
Coronary artery disease (CAD) remains one of the leading causes of morbidity and mortality worldwide, particularly in patients with multiple comorbidities and impaired left ventricular function [1]. In advanced cases, where ischemic cardiomyopathy is complicated by ventricular aneurysms and intracardiac thrombi, surgical intervention becomes both challenging and critical. Apical left ventricular aneurysms, often a result of transmural myocardial infarction, can lead to progressive ventricular dysfunction because of the disruption of the normal geometrical shape of the ventricle, thromboembolism, and life-threatening arrhythmias [2]. In such cases, a combination of myocardial revascularization, thrombectomy, and ventricular reconstruction may offer significant clinical benefits by improving cardiac function and reducing associated risks [3]. This case report describes the successful management of a 67-year-old patient with coronary three-vessel disease, an apical left ventricular aneurysm with a thrombus, and a severely reduced left ventricular ejection fraction (LVEF). The patient underwent triple arterial coronary bypass grafting, left ventricular thrombectomy, and ventricular reconstruction according to the Dor procedure. This report highlights the surgical approach, perioperative management, and postoperative outcomes, illustrating the role of a multidisciplinary strategy in managing complex cardiac pathologies.
A 67-year-old male patient with a history of coronary three-vessel disease and an apical left ventricular aneurysm presented for elective myocardial revascularization. The patient’s preoperative left ventricular function was severely impaired, with an ejection fraction (LVEF) of 20%. His past medical history was significant for peripheral arterial occlusive disease (PAOD) stage I without symptoms, chronic bronchitis with a known pulmonary lesion in the right lower lobe, congenital obstructive defects of the renal pelvis and ureters, suspected asthma, iodine-deficiency thyroid disease with a history of thyroidectomy, type 2 diabetes mellitus, gout, and essential hypertension. The patient had been under regular cardiologic evaluation, where an unclear mass at the left ventricular apex was discovered (Figure 1). Computed tomography (CT) scan confirmed the presence of a ventricular aneurysm (Figure 2). The patient did not report symptoms such as angina pectoris, syncope, or exertional dyspnea. Echocardiography revealed a severely reduced left ventricular function with significant septal hypokinesia and an apical aneurysm containing a rounded thrombus. Coronary angiography confirmed coronary three-vessel disease, including distal left main stenosis, occlusion of the proximal left anterior descending artery (LAD), retrograde collateralization via the right coronary artery (RCA), and ostial stenosis of the right ventricular branch (Figure 3). The patient underwent surgery under general anesthesia and median sternotomy, cardiopulmonary bypass was established without complications. The surgical procedure included triple arterial coronary bypass grafting, thrombectomy of the left ventricle, and left ventricular reconstruction according to the Dor procedure. The left internal mammary artery (LIMA) was harvested as an in-situ graft and anastomosed to the LAD, and the right internal mammary artery (RIMA) was harvested as free graft and sequentially grafted as a T-graft to the diagonal and obtuse marginal branches. Following the bypass grafting, the left ventricle was longitudinally opened at the apical aneurysm site parallel to the LAD. The thrombus, partially encapsulated in fibrous tissue, was removed entirely. Subsequently, a pericardial patch (2 × 2 cm) was sutured to the transitional zone of the scarred ventricle, and the ventricular apex was reconstructed using Teflon strips (Figure 4). The procedure was completed without complications, and the heart exhibited improved contraction post-reconstruction. The postoperative course was uneventful. The patient was extubated on the first postoperative day following uncomplicated weaning from mechanical ventilation. He remained hemodynamically stable under intensive care monitoring. On the second postoperative day, the patient was transferred to the general ward, where mobilization was initiated and progressed well. Postoperative transthoracic echocardiography revealed an improvement in systolic left ventricular function, though it remained severely impaired with an ejection fraction of 30%. A relaxation disturbance of the diastolic function was also noted. Given the significant hypokinesia and persistently reduced LVEF, the patient was at elevated risk for malignant arrhythmias. Therefore, a wearable cardioverter-defibrillator (LifeVest) was prescribed for three months, with re-evaluation for implantable cardioverter-defibrillator (ICD) placement in line with current guidelines. On the 8th postoperative day, the patient was discharged in stable condition. A rehabilitation program was organized to support his recovery and optimize functional outcomes. The clinical follow-up will include cardiac function monitoring and reassessing ICD implantation after 3 months.
Figure 1
Echocardiographic diagnosis of the left ventricular aneurysm located in the apical anterior wall with evidence of thrombotic material. A – Transthoracic echocardiography in the 4-chamber view showing the aneurysm. B – Transthoracic echocardiography in the 2-chamber view confirming the aneurysm and thrombus. C – Transesophageal echocardiography demonstrating the adherent thrombus in the thin anterior wall. D – Transgastric transesophageal echocardiography illustrating the clot within the aneurysmatic region
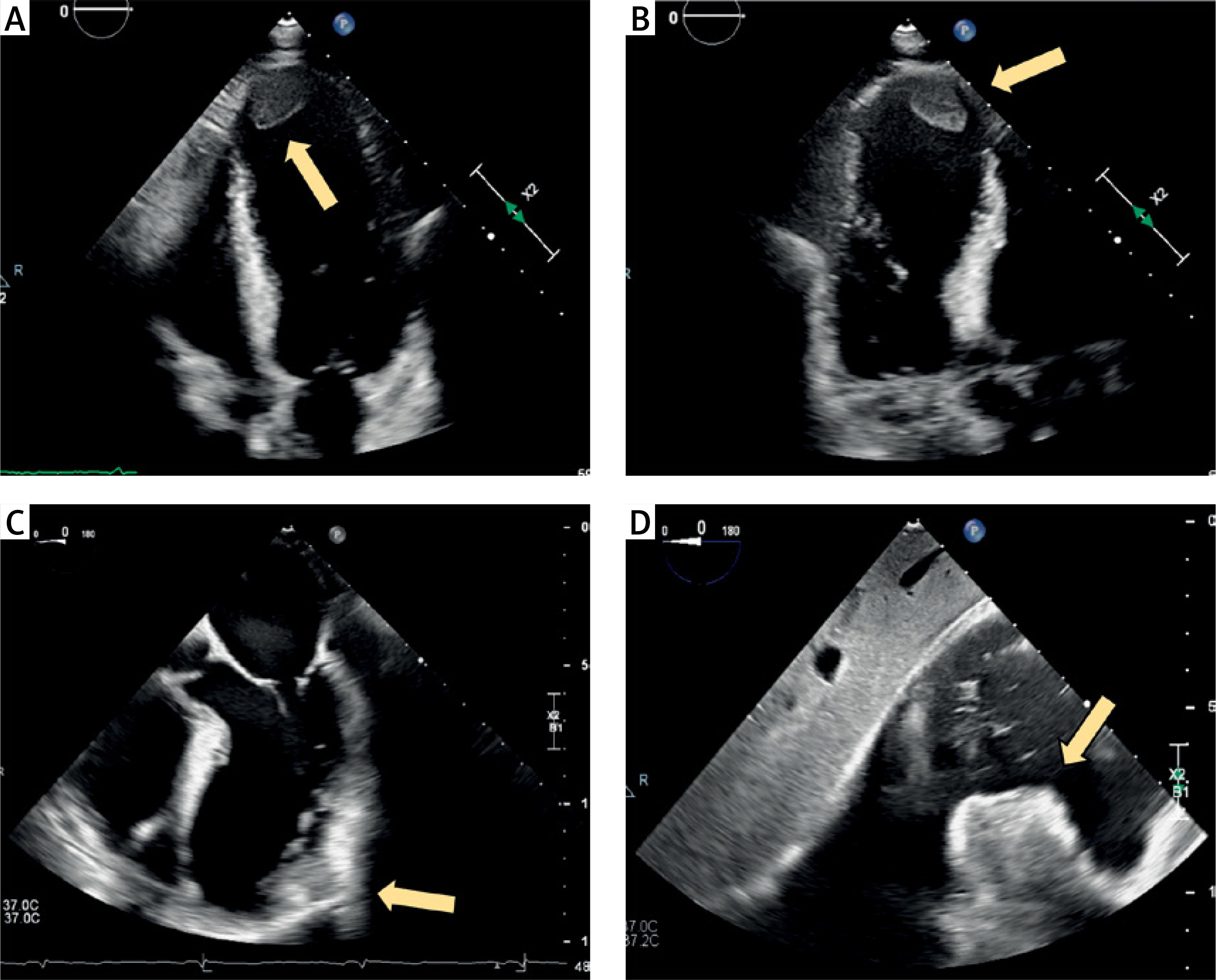
Figure 2
Computed tomography (CT) scans depicting the left ventricular aneurysm. A – Transverse plane section highlighting the ventricular aneurysm. B – Coronal reconstruction providing a detailed view of the aneurysm morphology
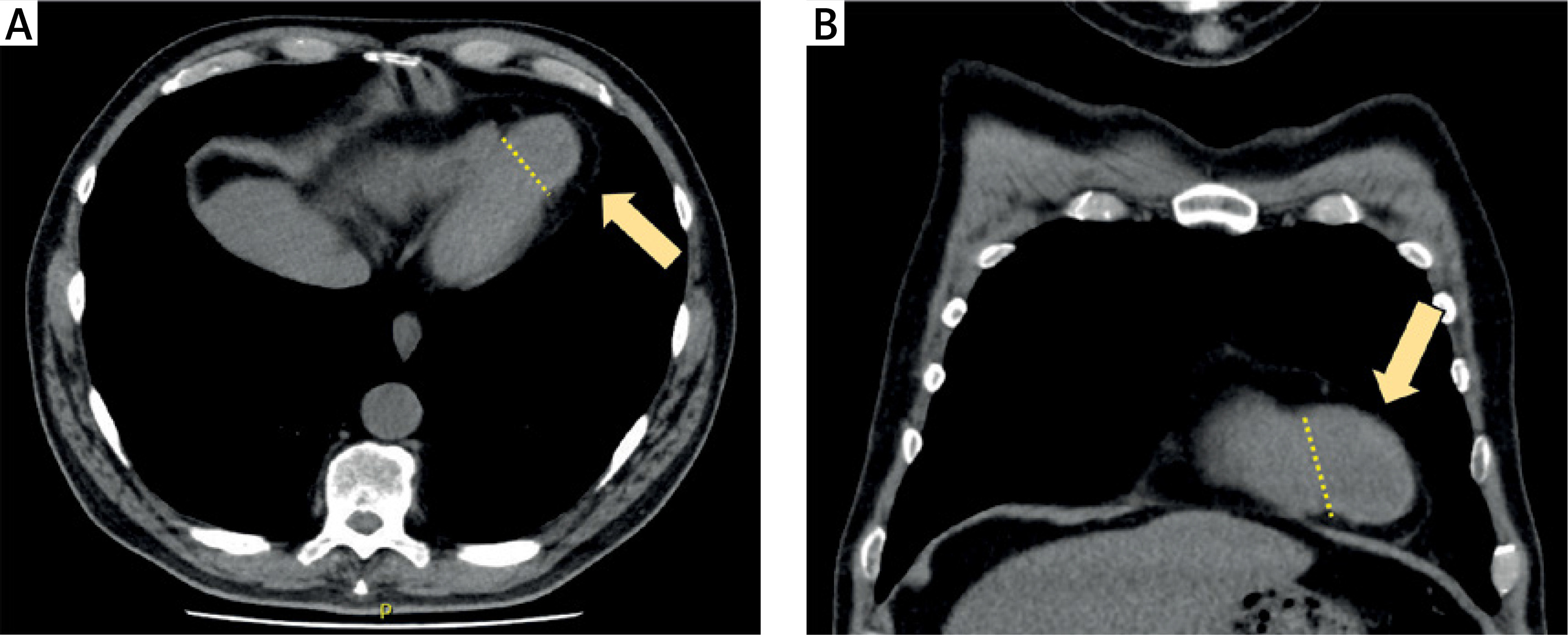
Figure 3
Coronary angiography findings of coronary three-vessel disease. A – The right coronary artery (RCA) showing stenosis of the right ventricular branch (arrow). B – Retrograde perfusion of the occluded left anterior descending artery (LAD) through collateral circulation via the RCA (arrows). C – Stenosis of the distal left main coronary artery (arrow). D – Complete occlusion of the proximal LAD. E, F – Occlusion of the LAD confirmed in a different angiographic projection
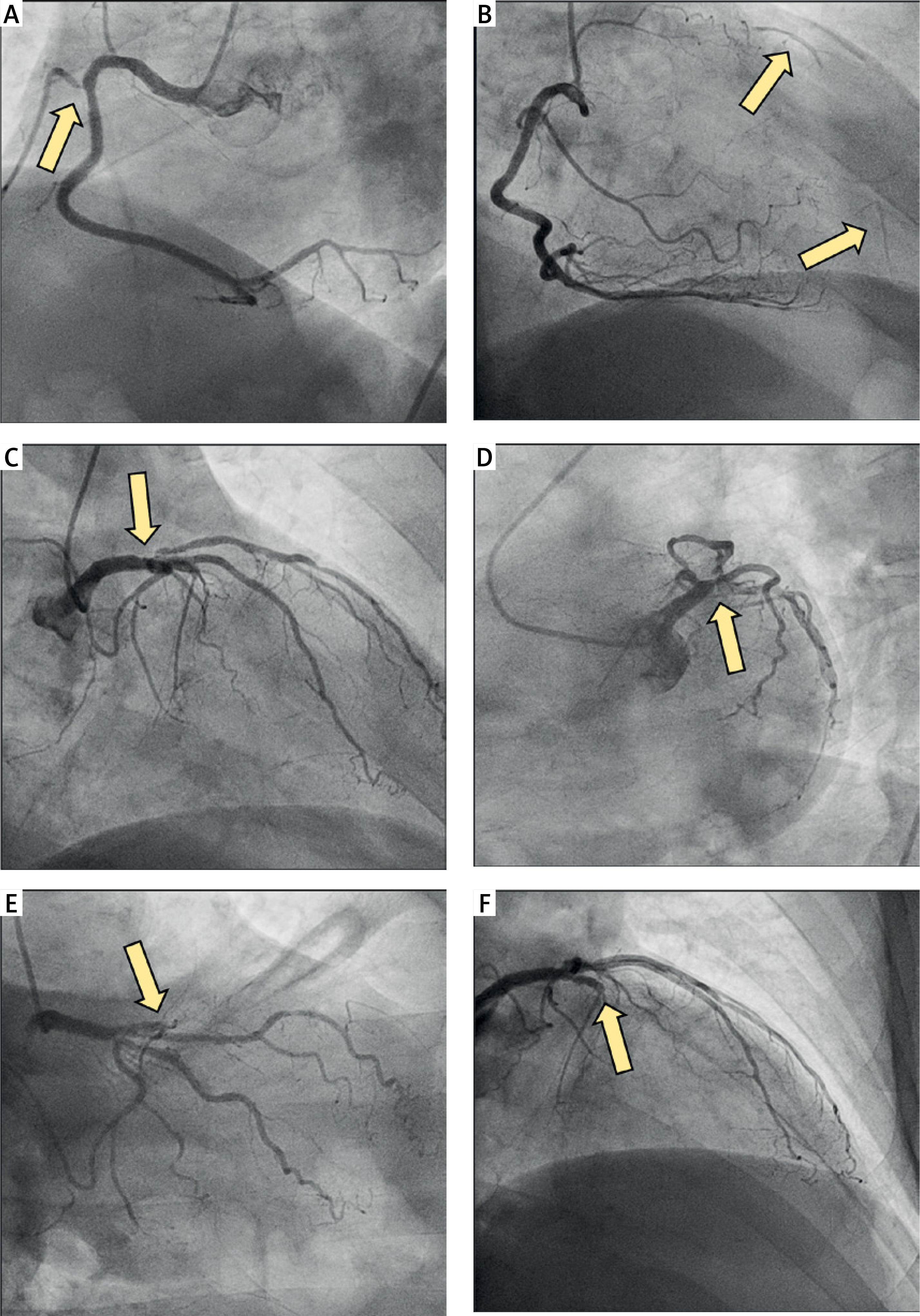
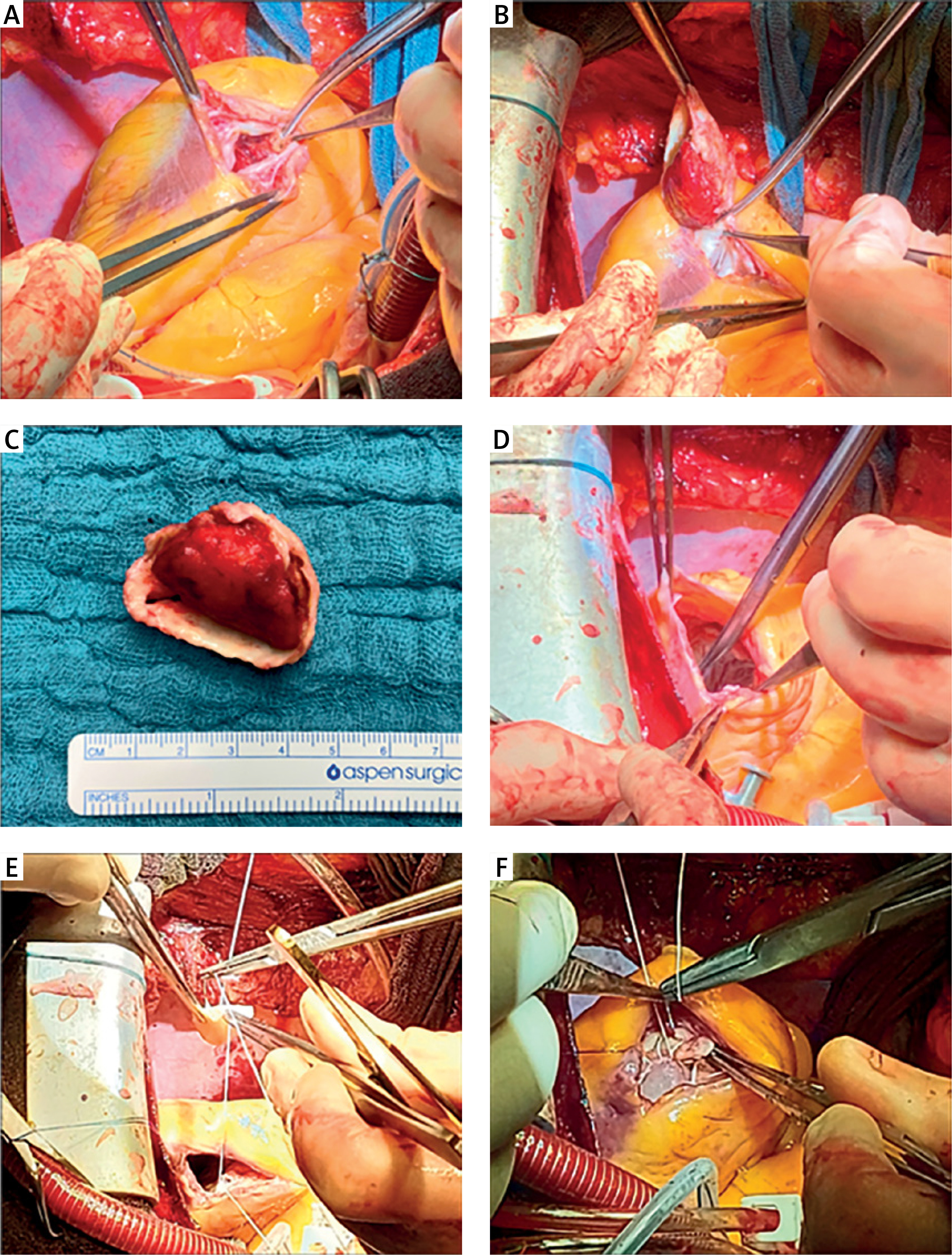
Figure 4
Intraoperative images illustrating the steps of complex left ventricular reconstruction surgery. A – Incision of the anterior left ventricle at the site of the aneurysm. B – Excision of the adherent thrombus from the aneurysmatic region of the left ventricle. C – The resected thrombus removed in its entirety. D – Identification of the margins of the ventricular aneurysm and transition to normal myocardium. E – Suturing of the pericardial patch to reconstruct the left ventricle, reinforcing the transitional zone between scarred and viable myocardium. F – Final placement of the pericardial patch between the aneurysmatic sac and the left ventricular cavity, ensuring optimal ventricular geometry and reducing wall tension. Teflon strips are used to reinforce the closure and prevent further ventricular dilation
Ventricular reconstruction surgery, particularly in the context of ischemic heart disease complicated by the left ventricular aneurysm and thrombus, remains an effective intervention to restore ventricular geometry, improve cardiac function, and prevent adverse outcomes such as thromboembolism and life-threatening arrhythmias [1, 2]. In this case, the successful application of the Dor procedure in a patient with coronary three-vessel disease, an apical aneurysm, and a severely reduced left ventricular ejection fraction (20%) highlights the safety and efficacy of this approach, even in complex clinical settings.
Indications for ventricular reconstruction surgery: Patients with post-myocardial infarction ventricular aneurysms often develop progressive systolic dysfunction due to paradoxical wall motion, impaired contractility, and increased left ventricular volume. Such pathological changes lead to deteriorating heart failure and poor prognosis if left untreated. Indications for ventricular reconstruction include [4, 5]:
Symptomatic heart failure (New York Heart Association Class III-IV) despite optimized medical therapy.
Presence of a true aneurysm with thin, non-contractile myocardium causing adverse ventricular remodeling.
Thrombus formation within the aneurysm, predisposing patients to embolic events.
Risk of ventricular arrhythmias secondary to scar tissue within the aneurysm.
For patients with severely reduced ejection fraction, as in this case, ventricular reconstruction combined with coronary artery bypass grafting (CABG) improves cardiac geometry, reduces wall stress, and enhances left ventricular performance, thereby alleviating heart failure symptoms and improving quality of life [6].
Evolution of ventricular reconstruction techniques: Over the decades, several surgical techniques have been proposed to manage ventricular aneurysms, including linear repair, endoventricular patch plasty, and more sophisticated geometric reconstructions. The earliest technique, linear repair, involved direct suturing of the aneurysm edges. While technically simple, this approach often resulted in suboptimal outcomes due to distortion of ventricular geometry and residual wall tension [7].
The introduction of endoventricular patch plasty by Dor in the 1980s revolutionized the approach to left ventricular aneurysms. The Dor procedure involves resection of the aneurysm, removal of the thrombus, and reconstruction of the ventricular cavity using a pericardial or synthetic patch to restore a more physiological, ellipsoid shape. This method preserves viable myocardium while eliminating the akinetic or dyskinetic segments, thereby improving global ventricular function. Unlike linear repair, the Dor procedure minimizes wall tension and ensures optimal volume reduction without compromising ventricular geometry [8]. Over the years, the Dor procedure has emerged as the preferred technique, largely because of its reproducible outcomes, safety, and superior physiological results. Studies have demonstrated significant improvements in ejection fraction, reduction in left ventricular end-systolic volume index, and enhanced patient survival [3, 9]. Moreover, its combination with CABG addresses the underlying ischemic etiology, ensuring comprehensive treatment.
Safety and benefits of the Dor procedure in complex settings: The safety of the Dor procedure in complex clinical scenarios, such as the presence of severe left ventricular dysfunction, large aneurysms, and intracavitary thrombus, has been consistently demonstrated [9]. In our patient, despite the severely reduced preoperative ejection fraction (20%), ventricular reconstruction, along with CABG and thrombectomy, led to an improvement in LVEF to 30% postoperatively. This incremental improvement, though modest, is clinically significant as it reduces symptoms of heart failure, limits further remodeling, and improves long-term survival. While the immediate postoperative improvement in LVEF from 20% to 30% is encouraging, further functional recovery is anticipated with optimized medical therapy and structured cardiac rehabilitation. Long-term follow-up studies suggest that patients undergoing ventricular reconstruction, particularly when combined with myocardial revascularization, may continue to experience gradual improvement in the left ventricular function over the subsequent months. Close echocardiographic monitoring is essential to evaluate functional gains and assess the need for adjunctive therapies.
Furthermore, addressing the intracavitary thrombus during the Dor procedure is critical to prevent embolic complications. The removal of the thrombus and reconstruction of the ventricle provide mechanical stability and reduce the risk of recurrence. Postoperatively, patients remain at risk for ventricular arrhythmias due to underlying myocardial scarring and persistent ventricular dysfunction. In such cases, close monitoring and consideration of prophylactic measures, such as wearable cardioverter-defibrillators (LifeVest), as utilized in this case, are essential. Electrophysiological assessment may play a role in risk stratification for arrhythmias in selected patients. The current guidelines recommend re-evaluation for ICD implantation after 40 days to determine if the persistent left ventricular dysfunction and arrhythmic risk warrant permanent device placement. The decision will be guided by repeat echocardiographic assessment and, if necessary, ambulatory ECG monitoring to detect non-sustained ventricular arrhythmias or other high-risk markers.
Long-term studies have demonstrated that the Dor procedure, when appropriately indicated, leads to significant improvements in left ventricular performance and patient survival. In addition to the early benefits seen in terms of ventricular remodeling and symptom relief, research suggests that patients may experience progressive functional gains beyond the immediate postoperative period. A recent study reported that in patients with severely reduced LVEF undergoing Dor reconstruction, the 5-year survival rate exceeded 75%, with a marked reduction in heart failure-related hospitalizations [10]. In a real-world ischemic heart failure population, surgical ventricular restoration demonstrated favorable outcomes, with no significant difference in survival between early and later operative cohorts, though patients with worse left ventricular remodeling and less extensive coronary artery disease exhibited a trend toward better outcomes [11]. These findings reinforce the long-term viability of the procedure as a cornerstone in the management of ischemic left ventricular aneurysms.
Challenges and considerations: Despite its benefits, the Dor procedure and ventricular reconstruction surgery in general pose technical and perioperative challenges. Proper patient selection is paramount as patients with diffuse myocardial scarring or significant residual viable myocardium are unlikely to derive substantial benefits [5, 8]. Preoperative imaging, including echocardiography, cardiac MRI, or CT, plays a pivotal role in assessing myocardial viability, aneurysm size, and thrombus burden [4]. Additionally, postoperative care remains critical, particularly in patients with multiple comorbidities, as seen in this case. Hemodynamic stability, careful management of heart failure medications, and structured rehabilitation programs are essential to optimize recovery. The decision to delay permanent ICD placement for 40 days, in line with current guidelines, reflects the importance of clinical reassessment following surgical revascularization and reconstruction. The Dor procedure has stood the test of time as the gold standard for left ventricular aneurysm repair due to its ability to restore ventricular geometry, reduce wall stress, and improve global function. In this case, its successful application alongside CABG and thrombectomy demonstrates its safety and efficacy even in patients with complex cardiac pathologies and a severely reduced ejection fraction. With proper patient selection, surgical expertise, and multidisciplinary postoperative care, ventricular reconstruction surgery continues to provide meaningful improvements in symptoms, cardiac function, and overall prognosis for patients with ischemic heart disease and ventricular aneurysms.