Introduction
Pericardial diseases carry significant morbidity and mortality and their presentation can range from asymptomatic and transient to severe and recurrent forms which may be life-threatening [1]. Bibliometric analysis is a well-established quantitative method for assessing research performance that evaluates the pattern and frequency of occurrence of citations in literature [2–4]. Although it is difficult to evaluate the true value of an article, citation analysis allows us to identify landmark studies in a particular field, demonstrate knowledge gaps, and identify studies that may have had a disproportionate influence on a particular field [3, 4]. Bibliometric studies in medicine have helped identify focus areas and understand biases in scholarly output [5]. Considering the significant disease burden, prolonged course, as well as evolving treatment options, it is likely that the research interest in the field of pericardial diseases will continue to evolve. In an attempt to better understand the research output in pericardial disease in terms of focus areas, role of funding, female representation, and to guide future course, we conducted a bibliometric analysis of the top 100 cited manuscripts on pericardial diseases.
Material and methods
Search strategy
We searched Web of Science from inception (January 1900) to April 20, 2020, using the following search terms: “pericarditis”, “pericardial”, “pericardium”, “pericardial effusion”, and “tamponade”. Under Web of Science Core Collection, the following data sources were selected that were pertinent to our study: Science Citation Index Expanded (SCI-EXPANDED), Conference Proceedings Citation Index-Science (CPCI-S), and Emerging Sources Citation Index (ESCI). From the search results, a list of journals under the Web of Science subject categories “Cardiac Cardiovascular System”, “Medicine General Internal”, “Oncology”, “Surgery”, “Immunology”, “Radiology Nuclear Medical Imaging”, and “Pathology” was compiled. This was done to avoid missing out on articles on pericardial disease that were published in journals other than those that focused on cardiovascular diseases only. These journals were then searched to compile a database of manuscripts pertaining to pericardial diseases. Only English language studies in humans and the field of medicine were included. We excluded studies that were done on animals. All manuscripts from journals focusing on fields of science other than medicine were also excluded. We did not limit our search based on abstract availability, country of origin, or study type. All journals included in our list were searched using print and electronic International Standard Serial Numbers. For manuscripts where electronic copies were unavailable, hard copies were sought from an inter-library loan service to ensure that full texts of included articles were reviewed.
After an extensive search, the results were sorted in descending order of citations received. This method of citation analysis has been shown to be a reliable measure of assessing the impact of an article [4]. The title and abstracts were screened by 2 reviewers (V.J. and H.N.E.) independently to ensure that the manuscripts adhered to the aforementioned inclusion criteria. A list of the top 100 cited manuscripts was subsequently compiled. In case of discrepancy, a consensus was achieved with the help of a third independent reviewer (A.K.). This was a retrospective review of already published literature and institution review board approval was not required.
Study variables
Data were extracted regarding citation count, authors, institutional affiliation, country, year, journal of publication and theme. The bibliometric tags used for analysis from the Web of Science search are presented in Supplementary Table SI.
The manuscripts were ranked in order of total citations received since publication. The most relevant authors were defined by the number of manuscripts contributed by them in the top 100 list. While ranking authors on relevance, the order of authorship in the manuscript was not given weightage. For example, authors with the same number of manuscripts as the first or second author had the same relevance. We calculated a collaboration index for multi-authored (≥ 2) manuscripts. It is given as total authors/total multi-authored manuscripts [6]. The collaboration index helps understand the mean number of authors per multi-authored manuscript, with a higher collaboration index implying more collaboration among authors. The reprint author was designated as the corresponding author. This method has previously been validated in other bibliometric analysis [7]. If multiple authors were designated as corresponding authors, we considered all of them as corresponding authors. Information on the gender of the first and the corresponding author was extracted using the author’s photograph on institutional portfolios. The relevance of institutions and countries was derived according to the number of manuscripts. If there were multiple authors on a manuscript with different institutional affiliations or countries, the document was assigned to > 1 institution or country. Thus, there could be more than 100 institutional affiliations. In cases where authors changed their affiliation over time, we selected the country and institute with which the authors were affiliated at the time of publication of the respective manuscript.
We used Keywords Plus to identify keywords that are automatically generated from a manuscript’s bibliography and are unique to the Web of Science [8]. Keywords Plus may include words not included in author keywords and help evaluate an article’s content in greater depth. These were analyzed using a co-occurrence network to identify recurrent associations. The abstracts of the manuscripts were reviewed to identify themes.
Local citations are the manuscripts that are included in the bibliography of ≥ 1 manuscript in the reference set, i.e. manuscripts that were cited by the top 100 most cited manuscripts. We used reference publication year spectroscopy to create a temporal profile of these locally cited references in the top 100 cited manuscripts to understand the impact of landmark publications [9]. Landmark publications have been evaluated previously to assess the impact of key publications over time that were cited multiple times by the most impactful papers in a field. We considered the top 10% most locally cited publications as landmark publications [10].
Software for bibliometric analyses
The bibliometrix package of R statistical software was used for bibliometric analysis [11]. Briefly, bibliometrix is an open-source R package used for comprehensive science mapping using a logical bibliometric flow. It uses metadata from Web of Science references as bibliographic attributes and facilitates data analysis and data visualization.
We used the χ2 test to evaluate an association between the gender of the first and the corresponding author. The statistical analyses were conducted in Stata version 14.2 (StataCorp, College Station, TX, U.S.A.). All p-values were 2-sided, with < 0.05 considered statistically significant.
Results
Citations and type of manuscript
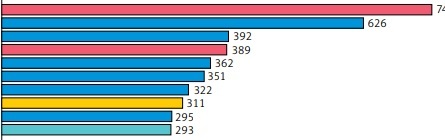
Among the top 100 cited manuscripts in the Web of Science, there were 43 case series, 25 review papers, 14 cohort studies, 7 randomized trials, 5 cross-sectional studies, 4 case-control studies, and 2 meta-analyses. Of the review articles, 3 were society guidelines. These manuscripts were published between 1965 to 2015 in 29 sources and 26% of manuscripts were published between 2000 and 2009 (Supplementary Figure S1 A). The ten manuscripts with the highest number of citations are given in Figure 1. Among these ten manuscripts, there were 6 original articles, 1 case series, and 3 reviews. Of the 3 review articles, 2 were society guidelines. A complete list of the top 100 manuscripts is given in Table I. These manuscripts were cited 189 times on average (range: 110–743); only two manuscripts were cited > 500 times.
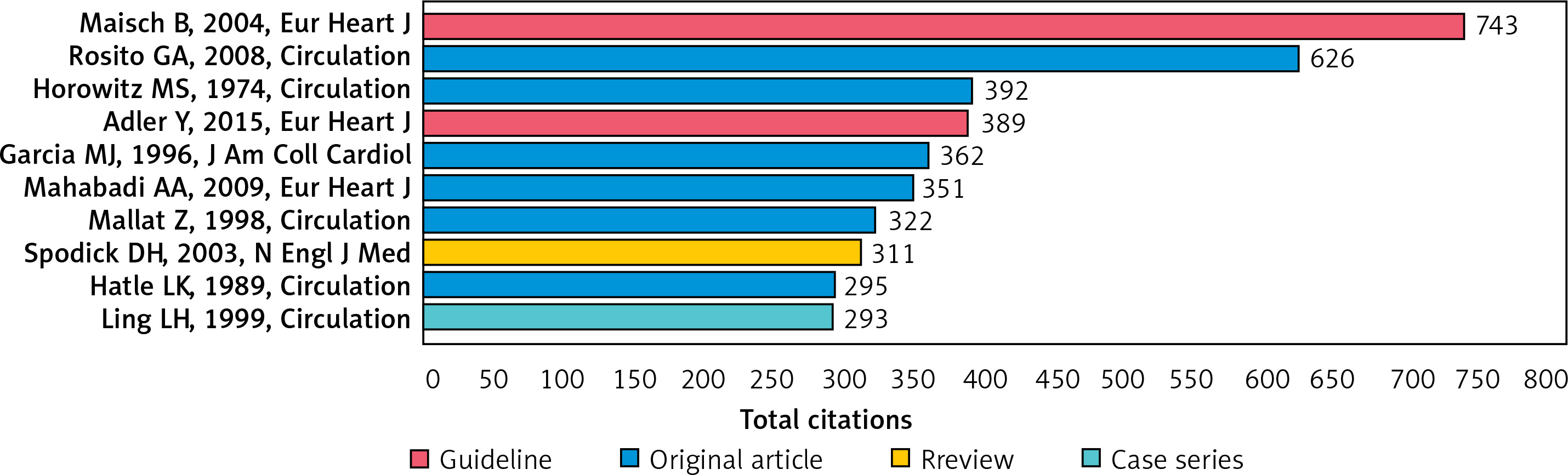
Table I
Top 100 cited documents in decreasing order of citations received
Authors
The top 100 manuscripts were published by 478 authors and 9 manuscripts were written by a single author. Each document was written by five authors on average with a collaboration index of 5.3. Around 90% of authors had written just one document. The most relevant authors are given in Table II and Supplementary Figure S1 B. Women were the first author in ten manuscripts and the corresponding author in seven manuscripts. There was a significant association between the gender of the first and the corresponding author, such that there were higher odds of having a woman as a first author if the corresponding author was also a woman (odds ratio = 44, p < 0.001).
Table II
Most relevant authors in the top 100 manuscripts
Author affiliation, country and funding information
Harvard University and Mayo Clinic Foundation in the United States and Maria Victoria Hospital in Italy had the highest number of manuscripts in the top 100 (Supplementary Figure S1 C). Most manuscripts were from institutions in the United States (n = 40), Italy (n = 10), and Spain (n = 5). There were only a few manuscripts that had co-authors from multiple countries (Supplementary Figure S2). Funding information was publicly available for 20 manuscripts; thirteen were funded by US organizations – nine by the National Institutes of Health. There was no association between funding and the gender of the first or corresponding author.
Journal
Circulation (n = 26), American Journal of Cardiology (n = 11), and Journal of American College of Cardiology (n = 9) had the highest impact and together published ~50% of these manuscripts (S3 ????? Supplementary Figure S1 D).
Co-occurrence network of Keywords Plus
When two Keywords Plus appear together in a document, there are said to co-occur. The word is given in the rectangle; the size and the color of the rectangle depict the frequency and network of occurrence, respectively. Out of the four, one network (red) had the unique words “epicardial adipose tissue”, “obesity” and “inflammation”, suggesting an increase in research interest in this field.
Content of the manuscript
Among the top 10 manuscripts, both guidelines provided a comprehensive review of etiology, classification, diagnosis, and management of pericardial diseases. Both guidelines were published by the European Society of Cardiology. Among the six original manuscripts, two studies evaluated the diagnostic accuracy of echocardiography to differentiate restrictive cardiomyopathy vs. constrictive pericarditis. Another two studies assessed the adverse prognostic role of pericardial fat on cardiovascular outcomes in primary prevention. There were 29 and 31 studies on clinical features, diagnosis, or management of pericardial effusion or tamponade and pericarditis, respectively (Supplementary Figure S3). There were eight and six manuscripts on pericardial fat and neoplasms, respectively.
Discussion
In our analysis of the top 100 cited manuscripts on pericardial diseases, we found that most of the top-cited manuscripts were published in the period 2000–2009. This parallels the evolution of research in other fields of cardiology and is associated with advances in medical imaging and diagnostic techniques [5, 12]. Landmark manuscripts, such as by Dressler et al., were progressively cited less over time, suggesting a trend that certain facts and findings may become so fundamental in clinical practice that researchers no longer feel the need to cite the source article [13]. This phenomenon is called obliteration by incorporation, and it often contributes to recent time peaks in the bibliometric analysis [14].
Among the top 10 cited manuscripts, there were 2 guidelines on the management of pericardial diseases. The highest research output was from the United States and Europe, and in fact, both guidelines were published by the European Society of Cardiology. This suggests an unmet need for guidelines by professional cardiology institutions such as the American College of Cardiology and the American Heart Association, unlike their European counterparts. In recent years, cardiovascular conditions such as valvular heart disease and heart failure have received more attention from professional cardiology societies with updated guidelines every few years [15, 16]. This is because of the high burden, rapid evolution in therapeutics, and high-quality data from randomized control trials in these fields. Currently, there is limited information on the morbidity and mortality associated with pericardial diseases. Initiation of or including data on pericardial diseases in ongoing registries such as the Atherosclerosis Risk in Communities study will help understand the actual burden and knowledge gaps for future research.
Pericardial diseases, such as pericarditis and effusion, were the most common themes explored in these manuscripts. For conservative management of pericarditis, a few therapeutic options such as colchicine or immunosuppression are available [17–19]. In our study, we found six randomized trials and all of them studied colchicine as a treatment modality for pericardial diseases. This indicates a possible unmet need for data exploring other treatment options. However, it is worth mentioning upcoming clinical trials on rilonacept, an IL-1 blocker, which is being investigated as a new therapeutic modality and offers new hope for the future.
Most manuscripts were published in one of the three major cardiology journals in the United States: Circulation, the Journal of the American College of Cardiology, and the American Journal of Cardiology. These findings demonstrate the application of Bradford’s law, a bibliometric concept that indicates that researchers obtain a majority of their citations from a few leading journals, and whenever they deviate from these selected journals, the frequency of citations and impact decrease [20].
We found that there was an underrepresentation of women as first or corresponding authors, with a significant association between the gender of the first and the corresponding author, indicating that having women as first authors was less likely if the corresponding author was male. This imbalance pattern in scholarly output is similar to the trend seen in other fields in cardiology [21]. There were ten authors with ≥ 5 citations in the top 100 list, which is significantly higher than those seen in other bibliometrics. This may suggest that a few authors are publishing the bulk of the literature on pericardial diseases. We also found that an overwhelming proportion (n = 50) of the top-cited work was published by two countries – the United States and Italy – but only a few manuscripts had authors from ≥ 1 country. A better international collaboration, such as in heart failure, will help advance knowledge to generate high-quality data for diagnosis and management of pericardial diseases.
Our review of available data suggested that only 20% of manuscripts on pericardial diseases were funded. This is in sharp contrast to other fields of research in cardiology such as heart failure, where a similar study suggested that 86% of top-cited manuscripts were funded [22]. Most manuscripts on pericardial diseases were funded by government institutions such as the national institution of health. Lack of data on morbidity and mortality and limited options for management may be limiting industry sponsorship and progress in research in pericardial diseases. It would be interesting to see if this trend changes in the upcoming years with pharmaceutical companies funding trials such as those for IL-1 blockers as potential therapeutic targets.
In our analysis, we found a growing interest in the study of pericardial fat. Pericardial fat has been found to have an association with the burden of coronary artery disease and is hypothesized to drive local inflammation [23]. Improvement in medical imaging has advanced our understanding of how local fat deposits might be associated with diverse cardiac pathologies such as atherosclerosis and atrial fibrillation [23, 24]. With a shift in focus from infectious to metabolic diseases, research on the role of pericardial fat in the pathophysiology of cardiovascular diseases is likely to increase.
To the best of our knowledge, this is the first study to comprehensively review the current status of research in pericardial diseases. There are limitations to our analysis. The Web of Science database is updated weekly but the total citations may differ from other databases such as Google Scholar or PubMed [25]. Scopus has a wider range of sources and may yield more manuscripts with the same search words, but does not go as far back as Web of Science. The selection of top-cited manuscripts may exclude recently published landmark research. For example, a document published in 2020 with 10 citations is likely to be more relevant than a document published in 1970 with 200 citations (averaging 4 citations per year). The search strategy used may have missed other sources of pericardial research such as book chapters and online documents that were not cited in the literature.
In conclusion, in this bibliometric analysis of the top 100 cited manuscripts in pericardial diseases, we provide an insight on the characteristics and quality of the highly cited literature in the field of pericardial diseases. This can be used to guide further research in the field of pericardial diseases.