Introduction
The long-term viability and optimal biological and haemodynamic behaviour are the main issues in the selection of grafts. It is a complex process, crucial to the effectiveness of coronary artery bypass grafting (CABG) interventions, during which many factors must be taken into account: the extent of the disease (precise quantification, detection of stenoses), coexisting cardiological/cardiosurgical pathology (e.g. porcelain aorta), patient data (anthropometric-age-sex), comorbidities (chronic kidney disease (CKD)/diabetes mellitus (DM)/chronic obstructive pulmonary disease (COPD)/peripheral vascular disease/history of chest radiation), habits (profession-lifestyle),availability of grafts (clarity/reoperation of the heart), and technical data, to avoid mismach between the graft and the coronary artery [1].
The heart grafts are classified into 2 categories: arterial (internal mammary artery – IMA, radial artery – RA, right gastroepiploic artery – RGEA) and venous (saphenous vein graft – SVG). Other arterial (gastroepiploic artery, superior epigastric artery, inferior epigastric artery, splenic artery) and venous (lesser saphenous vein) grafts are used very rarely. Biological grafts, such as human umbilical vein graft (Biograft, Meadox-Medicals), processed bovine IMA (Biocor BIMA Biograft, Biocor-laboratory), synthetic grafts (PTFE/Dacron), and polyurethanes, have not yielded results due to high thrombogenicity [2].
The aim of the study was to present a current review of available choices of conduits in coronary artery bypass surgery.
Material and methods
We searched for all studies, including case reports, observational studies, and interventional trials, which reported available choices of conduits in coronary artery bypass surgery. We considered studies published from January 1990 until April 2023. We included studies published only in English language. A systematic search for related studies was carried out on PubMed and Cochrane Database, and the last search date was 30 November 2022. Search terms were “conduits” OR “coronary artery bypass surgery” OR “Coronary Artery Bypass Grafting” OR “CABG” OR “arterial grafts” OR “venous grafts”.
Results
A total of 196 studies were retrieved after applying this search strategy. 122 were excluded because they were not relevant to the scope of this review. From the remaining 74 studies, 20 were chosen as more representative of the full spectrum of the currently used techniques. The majority of studies were retrospective case series or case reports. These results can help cardiovascular surgeons in decision making regarding the most applicable technique in coronary artery bypass surgery.
Discussion
Internal mammary artery
The IMA originates from the proximal part of the subclavian artery, distributes parallel to the 2 ends of the sternum (Left-LIMA, Right-RIMA), and at the level of the 6th-7th intercostal space it divides into an upper epigastric and a myophrenic branch. As early as 1946, its usefulness as a graft was recognized (Vinberg intervention: intramyocardial implantation of LIMA). In 1986, its benefits were documented for the first time, compared to venous grafting [3]. Today, the use of LIMA for revascularization of the left anterior descending (LAD) artery is the gold-standard of cardiac surgery because it has been proven to improve survival and protect patients who have undergone CABG from major cardiovascular events.
Without doubt, the internal mammary artery exhibits better behaviour not only in relation to venous but also to other arterial grafts, which is due to its particular characteristics: It presents mainly large, elastic-type elements (such as aorta) and fewer medium-sized, muscular-type arteries (such as the coronary arteries). The endothelium is continuous, with low permeability. The internal elastic lamina is well developed and non-atherosclerotic. The media consists of elastic fibres and fewer smooth muscle cells, which are distributed circularly around the vessel axis. The outer coat has few vasa vasorum. Functionally, the endothelium produces large amounts of vasoconstrictors, mainly nitric oxide (NO), prostacyclin, and thromboxane [4].
The above provide excellent properties:
– The wall of the vessel is stable, so that it can withstand high blood pressures well but also adapt easily to pressure fluctuations, thus ensuring linear, and avoiding turbulent, flow. In combination with the fact that the flow in the IMA simulates the flow of the coronary arteries, the probability of thrombosis is minimized and the predisposition to atherosclerosis is limited. Cellular migration and entry of lipoproteins into the subendothelial space are obstructed, protecting against endothelial hyperplasia, neointima development, and atherosclerosis progression.
– The secretion of vasoactive factors, in combination with muscle fibre deficiency, protects against vascular rupture.
– Increased NO production and prostacyclin have a protective effect against atherosclerosis development, both in the grafted vessel and in the entire coronary network [5, 6].
– The graft is remodelled according to local haemodynamic conditions. Thus, changes are observed: change in the diameter of the IMA lumen depending on the degree of stenosis of the coronary artery, thickening of the endothelium up to 65% compared to the contralateral ungrafted LAD and reduction of the thickness of the media [7].
The method of skeletonization, during the preparation of the graft, offers further benefits: and increase in the diameter of the lumen, and increase in flow (due to peripheral sympatholysis), and significantly greater functional length, making more peripheral targets accessible. Also, sequential anastomoses and complex arterial grafts (T/Y grafts etc.) are facilitated [8].
Due to the avoidance of extensive sternal avascularity, healing is favoured and there is less risk of sternal wound infection (a condition of very poor prognosis), so the method is recommended for patients who are particularly susceptible to complications, such as diabetic patients, or patients with COPD, osteoporosis, or obesity. In addition, the use of in-situ IMA is a structural element in the implementation of CABG, a technique that is strongly recommended because, among other things, it is combined with a significant reduction in perioperative embolic events [9]. The patency of the IMA can reach 95% at 20 years for in-situ anastomosis of the LAD. Similarly, good results are observed in anastomosis of the IMA in other positions of the left system: 97% at 5 years and 91% at 15 years. Analogous are the results of RIMA, a biologically identical vessel of LIMA, in the left system. The lower patency in the anastomosis of the right system (80–90% at 10 years) can be attributed to the mismatch between graft and target coronary vessel, as well as to the faster progression of atherosclerosis at the bifurcation (crux) and at the distal part of the posterior descending artery (PDA). RIMA can also be used as a free graft in the Left system with similar good results [10].
Radial artery
The radial artery (RA) was initially used in 1971 by Carpentier but abandoned due to high tension for spasm and early occlusion [11]. For the downgrade of the graft, injury and hyperplasia of the endothelium were blamed, resulting from the mechanical stress of the vessel, due to the then technical preparation of the RA. The graft returned to the forefront in 1992 when the physiology of the vessel was understood and the mechanisms responsible for the first negative results were recognized. It is now exposed with a ‘no-touch’ technique and prepared/protected using pharmacological/vasoconstrictive factors, and today presents high long-term patency [12]. Histologically, it presents an expanded media muscularis layer, which explains its tendency to spasm. However, it seems that as a graft, the RA has the ability to be remodelled towards a more elastic phenotype, so that the traditionally long-term use of vasodilator factors is questioned [13, 14]. The vessel’s endothelium produces NO in smaller quantities, perhaps explaining its tendency for atherosclerosis development and its inferiority to IMA in long-term patency, which remains satisfactory: 90–98% medium-term, 89–91% in a decade, and 84.8% in a 20-year period [15]. However, there are limitations to the use of RA: The stenosis must be at least 70%, and for the right coronary system greater than 90%, to avoid competitive flow and/or early occlusion. Preoperative assessment of hand perfusion and adequacy of collateral ulnar-radial artery flow with the Allen test should be performed, and only if ulnar flow is adequate should we proceed to the collection of the graft. Haematoma and neurological complications are possible, which is why it is recommended to take from the non-dominant upper limb. It should be avoided in patients with CKD who may require dialysis/permanent fistula. The likelihood of vessel injury during previous angiography should be estimated, which will affect graft quality [13–15].
Right gastroepiploic artery
It is distributed along the major arch of the stomach, as the final branch of the gastroduodenal artery. It contains several smooth muscle fibres in the middle coat, so it is susceptible to spasm. It was initially used by Bailey in 1967 in the context of Vinberg’s intervention; however, it was established in clinical practice after 1987, following the announcement of very good results [16]. Since then, and given that the vessel has adequate flow when used in situ and there are no frequent contraindications (seriously atherosclerotic descending aorta, previous gastrectomy) in its collection, the graft has become quite popular. The most appropriate target is the peripheral of the right coronary artery, but vessels of the circumflex system are not excluded, with only the requirement for stenosis of the coronary > 90%. In contrast, phenomena of competitive flow/early occlusion are relatively frequent [17]. While the short-/medium-term patency of the graft exceeds 90%, initial results were lower than expected (62%). Modification of the method of collection, the graft dramatically improved long-term results (90.2% at 8 years), so today skeletonized preparation is proposed as a method of choice [18].
Great saphenous vein
Use of the great saphenous vein began in 1968 by René Favaloro. In October 1973, D. Cooley published an important article with the following central observation: the mortality of patients with 1-, 2-, or 3-vessel disease is, respectively, 4%, 6%, and 10% per year if treated with drug therapy. However, if they undergo CABG using GSV, the overall mortality is only 2.7%. This announcement played a fundamental role both in establishing CABG as well as in the widespread use of venous grafting [19]. Since then, venous grafting has been the most commonly used graft for 2 main reasons: a) it has sufficient length to cover the requirements of a large number of peripheral targets; and b) its preparation is easy, fast, and safe. However, the patency of the graft is lower: 81–97.9% in the first year, 75–86% in the medium term, and 50–60% after a decade, with a steady lowering rate of 1–2% per year for the first 6 years and then 4% per year in the next decade [6]. Three mechanisms are implicated in the downgrade of venous graft: Immediately postoperative (1st month): obstruction is attributed to thrombosis, a result of trauma and microruptures of the endothelium during graft collection, preparation, and suturing. Further endothelial damage occurs during exposure of the vein graft to high arterial pressures/pulsatile flow, and given that the venous wall is quite noncompliant, it favours the development of turbulent flow. Medium-term (1st month–1st year), thrombotic material organizes into fibrous tissue, migration/proliferation of smooth muscle cells is induced, and finally endothelial hyperplasia occurs. Long-term: all of the above lead to atherosclerosis, the responsible process for venous graft dysfunction. Atheromatous plaques tend to be diffuse, soft, minimally calcified, with necrotic areas and intense inflammatory elements, characteristics that predispose to rupture [20]. It should be emphasized that saphenous veins often present preexisting wall illness although it might not always be macroscopically obvious. These preexisting conditions may seriously affect the functionality and durability of the vein graft. Pre-existing endothelial hyperplasia is found in up to 95% of vein grafts after 60 years of age. All of these phenomena are interpreted by the morpho-functional properties of vein grafts, with main characteristics as follows: adequate presence of smooth muscle fibres (which are distributed circularly and parallel to the axis of the vein), high degree of differentiation/proliferation/cellular migration, limited NO production, and vulnerable to injury endothelium. For primary prevention of graft degeneration, various measures are taken, such as ‘no-touch’ preparation technique, avoidance of mechanical stress, careful anastomosis, intraoperative flow/outflow measurement, external graft-support of the graft, and finally pharmacological antiplatelet therapy [21].
Choices of grafts
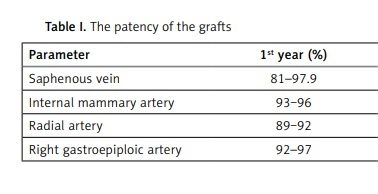
Survival after CABG depends directly on the patency of the grafts as it evolves over time (Table I) [22]. Arterial grafts have a long-term higher patency than venous ones, which is attributed to their biological and haemodynamic behaviour (they may present angiographically diffuse spasm and string-sign, a condition that resembles occlusion but is lifted when local haemodynamic or rheological conditions allow). Thus, the use of more than one arterial graft in multivessel CABG is associated with better results [4, 22, 23].
Table I
The patency of the grafts
| Parameter | 1st year (%) | 5th–7th year (%) | ≥ 10 years (%) |
|---|---|---|---|
| Saphenous vein | 81–97.9 | 75‒86 | 50‒60 |
| Internal mammary artery | 93‒96 | 88‒98 | 85‒95 |
| Radial artery | 89‒92 | 90‒98 | 89‒91 |
| Right gastroepiploic artery | 92–97 | 80–90 | 62 |
However, multiple arterial revascularization is internationally quite limited (< 7% in the USA, < 20% in the EU, < 10% in the UK and Australia, and about 25% in Japan), mainly because the preparation of arterial grafts is more demanding and time-consuming, arterial anastomoses are more difficult, and the risk of sternum injury exists [23]. The ART randomized study did not confirm a clinical advantage of arterial revascularization, and this is attributed to internal design weaknesses of the protocols, so its validity is now being checked. The ROMA study (Randomized Comparison of the Clinical Outcome of Single Versus Multiple Arterial Grafts) is expected to clarify the landscape; the first results will be announced in 2025. With the practice of implanting IMA in LAD not being disputed, the choice of the second arterial graft is made between RA and the contralateral IMA because both grafts have better patency than venous. Many randomized studies have indeed confirmed the greater long-term patency of RA compared to SVGs, which is also expressed clinically (when the second most important target is revascularized with RA and not with venous graft, there are fewer cardiac events in the decade) [4]. The choice between RA and RIMA is rather individualized and depends on the patient’s specific data and the surgeon’s familiarisation. From a practical point of view, RA is an excellent alternative to RIMA in patients at high risk for sternal trauma infection (DM, cortisone therapy, etc.) who are judged to benefit from multiple arterial reperfusion, and a positive Allen test precludes its use. Today, RA may have some theoretical advantage, because it seems to excel in the 10 years of free, but not in-situ, RIMA [24]. Finally, we should note that total arterial revascularization has been confirmed to be associated with longer survival, fewer major complications (stroke, MI), and can be considered the procedure of choice in patients with satisfactory survival expectancy [25].
Independently of the technique that is used, the systemic temperature must be maintained during the cardiopulmonary bypass above the temperature threshold activity of the cold-reactive proteins. Anaesthetic gases, intravenous liquids, and blood products should be warmed. The temperature in the surgery room should be raised and warm materials should be put on the surgical table.
The selection of conduits in coronary artery bypass surgery is a crucial aspect that significantly impacts patient outcomes. In this review article, we have explored the various arterial and venous graft options available for revascularization and discussed their respective applications in different clinical scenarios. The key learning points from this study include the prominence of arterial conduits, particularly the left internal mammary artery, which consistently demonstrates superior long-term patency rates and favourable outcomes. The use of the radial artery as an arterial conduit also proves to be a valuable alternative when the LIMA is unsuitable or when multiple grafts, especially in cases of total arteria revascularization in younger patients, are needed. However, the study highlights the importance of individualizing treatment plans based on patient-specific factors, such as age, comorbidities, graft number requirements, location and severity of coronary lesions, presence of prior bypass grafts, and left ventricular function. While venous conduits, such as the great saphenous vein, remain essential in certain situations, the concept of “arterializing” venous grafts emerges as a promising strategy to improve graft durability. Furthermore, hybrid conduit techniques, such as the application of T- or Y-grafts and bilateral internal mammary arteries (BIMA), offer innovative solutions for specific clinical cases. These insights can aid surgeons in making informed decisions, leading to improved patient outcomes and long-term success of coronary artery bypass surgery [26–30].
Limitations of the study: Despite the comprehensive nature of this review article, there are several limitations that should be acknowledged. First, the study’s reliance on existing literature may introduce publication bias because studies with positive or significant results are more likely to be published than those with negative findings. Additionally, the inclusion of studies published only in English could introduce language bias and potentially exclude valuable research published in other languages. Moreover, despite the systematic search on PubMed and Cochrane Database, it is possible that some relevant studies were missed because the search was limited to articles available only until 30 November 2022. Furthermore, the variability in study designs, patient populations, and surgical techniques among the included studies might have influenced the quality and generalizability of the findings. The review’s focus on published studies might also overlook valuable insights from ongoing research and unpublished data. Lastly, while case reports provide unique clinical observations, their limited sample size and lack of control groups may limit the strength of evidence for certain conduit choices. Despite these limitations, this review article aims to provide a comprehensive and informative overview of the available choices of conduits in coronary artery bypass surgery based on the existing literature up to the specified search date.
Conclusions
The choice of conduits in coronary artery bypass surgery should be based on a thorough understanding of each graft’s advantages and limitations, as well as consideration of patient-specific factors. Arterial conduits like the LIMA and radial artery are preferred when feasible, given their superior patency rates. However, venous conduits, particularly the saphenous vein, remain important alternatives when arterial grafts are unavailable or insufficient. The emergence of hybrid conduit techniques adds to the armamentarium of options available to surgeons, offering unique solutions to complex cases. The ultimate goal of conduit selection in CABG is to achieve optimal revascularization and long-term success, leading to improved patient outcomes and quality of life. Future research and advancements in surgical techniques may further refine the selection process, enhancing the efficacy of coronary artery bypass surgery.