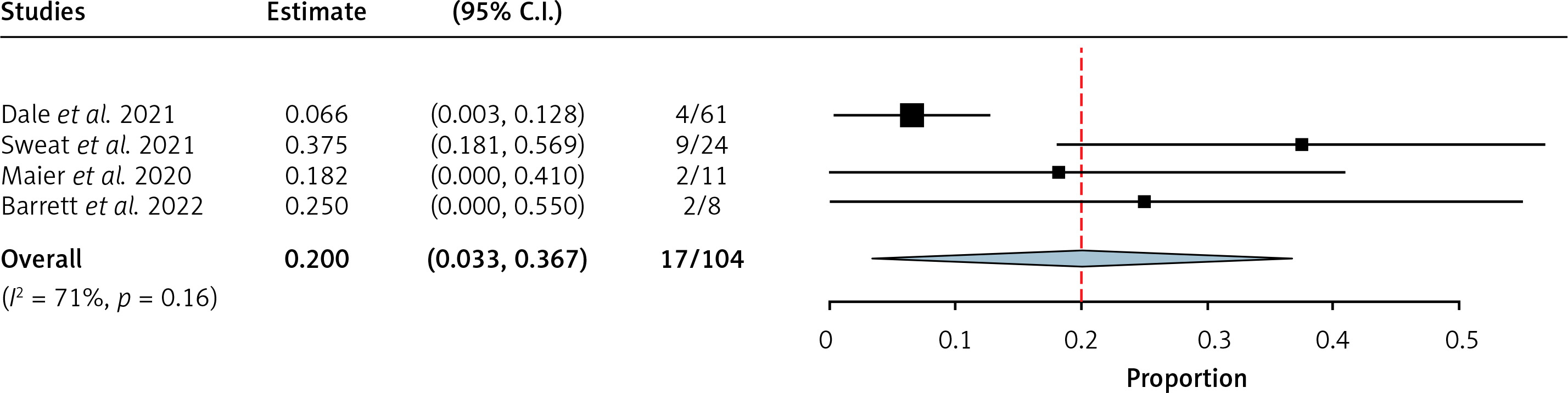
Data for re-ablation were reported by 4 studies, comprising a total sample size of 104. The pooled incidence for re-ablation was 20% (95% CI = 3.3% to 36.7%, I2 = 71%, Figure 4) following the initial treatment.
All-cause mortality
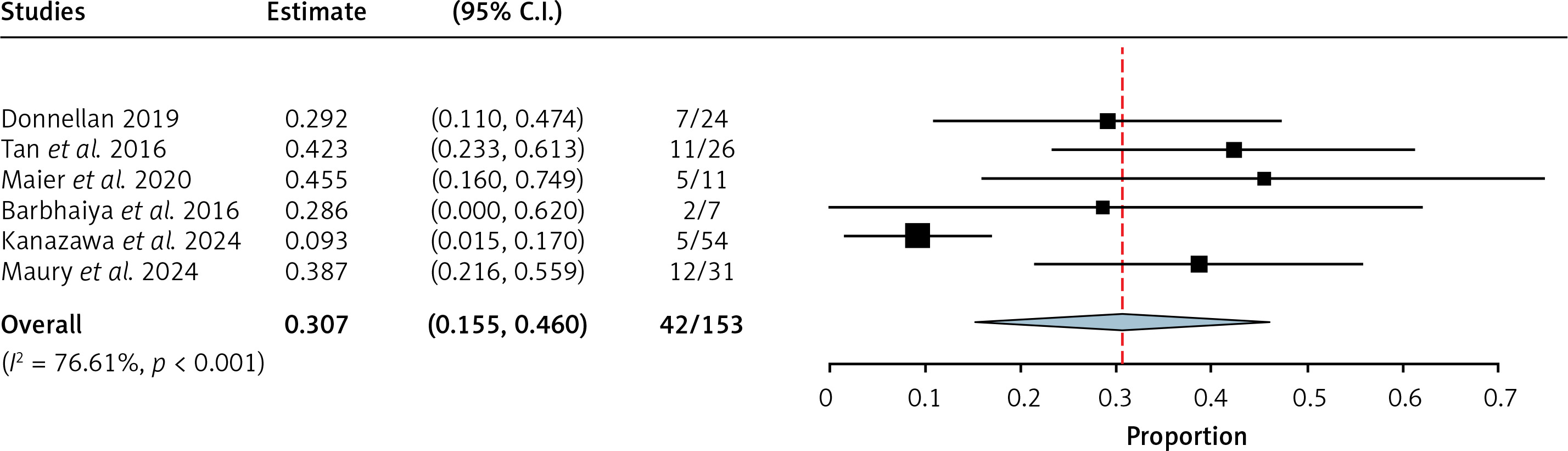
Data for all-cause mortality were reported by 3 studies, with a net sample of 153. The pooled incidence of all-cause mortality was 30.7% (95% CI = 15.5% to 46%, I2 = 76.61%, Figure 5) in the CA patients who underwent ablation.
Discussion
The findings showed that catheter ablation may be an effective treatment option for patients with cardiac amyloidosis and atrial arrhythmias. However, the high recurrence rates following catheter ablation are a concern, with a pooled incidence of 45%. There are several possible reasons for the high recurrence rates in this population. One possibility is that the amyloid deposits in the heart muscle make it difficult to ablate all the arrhythmia-causing tissue. Another possibility is that the amyloid deposits may grow over time, even after the ablation procedure. The decision of whether to undergo the procedure should be made on a case-by-case basis, after carefully considering the patient’s risks and benefits. This also suggests the possibility of variance in the patient cohorts, research methodologies, or interventions applied among the encompassed studies. Moreover, the comparatively modest rates of re-ablation succeeding the primary treatment imply that catheter ablation may confer certain advantages, albeit not completely eradicating arrhythmias. The high heterogeneity in the recurrence rate results suggests that there may be differences in the patient populations, study designs, or interventions used across the included studies. Despite undergoing the ablation procedure, complete elimination of factors causing arrhythmias cannot be guaranteed, leading to a high recurrence rate and subsequent re-ablation, which poses a significant concern for amyloidosis patients. This can have detrimental effects on their quality of life and increase the risk of mortality.
Black-Maier and Tan et al. reported 40% and 75% recurrence-free survival in their respective CA-AT/AF cohorts at 1 year, but their studies were limited in scope and underpowered due to small sample sizes and including patients with all types of atrial arrhythmias [16, 18]. In conclusion, patients with CA-AF have a higher risk of recurrence of AT/AF compared to non-CA-AF patients. Previous studies have reported varying rates of recurrence-free survival, with the most comprehensive study to date, by Donnellan et al. [15], showing a 58% recurrence rate at 3 years. However, this study was limited in scope to patients with ATTR-CA and compared to a medically treated cohort rather than a matched non-CA group. Although the results were not statistically significant, the finding that patients with cardiac amyloidosis have a higher all-cause mortality compared to controls is significant. This implies that patients with cardiac amyloidosis may be at a higher risk for mortality, which could influence treatment decisions. Interestingly, patients with atrial arrhythmias had lower all-cause mortality compared to those with AV nodal arrhythmias, indicating that the type of arrhythmia may impact mortality risk in patients with cardiac amyloidosis. The findings of the direct comparison between catheter ablation and medical management for atrial arrhythmias in cardiac amyloidosis are encouraging, suggesting that catheter ablation may provide a survival benefit and improved outcomes compared to medical management alone. These findings are further supported by the Cox proportional hazards analysis, which indicates that catheter ablation may be an important treatment option for these patients [15]. However, it is important to note that this direct comparison study involved a relatively small sample size and may be subject to certain limitations that could affect the generalizability of the results. For example, the study may not have adequately accounted for confounding factors or differences in patient characteristics that could have influenced outcomes.
There are several limitations of our study. The analysis included studies having variable follow-up durations which could have impacted the incidence of recurrence rates and re-ablation rates. The small sample size and observational nature of included studies may not have adequately accounted for confounding factors and other differences in patient characteristics that could have influenced patient outcomes. The significant heterogeneity could affect the generalizability of the results.
In conclusion, the study’s results suggest that catheter ablation may be a promising treatment option for patients with cardiac amyloidosis and atrial arrhythmias. However, the high recurrence rates following the procedure and the limited evidence available in the literature underscore the need for more research to better understand the factors that influence outcomes. Further research is needed to fully understand the long-term outcomes of catheter ablation in this patient population. It is important to consider the limitations of this study when interpreting its findings and making clinical decisions for individual patients.