Heart disease is the leading cause of death in the United States, followed by cancer. Due to advances in treatment options for both conditions, the chances of cancer patients having heart disease are trending upwards. A retrospective cohort study using an administrative health care database showed that the cardiovascular risk was greatest for patients with genitourinary, gastrointestinal, thoracic, nervous system, and haematological malignancies [1]. Another large real-world analysis showed that cancer patients with acute myocardial infarction (AMI) tend to be older, with multi-vessel disease, and carry a high burden of arrhythmia and medical comorbidities [2]. Due to the above factors, evaluating and understanding the clinical outcomes of cancer patients with cardiovascular disease becomes important.
Renal cell carcinoma (RCC) represents 2–3% of all adult malignancies, which is projected to increase [3]. Recent studies have shown that non-RCC-related causes of death, specifically cardiovascular disease, are increasingly prevalent in RCC patients [4]. However, there is a paucity of literature on the outcomes of such patients following admissions for AMI.
The objectives of this study are to evaluate the complications, and rates of percutaneous intervention (PCI), coronary artery bypass grafting (CABG), and mortality in RCC patients admitted for AMI.
The National Inpatient Sample (NIS) from 2016 to 2020, a component of the Healthcare Cost and Utilization Project (HCUP), was utilized. The database consists of deidentified patient records of hospitalizations, patient characteristics, diagnoses, and procedures performed during hospitalization [5]. Adults aged 18 years and over with a primary diagnosis of AMI as per the International Classification of Diseases, Tenth Revision (ICD-10) codes were recruited. Among them, patients with RCC were identified using the ICD-10 codes, and 2 cohorts were created: patients with RCC and those without RCC [6, 7]. Patients with other cancers were excluded. Baseline comorbidities were compared between the 2 groups [8]. Propensity score matching (PSM), adjusting for multiple patient and hospital characteristics (as seen in Table I), was performed to compare the outcomes of the patients admitted with AMI with and without RCC. PSM reduces the effects of confounding factors by matching the 2 groups of patients with a similar distribution of confounders so that the difference in their outcomes is unbiased. To comply with HCUP guidelines, all values < 11 were masked and not reported.
Table I
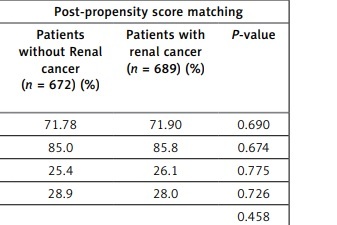
Characteristics of patients with and without renal cell cancer admitted for acute myocardial infarction; a pre-propensity and post-propensity matching analysis
| Parameter | Pre-propensity score matching | Post-propensity score matching | ||||
|---|---|---|---|---|---|---|
| Patients without Renal cancer (n = 3,039,479) (%) | Patients with renal cancer (n = 3445) (%) | P-value | Patients without Renal cancer (n = 672) (%) | Patients with renal cancer (n = 689) (%) | P-value | |
| Mean age [years] | 66.59 | 71.90 | < 001 | 71.78 | 71.90 | 0.690 |
| Age ≥ 60 years | 69.8 | 85.8 | < 0.01 | 85.0 | 85.8 | 0.674 |
| Weekend admission | 26.4 | 26.1 | 0.671 | 25.4 | 26.1 | 0.775 |
| Females | 37.4 | 28.0 | < 0.01 | 28.9 | 28.0 | 0.726 |
| Insurance form: | < 0.01 | 0.458 | ||||
| Medicare | 56.1 | 71.4 | 74.7 | 71.4 | ||
| Medicaid | 9.7 | 4.8 | 3.7 | 4.8 | ||
| Private | 26.1 | 19.2 | 18.3 | 19.2 | ||
| Race: | < 0.01 | 0.022 | ||||
| White | 73.3 | 74.0 | 82.0 | 74.0 | ||
| Black | 11.4 | 10.4 | 7.1 | 10.4 | ||
| Hispanic | 8.9 | 10.4 | 7.1 | 10.4 | ||
| Urban teaching hospitals | 70.1 | 73.7 | < 0.01 | 77.7 | 73.7 | 0.203 |
| Cirrhosis | 0.8 | 1.2 | < 0.01 | * | * | 0.062 |
| Diabetes | 40.9 | 45.4 | < 0.01 | 43.5 | 45.4 | 0.463 |
| Hypertension | 43.3 | 26.7 | < 0.01 | 33.9 | 26.7 | < 0.01 |
| Peripheral vascular disease | 7.8 | 8.9 | 0.019 | 8.2 | 8.9 | 0.659 |
| Smoking | 49.4 | 46.9 | < 0.01 | 45.1 | 46.9 | 0.508 |
| Obesity | 20.7 | 15.7 | < 0.01 | 12.5 | 15.7 | 0.093 |
| Chronic kidney disease | 23.6 | 50.9 | < 0.01 | 43.9 | 50.9 | < 0.01 |
| Prior MI | 16.0 | 20.0 | < 0.01 | 15.0 | 20.0 | 0.015 |
| Prior stroke | 8.0 | 9.1 | 0.011 | 6.8 | 9.1 | 0.118 |
| Prior CABG | 9.9 | 10.4 | 0.261 | 9.2 | 10.4 | 0.449 |
| Prior PCI | 17.1 | 17.4 | 0.654 | 15.0 | 17.4 | 0.233 |
| Alcohol abuse | 3.4 | 1.9 | < 0.01 | * | * | 0.568 |
| Depression | 9.0 | 8.3 | 0.156 | 6.5 | 8.3 | 0.225 |
| Drug abuse | 2.9 | 1.5 | < 0.01 | * | * | 0.955 |
| Lipid disorder | 67.9 | 61.5 | < 0.01 | 63.7 | 61.5 | 0.412 |
| Family history of CAD | 14.7 | 8.3 | < 0.01 | 8.3 | 8.3 | 0.968 |
| Anaemia | 22.0 | 42.8 | < 0.01 | 36.6 | 42.8 | 0.019 |
| COPD | 17.3 | 22.2 | < 0.01 | 16.5 | 22.2 | < 0.01 |
| Mean CCI score | 3.12 | 6.31 | < 0.01 | 3.64 | 6.31 | < 0.01 |
A total of 3,042,924 patients with the diagnosis of AMI met the inclusion criteria, of whom 3445 (0.11%) had concomitant RCC. Patients with RCC were older than those without RCC (mean age of 71.90 vs. 66.59 years, p < 0.010), with more patients aged ≥ 60 years (85.8% vs. 69.8%, p < 0.01). Both cohorts were primarily insured via Medicare (71.4% in RCC group and 56.1% in non-RCC group) and mainly consisted of patients racially classified as white (74.0% in RCC group and 73.3% in non-RCC group).
Regarding baseline comorbidities, RCC patients had a higher prevalence of cirrhosis (1.2% vs. 0.8%), diabetes (45.4% vs 40.9%), peripheral vascular disease (8.9% vs. 7.8%), chronic kidney disease (50.9% vs. 23.6%), prior history of myocardial infarction (20% vs. 16%), prior stroke (9.1% vs. 8%), anaemia (42.8% vs. 22%) , and COPD (22.2% vs. 17.3%) and a higher mean Charlson Comorbidity Index (CCI) score (mean score of 6.31 vs. 3.12). However, RCC patients had a lower prevalence of smoking (46.9% vs. 49.4%), obesity (15.7% vs. 20.7%), alcohol use disorder (1.9% vs. 3.4%), and drug use (1.5% vs. 2.9%) than those without RCC (Table I).
To evaluate the primary outcomes, propensity score matching was done. Before propensity score matching, higher rates of complications in patients with RCC, including acute kidney injury (AKI) (34.4% vs. 19.7%, p < 0.01), cardiogenic shock (7.4% vs. 6.4%, p = 0.016), and pulmonary embolism (PE) (2.3% vs. 0.5%, p < 0.01) were seen. Fewer RCC patients underwent PCI (32.2% vs. 49.3%, p < 0.01) and CABG (6.5% vs. 9.0%, p < 0.01). The rate of cardiopulmonary resuscitation (CPR) was lower (2.9% vs. 3.6%, p = 0.038) and mortality was higher in patients with RCC (7.3% vs. 4.5%, p < 0.01).
After propensity score matching, patients with RCC had higher odds of developing acute pulmonary embolism during their hospitalization (aOR = 5.006, 95% CI: 1.5–16.4, p = 0.008) and lower odds of undergoing PCI (aOR = 0.755, 95% CI: 0.58–0.97, p = 0.028). No statistical significance was seen in the prevalence of AKI, cardiogenic shock, ischaemic stroke, and rates of CABG, CPR, and mortality. While patients with RCC experienced a longer hospitalization (mean length of stay 5.62 days vs. 4.98 days, p < 0.01), no statistically significant differences were noted in the mean hospital charges ($107678.47 in RCC cases vs. $97495.55 in the non-RCC group, p = 0.068).
Various factors could be hypothesized regarding the higher risk and poorer outcomes of AMI in RCC. Increasingly, there is a trend towards an earlier and incidental diagnosis of RCC due to the widespread use of imaging. Due to this and enhanced treatment modalities, RCC patients are living longer, with 5-year survival for locoregional disease ranging from 72% to 93% [9]. The hypercoagulable state of cancer and treatment modalities like immunotherapies, tyrosine kinase inhibitors, and antibodies could all contribute to an increased risk of cardiovascular disease.
To the best of our knowledge, our retrospective study is currently the largest and most up-to-date analysis focusing on the characteristics and outcomes of AMI patients with RCC. While a higher mortality rate was initially observed in the AMI patients with RCC, it was not statistically significant after PSM, which was consistent with previous studies in this area [10]. Furthermore, while it is known that there is an increased risk of PE in patients with RCC [11], our study highlights the higher odds of pulmonary embolism during AMI admissions in RCC patients.
Although a higher comorbidity score could explain the lower PCI rates in RCC patients, the authors believe that there could be a component of underutilization of interventional procedures in cancer patients due to concerns about prognosis. This is consistent with a previous analysis by Mohamed et al., who found that despite PCI reducing all-cause mortality and major adverse cardiovascular events (MACE) in both cancer and non-cancer patients, cancer patients were less likely to receive PCI compared to the non-cancer group [12].
The results of our study bring forward some important points for clinicians when treating RCC patients with AMI. A high index of suspicion for atherosclerotic disease, strong focus on prophylactic anticoagulation, early diagnosis of complications like PE, and non-biased decision-making for procedural interventions might help improve prognosis in these patients. Promoting multidisciplinary care, specifically with oncology, cardiology, and palliative care, can help direct the right modality of treatment.
Our results, based on real-world cohorts, are best evaluated along with the limitations of the database. Firstly, the National Inpatient Sample (NIS) database does not differentiate whether RCC patients received surgery, chemotherapy, or both. We are also limited in our assessment of chronology to determine at what time during hospitalization a patient with RCC develops AMI. In addition, NIS relies on the accurate coding of diagnoses and procedures, which can affect the sensitivity of such an analysis. Finally, our analysis includes only hospitalized cases, and the patients with AMI who were managed in the emergency department and died before in-patient care could not be included.
In conclusion, the findings of this study suggest that patients with renal cell carcinoma admitted with acute myocardial infarction are older and have multiple comorbidities. They are at a higher risk for the development of pulmonary embolism during hospitalization. Patients with RCC and AMI are less likely to undergo percutaneous coronary intervention as compared to patients without RCC. Through our study, we wish to highlight these characteristics and the outcomes of RCC patients with AMI, thus advocating for a more individualized treatment approach catered to this high-risk patient population.