
Endovascular abdominal aortic aneurysm repair (EVAR) has been widely adopted as the preferable method to treat aneurysmal disease. A variety of different endografts are currently available to deal with diverse anatomies. Although accumulating experience has led to a high level of technical success, occasionally technical troubleshooting may arise, and special handling may be necessary [1–3]. Herein, we report on such a particular troubleshooting technique during EVAR.
An endograft with a suprarenal stent was placed in a patient with a 5 cm-sized abdominal aortic aneurysm. The anatomy was favorable and within the instructions for use of the graft. After deployment of the main body and placement of the contralateral limb, an inability to retract the delivery system was realized (green-yellow arrow). It seemed that the delivery system was blocked at the flow divider level for unknown reasons (green-yellow star). This issue occurred despite favorable anatomy and within the instructions for use of the graft. While the problem was encountered with this specific device, similar issues have been reported with other endografts. Factors such as iliac tortuosity, small aortic diameter, or increased friction at the flow divider level may contribute to such complications by hindering smooth retraction of the delivery system. Attempts to release it by forward and backwards movements were futile and as they were pushing the whole graft up and down, they resulted in endograft distal migration. The problem was solved after the insertion of a molding balloon at the contralateral side, just distally to the flow divider level. It was inflated enough to stabilize the main body (light blue arrow). Equal bidirectional forces were applied in the delivery system ipsilaterally (upward direction) and in the molding ballon contralaterally (backward direction). This bidirectional maneuver allowed for excessive force to be applied in both items without jeopardizing the stability of the whole graft. Excessive force achieved the upward release of the delivery system. Subsequently, it was easily retracted and removed. Afterwards, an aortic cuff was placed proximally to fix the initial endograft migration. The principle behind this bidirectional maneuver is that by simultaneously applying opposing forces – one stabilizing the graft distally with the molding balloon and the other releasing the delivery system proximally – the system can be disengaged without transmitting destabilizing forces to the main body of the endograft. This controlled force distribution minimizes the risk of graft displacement while effectively resolving the blockage. Imaging with computed tomography angiography on the 2nd postoperative day was normal, and the patient was discharged. Although early imaging was reassuring, mid- and long-term follow-up remains essential to ensure the durability of the repair. A follow-up CTA at 1 and 6 months was planned to assess for late migration, stent integrity, and overall endograft performance.
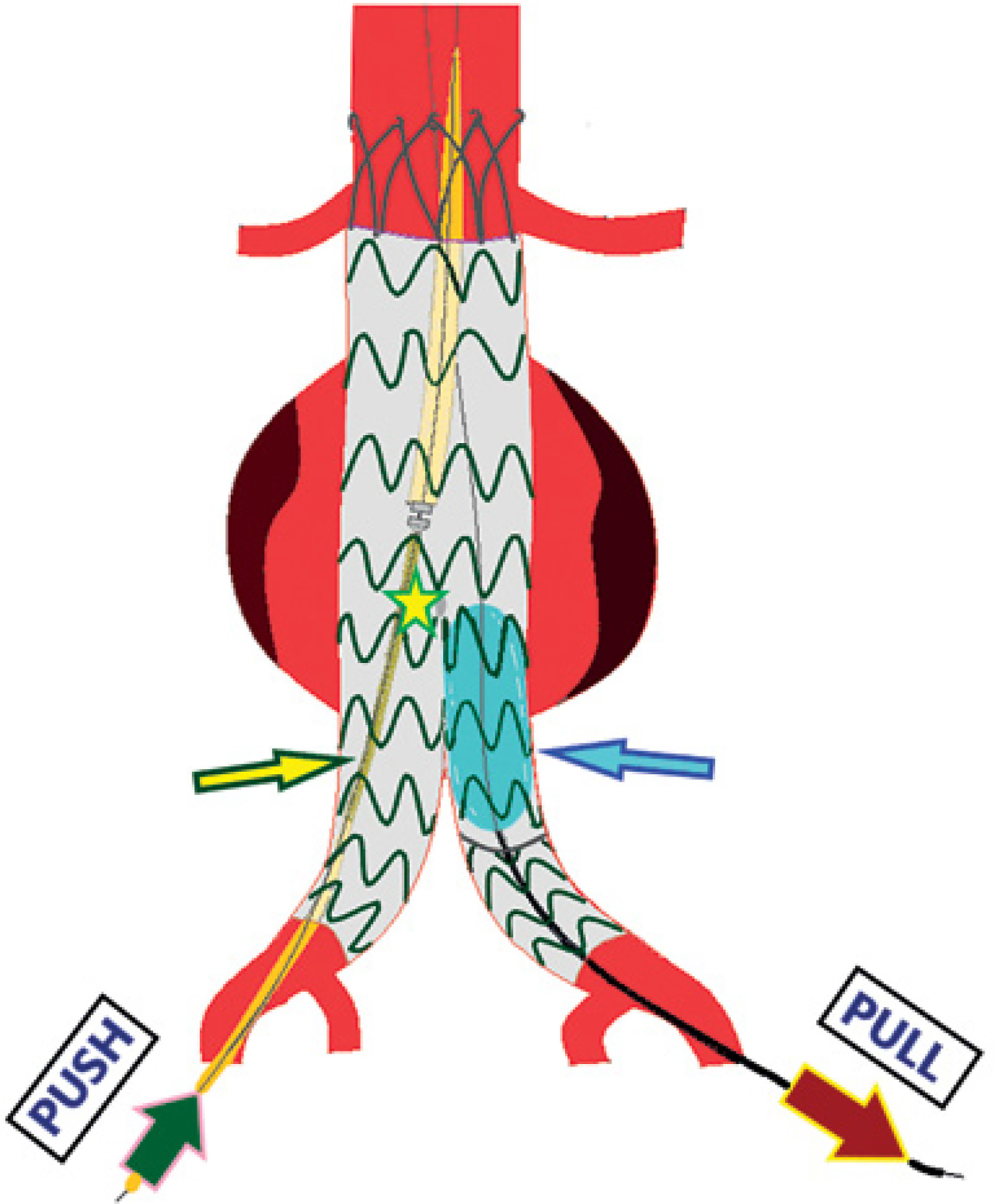
Figure 1
A troubleshooting technique to release the blocked delivery system at the flow divider level. It includes simultaneous pushing up of the delivery system (deep green arrow) and pulling down of an inflated contralateral molding balloon (maroon arrow). Excessive strength is applied in both sides, without jeopardizing the stability of the main body. This maneuver achieved the upward release of the delivery system and subsequently easy withdrawal
While this maneuver successfully resolved the issue, excessive force application carries inherent risks, including potential vessel wall injury, fabric tearing, or unintentional endograft migration. In this case, the bidirectional force approach helped distribute the applied stress evenly, mitigating these risks. However, careful intraoperative assessment is essential to ensure that force is applied in a controlled and measured manner to prevent unintended complications.
Alternative techniques such as guidewire-assisted retrieval or different balloon configurations could also be considered [2, 3]. The bidirectional force technique was selected due to its ability to maintain stability while effectively disengaging the delivery system. As with any troubleshooting technique, there is a balance between applying sufficient force to resolve the complication and avoiding excessive stress on the graft [1, 2]. This technique minimizes the risk of uncontrolled graft displacement but should be applied cautiously to prevent unintended structural alterations to the endograft.
Given that significant force was required to free the delivery system, structured follow-up imaging is necessary to rule out delayed complications such as migration or structural fatigue of the stent-graft material. This highlights the importance of post-EVAR surveillance protocols, particularly in cases where intraoperative troubleshooting was required.