Pre-hydration before percutaneous coronary interventions (PCI) to prevent acute kidney injury (AKI) has been a matter of debate. Initially, routine fluid administration was suggested to prevent post-PCI AKI. Later studied revealed that this is only true for patients with pre-existing renal insufficiency and has no beneficial effect in patients with normal renal function [1]. In contrast, dehydration increases the risk of 30-day and 1-year mortality [2]. Here, we underline the contribution of adequate preprocedural hydration to PCI success.
A 42-year-old man with a history of PCI with stent implantation to the left anterior descending (LAD) artery 5 years ago, arterial hypertension, and hypercholesterolaemia was admitted due to unstable angina. His renal function was normal. Echocardiography showed reduced left ventricle ejection fraction (32%) with regional wall motion abnormalities. Coronary angiography revealed calcified, critical stenosis in the mid segment of the right coronary artery (RCA, type B2 lesion), 80% stenosis in the proximal segment of the 1st marginal branch (MG1, type A lesion), and a patent stent in the LAD (Figures 1 A, B). Ad hoc PCI of the RCA lesion was performed. Following pre-dilation with a compliant balloon (MiniTrek 22.0 × 12 mm, 18 atm), 2 overlapping everolimus-eluting stents were implanted (Xience PRO 3.5 × 33 mm, 16 atm distally and 3.5 × 12 mm, 16 atm proximally), with a good result (Figure 1 C).
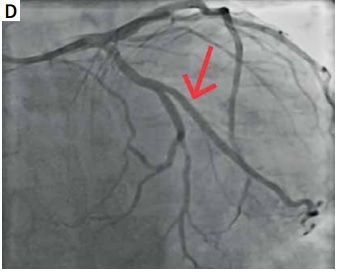
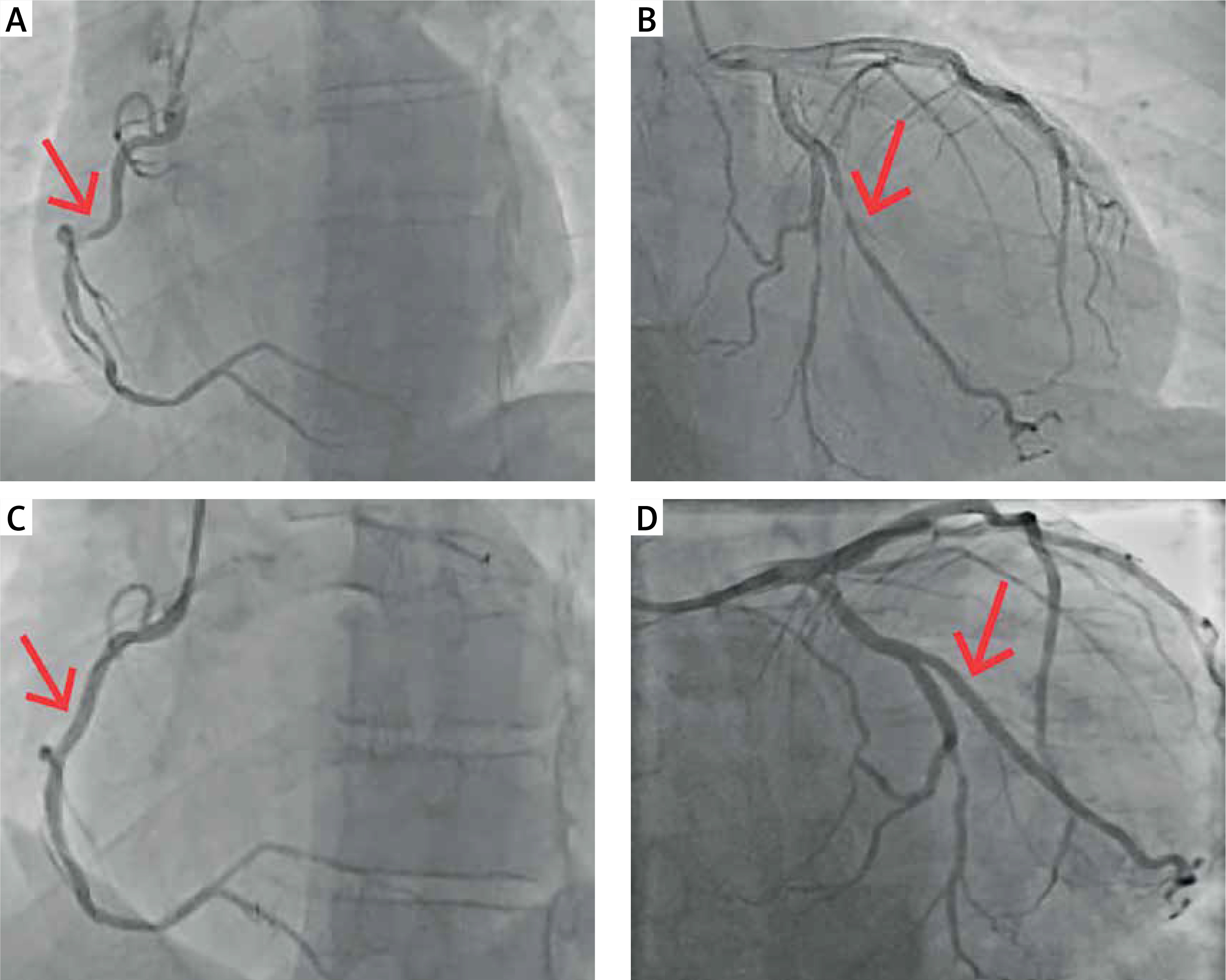
Figure 1
A, B – Coronary angiography showing calcified, critical stenosis in the mid segment of the right coronary artery (RCA; type B2 lesion), 80% stenosis in the proximal segment of the 1st marginal branch (MG1; type A lesion), and a patent stent in the LAD. C – Result of percutaneous coronary intervention of RCA with implantation of 2 overlapping everolimus-eluting stents (Xience PRO 3.5 × 33 mm, 16 atm distally and 3.5 × 12 mm, 16 atm proximally). D – Result of percutaneous coronary intervention of MG1 with implantation of everolimus-eluting stent (Xience PRO 2.5 × 23 mm; 10 atm)
Two days later, the PCI of MG1 was scheduled for the afternoon hours. The patient was fasting, but instructed to drink while awaiting the procedure, which he failed to do. The procedure was done via the right radial artery. Following insertion of the guidewire (Whisper MS) to the distal part of MG1 and pre-dilation of the lesion (Mini Trek 2.5 × 15 mm, 12 atm), the patient experienced a vasovagal syndrome, with dizziness and dyspnoea, accompanied by a drop in blood pressure (BP) to 45/30 mm Hg. Fluid resuscitation was immediately started, resulting in alleviation of symptoms and BP increase to 130/70 mm Hg. Because the patient became anxious and started moving, the guidewire dropped out from MG1 and it was troublesome to re-wire the vessel. Eventually, an everolimus-eluting stent (Xience PRO 2.5 × 23 mm, 10 atm) was implanted and post-dilated with a non-compliant balloon (2.5 × 18 mm, 20 atm) with a good effect (Figure 1 D). The patient was discharged from the hospital one day after the procedure on dual antiplatelet therapy (aspirin, ticagrelor) and standard-of-care heart failure pharmacotherapy.
Our case illustrates that pre-procedural dehydration is a risk factor for a troublesome PCI. Moreover, although fasting is often the standard care before PCI, there is no evidence supporting the benefits of fasting before low- or intermediate-risk procedures [3, 4]. Although the first emergency PCI was technically more challenging, it was better tolerated by the patient. The BP drop during the second, theoretically straightforward procedure led to patient anxiety and dropout of the guidewire, which prolonged the PCI and might have resulted in an adverse outcome. Although routine pre-procedural hydration is not recommended, especially in patients with advanced heart failure, care should be taken to avoid dehydration prior to PCI. Altogether, optimal, controlled, and careful hydration status might be the cornerstone of any percutaneous procedure, regardless of its complexity, left ventricle systolic function, and kidney function.