Introduction
Cardiovascular disease (CVD) is a class of diseases that involve the heart or blood vessels, and its prevalence continues to increase each year [1], remaining one of the most serious threats to human life and health and the first or second leading cause of death in most countries of the world [2, 3]. CVD includes both coronary artery diseases (CAD) such as myocardial infarction, as well as cardiovascular and cerebrovascular diseases such as rheumatic heart disease, cardiomyopathy, and myocarditis, ischemic heart disease, stroke, and hypertensive heart disease [4].
The majority of cardiovascular diseases develop at an after age for women compared to men, while men are about 3–4 times more likely than women to suffer from ST-eleva- tion myocardial infarction (STEMI) or non-STEMI. These gender differences between men and women are due to differences in gene expression from the sex chromosomes and differences in sex hormones [5]. Cardiovascular diseases occur mainly in middle and older adulthood. However, the onset of certain cardiovascular diseases has tended to occur at younger ages in recent years. For example, the prevalence of specific heart diseases such as rheumatic heart disease peaks between the ages of 20 and 29 years [6]. Furthermore, puberty is an important period for both physical and mental development of children, which is usually neglected for universal health coverage [7, 8]. It has been proved that young people with cardiovascular diseases represent a significant share of the mortality burden [9]. For example, atherosclerosis can appear early in life and remain undetected for a long time before progressing to an advanced, clinically apparent phase [10–12], while rheumatic heart disease causes approximately 250 000 deaths every year in developing countries [13].
The International Childhood Cardiovascular Cohort (i3C) study ascertained that metabolic risk factors such as high body mass index, high systolic blood pressure, and high cholesterol and the increased change in these risk factors from childhood to adulthood can predict fatal or nonfatal cardiovascular disease [14]. Therefore, an updated understanding of the global burden of CVD among young people is crucial to inform policymakers for the implementation of primary prevention and control.
The Global Burden of Disease (GBD) study offers a unique approach in the broader context of global health to track rapidly evolving patterns in the epidemiology of cardiovascular disease so that they can be studied comprehensively with the ultimate goal of future prevention. An analysis of 2012 WHO global health assessment data showed that cardiovascular disease has become the most important and largest cause of death from non-communicable diseases worldwide (more than 50%) over the past two decades and is set to remain the largest significant global health burden for the coming decades [15]. The 2015 GBD study ascertained that CVD remained the leading cause of premature death and chronic disability for all countries of the world, with ischemic heart disease (IHD) and stroke accounting for the majority of health losses due to CVD.
Therefore, based on data from GBD 2019, this paper identifies epidemiological trends in total and type-specific CVD prevalence from 204 countries/territories globally from 2010 to 2019, stratified by age and gender, and statistically significant differences between genders and age groups have also been identified.
Material and methods
The Global Burden of Disease study 2019 provides data on the prevalence, incidence, mortality and disability-adjusted life years (DALY) of 369 injuries and diseases for 204 countries and territories from 1990 to 2019 by age, sex and country [16]. This study focused on CVDs with an age range of 25–49 years, 50–69 years, 70–89 years, 90–-94 years and 95+ years. Data on the prevalence relating to overall and type-specific CVDs were extracted from the GBD 2019 dataset [17], that is, rheumatic heart disease, ischemic heart disease, stroke, hypertensive heart disease, non-rheumatic valvular heart disease, cardiomyopathy and myocarditis, atrial fibrillation and flutter, aortic aneurysm, and endocarditis. The statistical methods used in this work are the independent samples t-test and one-way analysis of variance (ANOVA) test to examine the existence of statistical significance between genders and between age groups in 2010 and 2019 in the prevalence of cardiovascular diseases.
Results
Table I shows the average global prevalence rate of cardiovascular diseases by gender in the period 2010–2019 as well as whether there is a statistically significant difference in these rates between the two genders, using the χ2 test. As can be seen, there is a statistically significant difference between the rates in the two genders in all cardiovascular diseases except atrial fibrillation and flutter. Females have the highest prevalence rates of CVDs worldwide. More specifically, the average global prevalence rate of cardiovascular diseases in females is 0.068%, while in males it is 0.062%. Moreover, females have statistically significantly higher prevalence rates of stroke, hypertensive heart disease, rheumatic heart disease, non-rheumatic valvular heart disease, endocarditis, peripheral artery disease and other cardiovascular and circulatory diseases globally. On the other hand, males have statistically significantly higher prevalence rates of cardiomyopathy and myocarditis, and ischemic heart disease than females. Figures 1 and 2 show the global prevalence rate of CVDs by gender during 2010-2019.
Figure 1
Global prevalence rate of stroke (A), cardiomyopathy and myocarditis (B), ischemic heart disease (C), hypertensive heart disease (D), and atrial fibrillation and flutter (E) by gender during 2010–2019
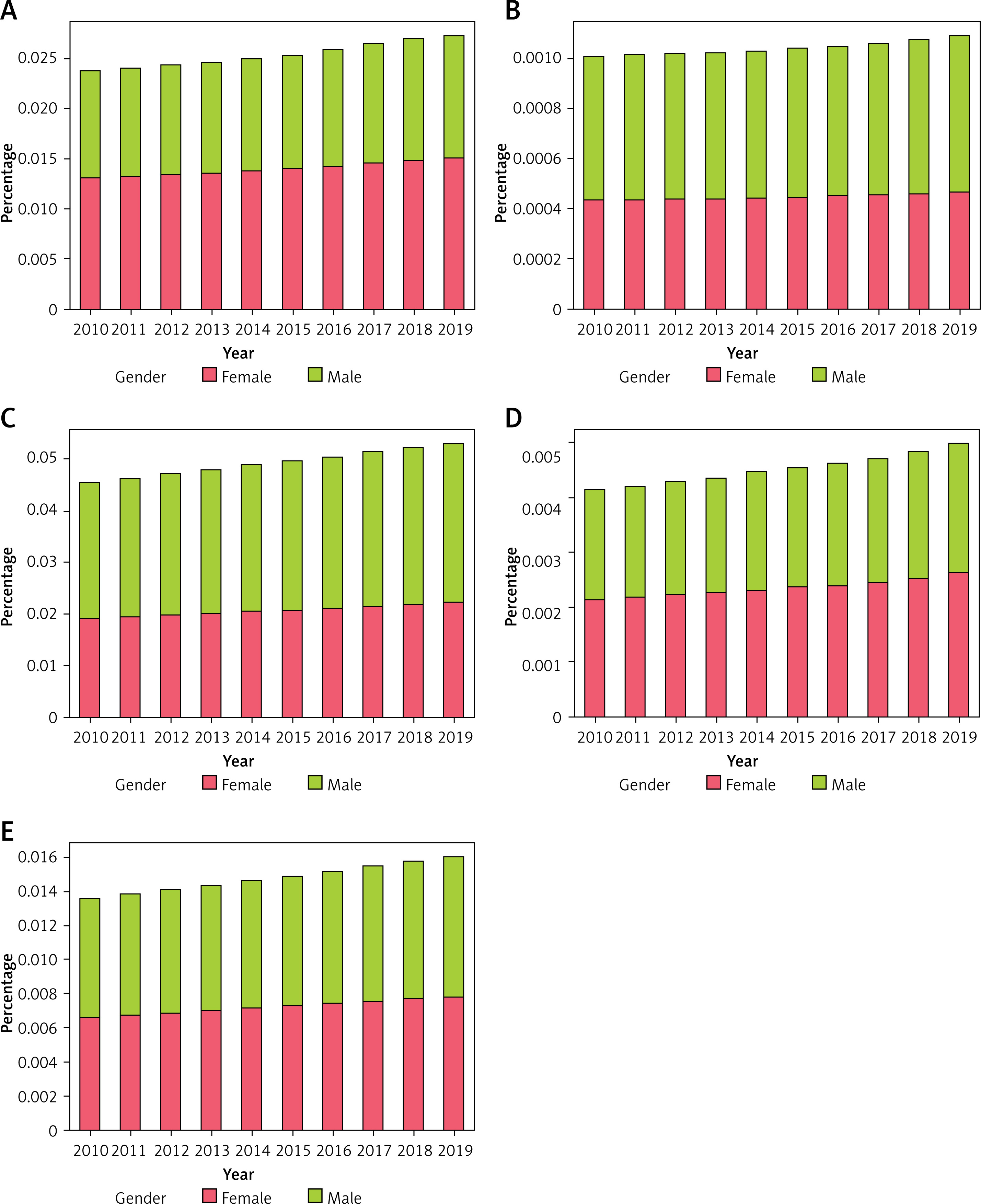
Figure 2
Global prevalence rate of rheumatic heart disease (A), non-rheumatic valvular heart disease (B), endocarditis (C), peripheral artery disease (D) and other cardiovascular and circulatory diseases (E) by gender during 2010–2019
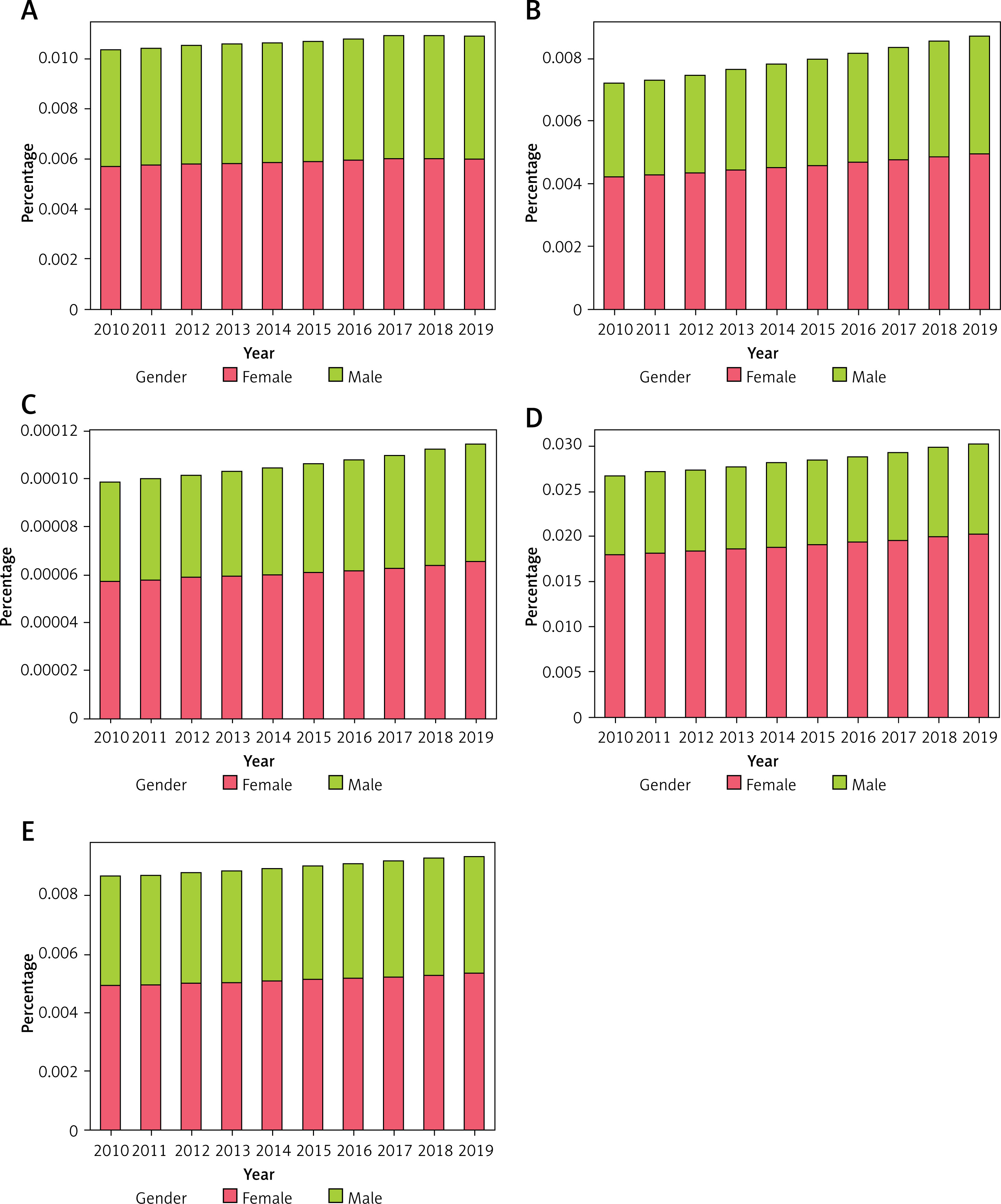
Table I
Global prevalence rate of CVDs by gender during 2010–2019 (independent samples t-test)
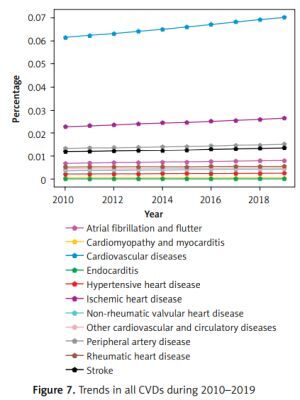
Table II shows the average global prevalence rate of cardiovascular diseases by age group in the period 2010–2019 as well as whether there is a statistically significant difference in these rates between the age groups of 25–49 years, 50–69 years, 70–89 years, 90–94 years and 95+ years, using the one-way analysis of variance (ANOVA) test. As can be seen, rheumatic heart disease has a statistically significantly higher rate in the age group of 25–49 years than the other age groups. Additionally, ischemic heart disease, and atrial fibrillation and flutter, have statistically significantly higher rates in the age group of 90–94 years than the other age groups. Stroke, cardiomyopathy and myocarditis, hypertensive heart disease, endocarditis, non-rheumatic valvular heart disease, peripheral artery disease and all cardiovascular diseases have statistically significantly higher rates in the age group of 95+ than the other age groups. Finally, other cardiovascular and circulatory diseases have statistically significantly higher rates in the age group of 70-89 than the other age groups. Figures 3 and 4 show these differences in each age group during 2010–2019. Figure 5 shows the global prevalence rate of CVDs by gender and age group during 2010–2019. Figure 6 shows the global prevalence rate of CVDs by cause for both genders and all ages. Finally Figure 7 shows the trends in all CVDs during 2010-2019. From Figure 7 it can be seen that all CVDs tended to increase from 2010 to 2019.
Figure 3
Global prevalence rate of stroke (A), cardiomyopathy and myocarditis (B), ischemic heart disease (C), hypertensive heart disease (D), and atrial fibrillation and flutter (E) by age during 2010–2019
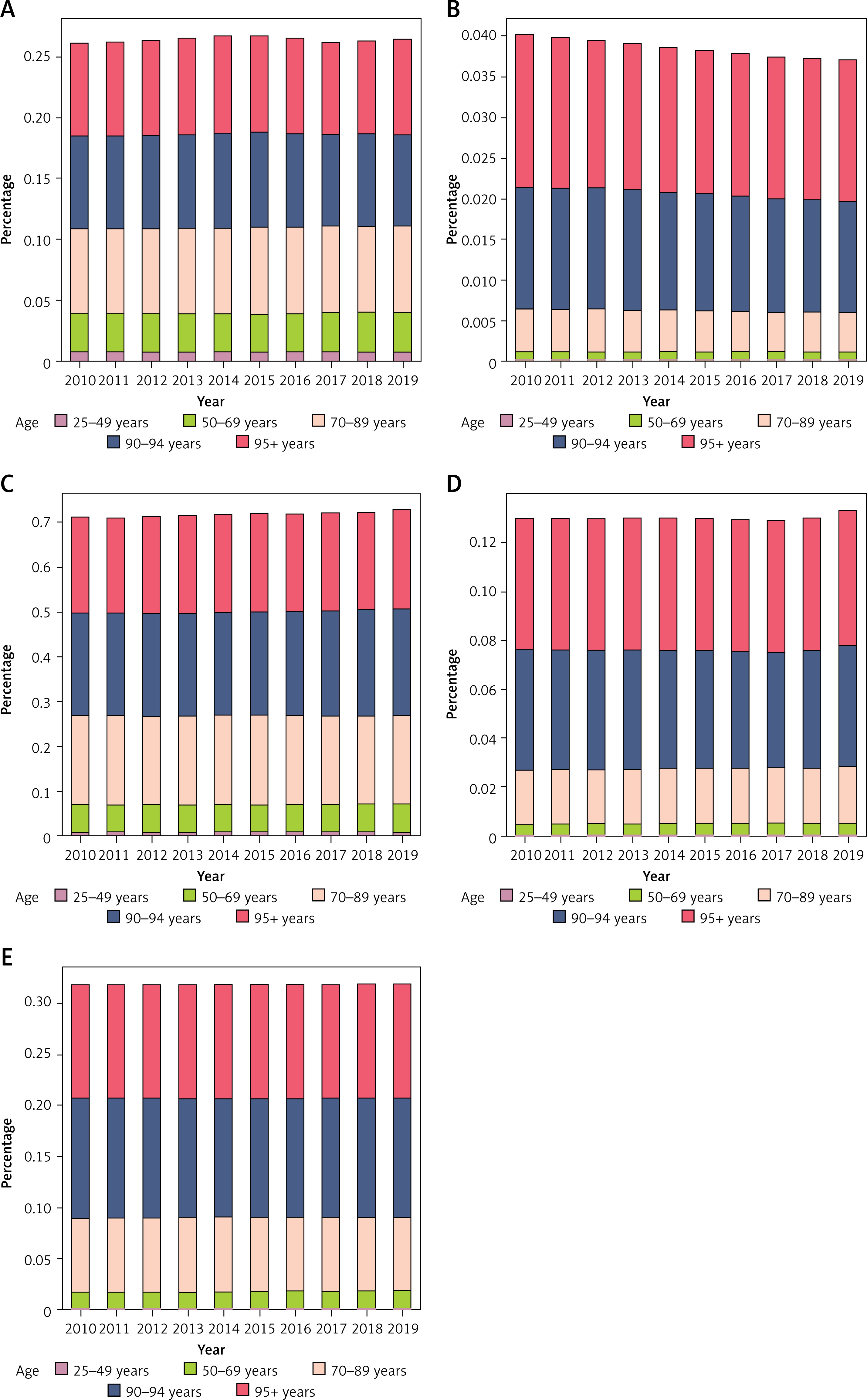
Figure 4
Global prevalence rate of rheumatic heart disease (A), non-rheumatic valvular heart disease (B), endocarditis (C), peripheral artery disease (D) and other cardiovascular and circulatory diseases (E) by age during 2010–2019
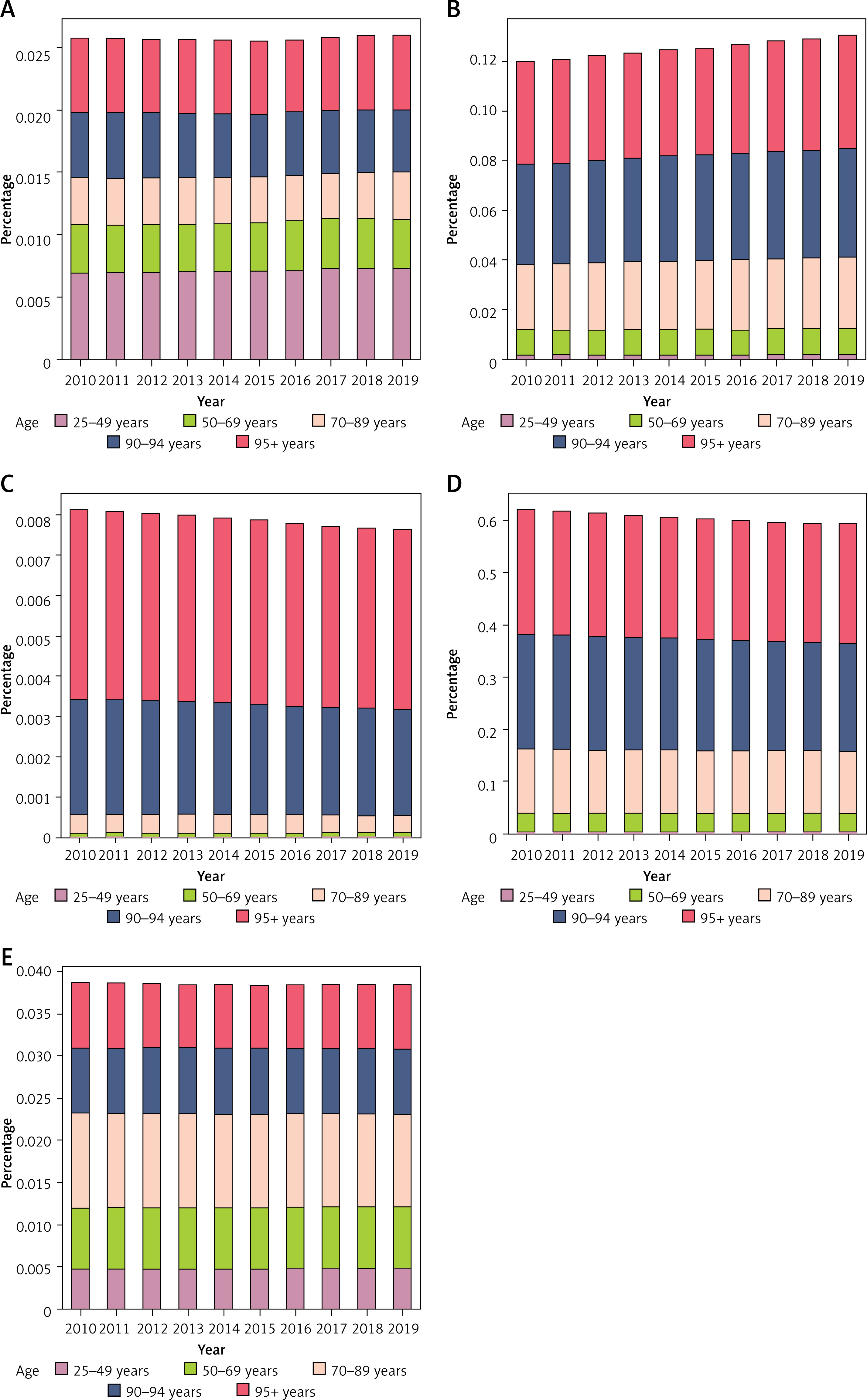
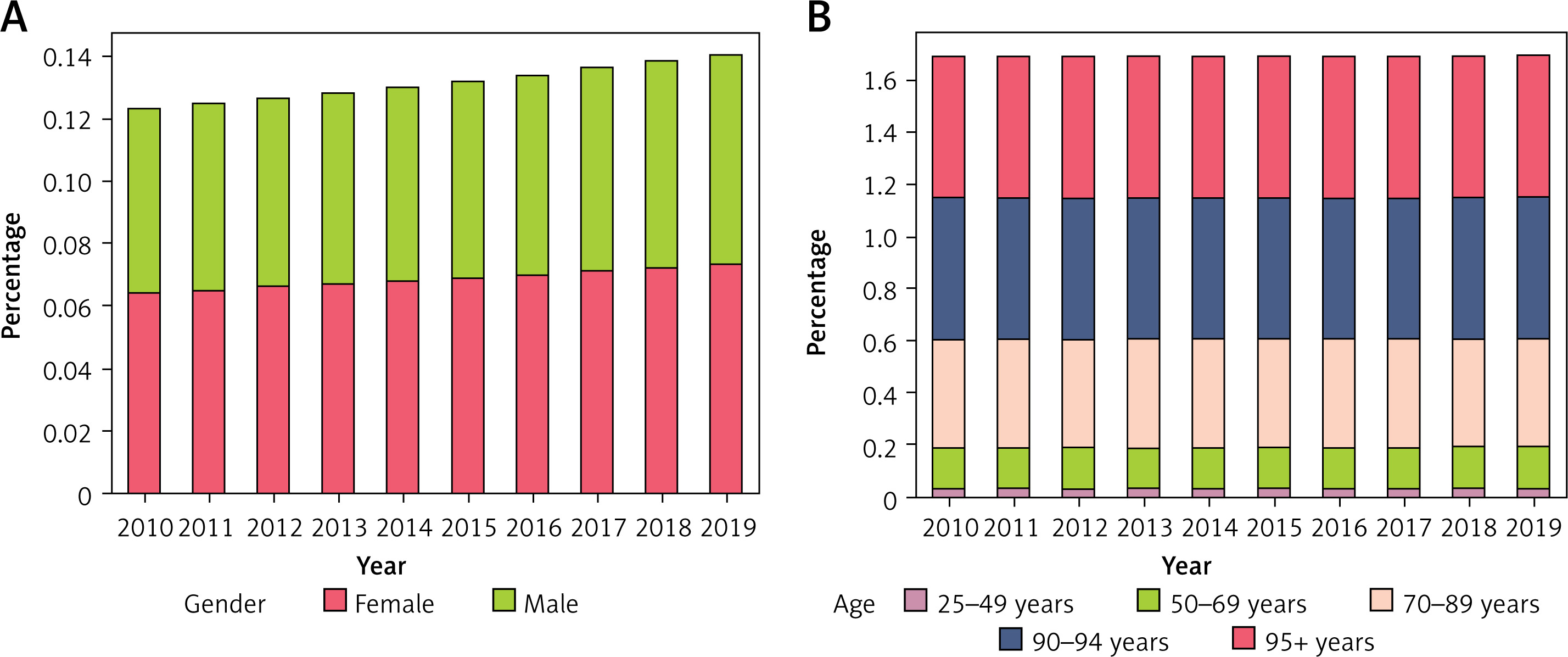
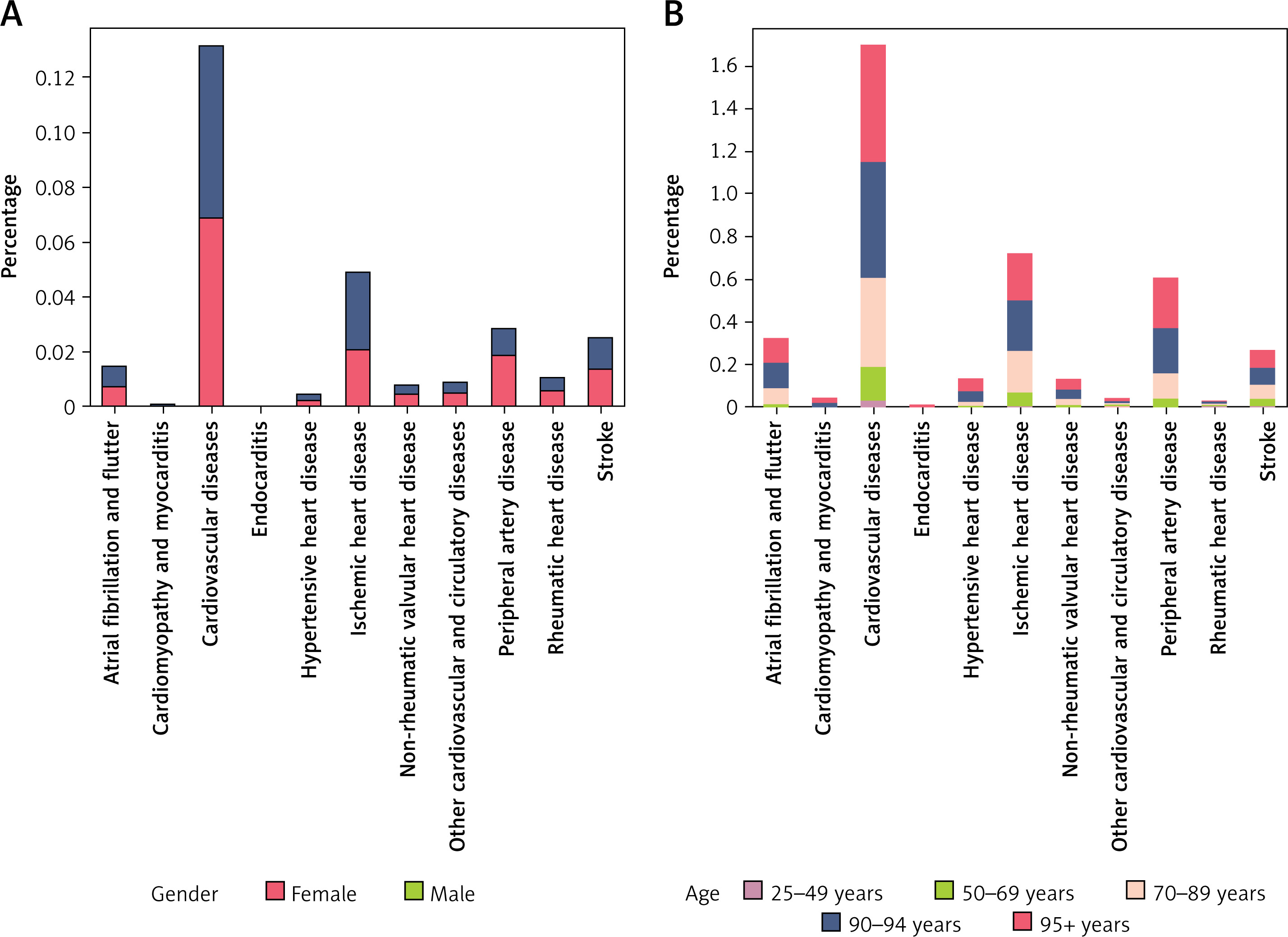
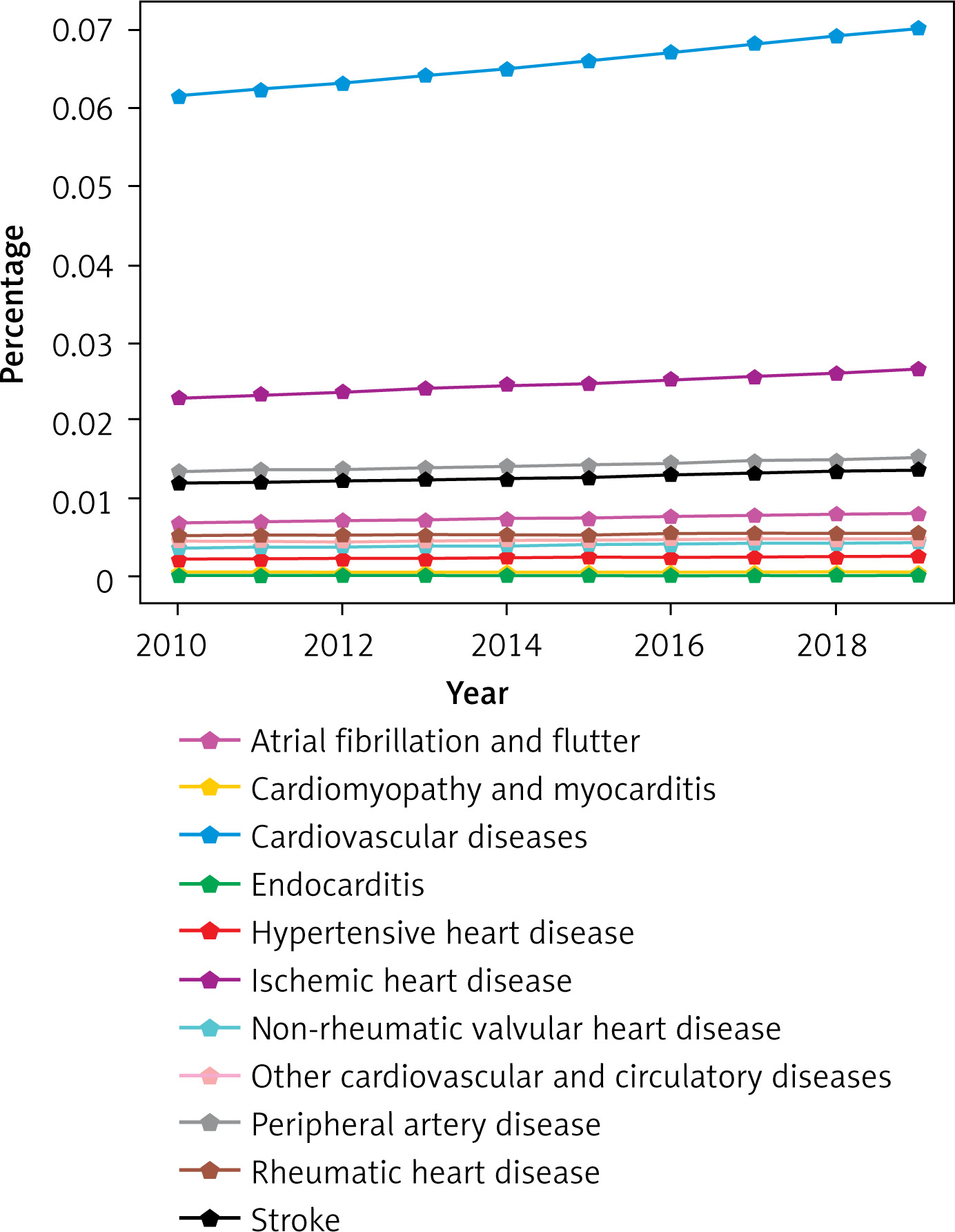
Table II
. Global prevalence of CVDs by age group during 2010–2019 (one-way ANOVA test)
Discussion
The main goal of this study was not only to study the global trend in the prevalence of CVDs but also to study whether there is a statistically significant difference between genders and ages during 2010–2019. Many researchers have tried to solve the same problem [18–21]. This study differs from the aforementioned studies and from the 2019 Global Burden of Disease Lancet Report [22] in that it is a study of cardiovascular disease prevalence that focuses on the last decade for which we have data to study and is also the only study to find statistically significant differences between the two genders and between age groups.
Comparing the results of this study with previous ones, it is noteworthy that a large number of studies have reported the high global burden of total or type of CVD in the general population [6, 23–27]. In contrast to the decreasing trend in overall CVD among middle-aged and older adults worldwide [24, 28], this study found an increasing trend in the prevalence rates of all CVD between 2010 and 2019. In addition, similar to a previous study [6], several type-specific CVDs such as rheumatic heart disease have become prevalent in young people (25–49 years). Regarding gender differences, similar to a previous study [18], females were found to have a higher prevalence rate of CVDs than men. In contrast to the ischemic heart disease being more pronounced in women [18] during 1990–2019, the present study found a higher global prevalence rate in men than in women in the decade 2010-2019. In contrast to the atrial fibrillation and flutter being more pronounced in women [18] during 1990–2019, the present study did not find a statistically significant difference between the genders during 2010–2019. Finally, similar to a previous study [18], females were found to have a higher prevalence rate of endocarditis than men.
The findings of this study suggest that targeted strategies and measures for the prevention and management of CVD in youth and young adults are urgently needed. Several public health approaches, such as school-based health promotion programs, increases in health care services by implementing interprofessional teamwork, implementing digital clinical decision-making tools, and creating accessible and affordable rehabilitation facilities, especially for youth and young adults, are useful for dealing with the challenges of cardiovascular diseases.
In conclusion, the prevalence of overall and specific cardiovascular diseases varies by age and sex. Cardiovascular diseases are largely preventable, which makes them deserve more attention in the targeted implementation of effective primary prevention strategies. The significance of this study is not only that it has succeeded in achieving to evaluate the global, gender, and age-related cardiovascular disease (CVD) burden, finding statistically significant associations, but it is also the only study to achieve this goal in the last decade.