
Pleural calcification or pleuritis calcarea, often presenting as calcified pleural plaques, is a clinical entity commonly associated with prior asbestos exposure [1]. However, it may also arise from other causes, such as previous infections like tuberculosis or empyema, chronic inflammatory conditions, trauma, or hemothorax. Several cases of pleural calcifications in patients with end-stage renal disease have also been reported [2, 3]. In some cases, pleural calcifications may develop idiopathically without any identifiable etiology. While these calcifications are frequently asymptomatic and incidentally discovered on imaging, they can occasionally present with symptoms such as chest pain or dyspnea [4–6].
The differential diagnosis for pleural calcifications is broad and includes malignant pleural mesothelioma, pleural metastases, and chronic pleuritis [6, 7]. Furthermore, conditions such as pleural thickening secondary to infections or autoimmune diseases like systemic lupus erythematosus and rheumatoid arthritis can mimic calcified pleura [8]. Differentiating between these conditions requires a combination of imaging studies, clinical history, and, when necessary, histopathological examination. Accurate diagnosis is critical as misdiagnosis can lead to delayed or inappropriate management [9–12]. This report discusses the case of a patient with extensive bilateral pleural plaques and no known history of asbestos exposure, highlighting the diagnostic process and the importance of distinguishing benign calcified pleural conditions from malignant or infectious causes.
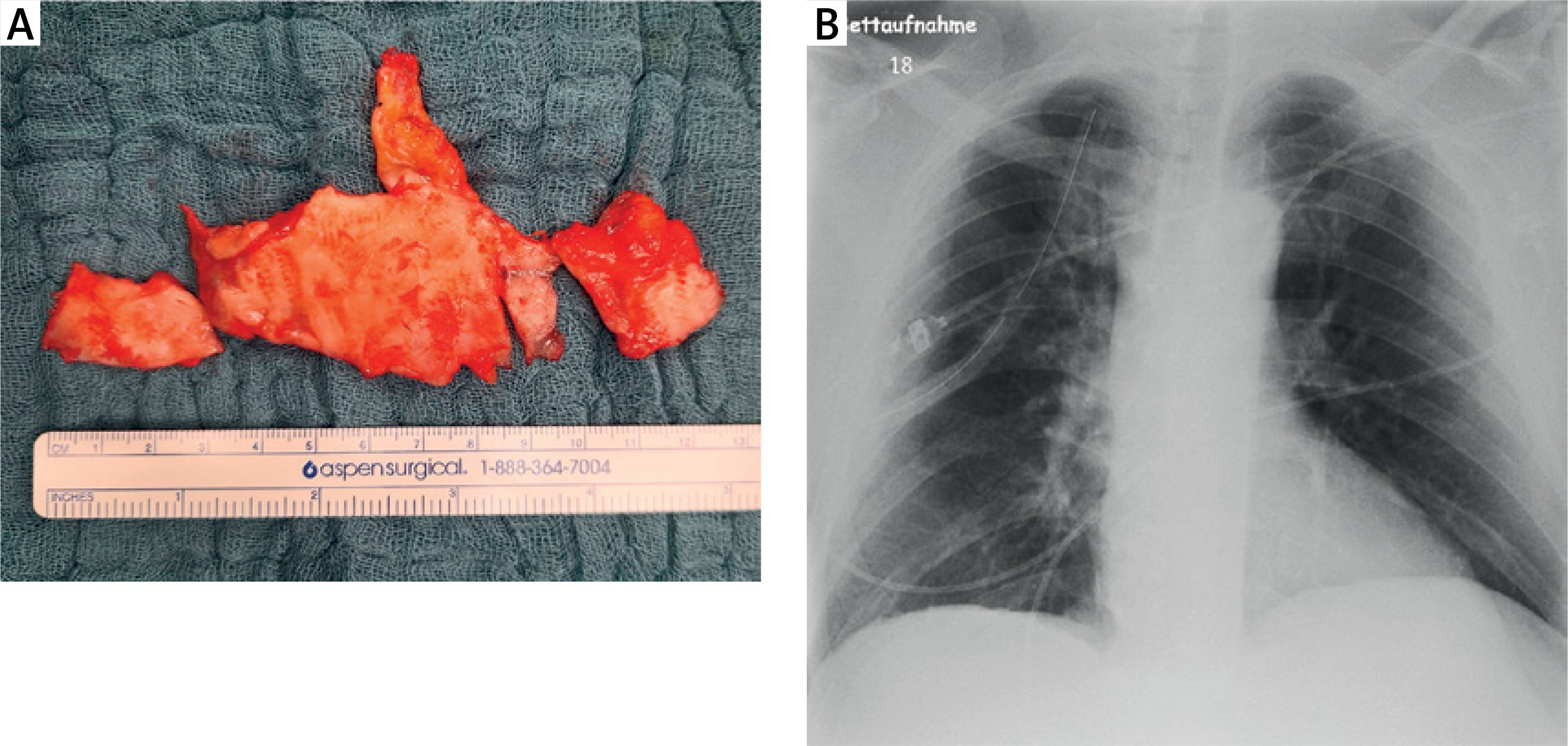
A 60-year-old male presented with a history of chest pain and shortness of breath that had persisted in the past 8 months. His medical history was significant for chronic obstructive pulmonary disease (COPD) classified as GOLD stage II, coronary artery disease for which he had undergone percutaneous transluminal coronary angioplasty (PTCA) with stent placement earlier in the year, and arterial hypertension. Imaging studies revealed extensive bilateral pleural plaques suggestive of pleuritis calcarea (Figure 1). The patient denied any known history of asbestos exposure but reported a 15-year occupational history of working in foundries beginning 40 years ago. Preoperative echocardiography revealed a normal-sized, concentrically hypertrophied left ventricle with good systolic function. The right ventricle was of normal size and exhibited good pump function. The heart valves appeared morphologically normal with no significant findings on Doppler imaging. There was no evidence of pericardial effusion, and pulmonary artery pressure could not be assessed due to the absence of tricuspid insufficiency. On admission, the patient’s symptoms and imaging findings warranted further investigation through surgical intervention. After appropriate preoperative preparation, he underwent uniportal video-assisted thoracoscopy (VATS). Intraoperative findings confirmed extensive calcified plaques on the parietal pleura (Figure 2). Pleurectomy and biopsies were performed without complications, and the patient’s immediate postoperative course was stable. Histological analysis revealed pronounced band-like fibrosis and sclerosis consistent with pleural plaques, with minimal chronic nonspecific inflammation. Importantly, there was no evidence of malignancy. Postoperatively, the patient’s recovery was uneventful. A chest drain inserted during the surgery produced serous fluid and was removed on the 2nd postoperative day. By the 3rd postoperative day, the patient was discharged in stable condition. At discharge, his wounds were healing well, and he reported no further symptoms.
Figure 1
Computed tomography (CT) scan images showing calcified plaques in the parietal pleura (arrows). A – Transverse plane scan of the thoracic cavity. B – Coronal reconstruction highlighting the distribution of pleural plaques
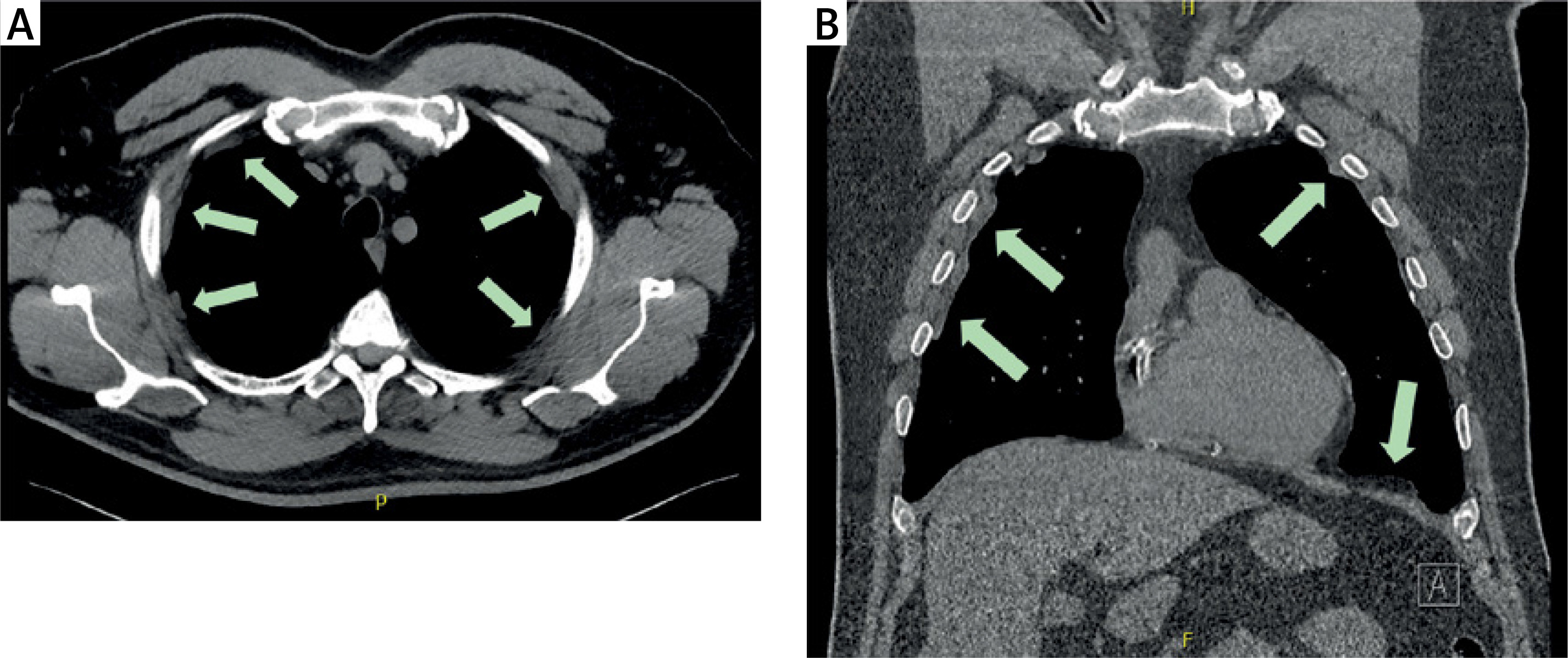
Figure 2
A – A section of the parietal pleura with representative calcified plaques, resected for histological examination. B – Postoperative chest X-ray showing no evidence of pneumothorax or hemothorax
Pleural calcification, as seen in the presented case, is a rare and often underrecognized entity [6–9]. While commonly linked to asbestos exposure, its presence in patients without such exposure necessitates consideration of alternative etiologies and a comprehensive differential diagnostic approach [7]. This is particularly important as pleural calcifications can mimic a range of benign and malignant pleural diseases.
Differential diagnosis and mimicking conditions: The differential diagnosis for pleural calcification includes both benign and malignant diseases (Table I). Malignant pleural mesothelioma is a primary consideration, especially when calcified plaques are present [10]. Mesothelioma often presents with nonspecific symptoms such as chest pain and dyspnea, much like pleural plaques, and can be associated with asbestos exposure [4, 7]. The absence of asbestos exposure in this case highlights the need to carefully evaluate imaging and histological findings to rule out malignancy. Similarly, metastatic pleural disease, arising from primary cancers such as lung, breast, or gastrointestinal malignancies, may present with pleural thickening or plaques, mimicking calcified pleura [6, 13–16].
Table 1
Comprehensive categorization of malignant and benign etiologies of pleural thickening and disease
Benign conditions, including chronic pleuritis and pleural thickening secondary to tuberculosis or bacterial empyema, must also be considered [6]. These conditions can lead to localized or diffuse pleural scarring and calcification, with imaging findings that overlap significantly with those of calcified plaques [15]. Autoimmune diseases, such as systemic lupus erythematosus, rheumatoid arthritis, or scleroderma, can also cause pleural thickening and effusions, further complicating the diagnostic process [6, 9].
Additionally, conditions such as pleural effusions from congestive heart failure, trauma-related hemothorax, or prior thoracic surgeries may result in pleural fibrosis and calcifications over time. Idiopathic pleural calcifications, though rare, remain a diagnosis of exclusion and should only be considered after other potential causes have been thoroughly ruled out [6–9].
Importance of clinical suspicion and diagnostic approach: In the presented case, the absence of asbestos exposure, coupled with the patient’s occupational history of working in foundries, raised a clinical suspicion of alternative etiologies. Occupational exposures to other industrial dust and particulates may also contribute to pleural abnormalities, though their direct link to calcified plaques remains less well established compared to asbestos [13]. Foundry workers are often exposed to metal fumes, silica, and other airborne particulates, which have been associated with chronic pulmonary and pleural changes. While a direct link between foundry work and pleural calcifications is less well established than with asbestos exposure, studies have suggested that prolonged exposure to certain industrial pollutants may contribute to pleural fibrosis and plaque formation [13]. Further research is warranted to clarify the impact of these exposures on pleural health.
The diagnostic pathway in such cases requires a systematic approach, integrating clinical history, radiological evaluation, and histopathological confirmation. High-resolution computed tomography (CT) is the imaging modality of choice for detecting pleural calcifications. It provides detailed visualization of calcified plaques, distinguishing them from other pleural diseases such as diffuse thickening or malignant infiltration [14–16]. Radiologically, benign pleural calcifications typically present as focal or diffuse plaques along the parietal pleura, often with a characteristic ‘holly-leaf’ pattern on CT. These calcifications tend to be well demarcated and do not invade the adjacent lung parenchyma. In contrast, malignant pleural thickening, as seen in mesothelioma or metastatic disease, may appear as irregular, nodular pleural deposits, frequently associated with soft tissue masses and pleural effusions. The presence of circumferential pleural thickening greater than 1 cm and involvement of the mediastinal pleura raises concern for malignancy. These distinguishing features are critical in differentiating benign from malignant pleural processes and guiding the need for further histopathological evaluation [14–16]. However, imaging alone cannot differentiate between benign and malignant conditions, necessitating histological examination through invasive procedures like video-assisted thoracoscopy (VATS).
In this case, the decision to proceed with VATS allowed for direct visualization and biopsy of the affected pleura, confirming the benign nature of the calcifications. This step is critical in excluding malignancy and establishing a definitive diagnosis, particularly when clinical and imaging findings are ambiguous.
Broader implications and clinical relevance: This case underlines the need for heightened clinical suspicion in patients presenting with pleural abnormalities, even in the absence of classical risk factors like asbestos exposure [1, 6, 15]. It also highlights the importance of a multidisciplinary approach involving pulmonologists, radiologists, and thoracic surgeons to ensure accurate diagnosis and management.
Beyond diagnosis, understanding the clinical implications of pleural calcifications is essential. While typically benign, extensive calcifications can lead to restrictive lung disease, contributing to symptoms such as dyspnea [5]. Long-term monitoring may be warranted in such cases to detect any functional impairment or progression of symptoms.
Although pleural calcifications are typically benign, their clinical significance extends beyond diagnosis. In some patients, extensive calcifications may contribute to restrictive lung disease, leading to progressive dyspnea over time. Long-term follow-up with pulmonary function tests may be warranted, particularly in patients with pre-existing lung disease. Additionally, monitoring for symptom progression is important to differentiate benign calcifications from evolving malignant processes. Further studies are needed to establish long-term prognostic outcomes in patients with idiopathic or non-asbestos-related pleural calcifications.
Finally, this case reinforces the importance of considering occupational and environmental exposures beyond asbestos in patients with pleural diseases. It also emphasizes the role of histopathological evaluation in distinguishing between benign and malignant pleural conditions. By adopting a thorough and systematic approach, clinicians can reduce diagnostic uncertainty and provide optimal care for patients with pleural calcifications or related conditions. Pleural calcifications represent a diagnostic challenge due to their potential to mimic a wide range of pleural diseases. This case highlights the critical role of the clinical suspicion, detailed imaging, and histopathological confirmation in establishing an accurate diagnosis. A systematic and multidisciplinary approach to the differential diagnosis, considering both benign and malignant etiologies, ensures timely and appropriate management, ultimately improving patient outcomes.