
Acute arterial occlusion (AAO) is a vascular emergency, which is characterized by a sudden interrupted perfusion of the limbs [1] and deep vein thrombosis (DVT) is a common complication of long-term hospitalizations and a preventable cause of in-hospital deaths [2, 3]. Although arterial and venous thrombosis are known as different clinical presentations due to risk factors, pathophysiology and treatment methods, two of these conditions have been shown to be associated [4]. The rupture of the atherosclerotic plaques leads to AAO known as platelet-rich white thrombus and decrease in blood flow usually may cause venous thrombosis [4]. AAO is associated with increased mortality and disability should be recognized rapidly since it will lead to loss of the limb [1]. It is important to distinguish venous and arterial thrombus for early diagnosis and treatment, and it is an uncommon condition to see both at the same patient [5]. Doppler ultrasound (DUS) is a valuable method to diagnose acute arterial thromboembolism and DVT, but when it cannot be applied, computed tomography angiography (CTA) may alternatively be preferred by physicians [6, 7].
Here, we reported a rare coexistence of acute thrombotic occlusion of the left popliteal-tibioperoneal artery and left iliofemoral vein admitted to emergency department (ED), which was successfully treated with surgical arterial thrombectomy and iliofemoral vein pharmacomechanical thrombectomy (PMT) with thrombolysis under local anaesthesia.
A 67-year-old man with medical history of hypertension, severe chronic obstructive pulmonary disease (COPD), current smoker and recent abdominal aortic aneurysm (AAA) surgery admitted to ED with complaints of pain, cyanotic colour changes, coldness and swelling of the left lower extremity which started approximately one day before (Figure 1). It was learned that the patient had an AAA surgery approximately 50 days ago, he was hospitalized for about 1 month after surgery and his activity became limited after he was discharged from the hospital. However, it was learned that the patient did not use his medications regularly in the post-discharge period. Coldness was detected and pulses were non-palpable in distal arteries of the left lower limb without any sensory loss or motor deficit. Vital and laboratory signs were as follows: blood pressure 100/50 mm Hg, pulse 83 per/min, respiratory rate 23 per/min, oxygen saturation 86% (chronicity was confirmed by the relative of the patient), haemoglobin 8.7 g/l, creatinine 1.4 mg/dl, white blood cell 13.5 × 109/l and platelets, prothrombin time and partial thromboplastin time were in normal range. Arrhythmia was not detected on his electrocardiography (ECG) and pathological finding was not observed on chest X-ray. Transthoracic echocardiography performed by an experienced cardiologist was normal and no septal defect was detected. Acute thrombosis of the left external iliac vein and distal arterial occlusion of the left limb was detected in the patient by DUS at the first admission. Thrombosis of the left external iliac and femoral vein and ipsilateral popliteal arterial occlusion were determined on CTA (Figure 2) performed for detailed examination. Hydration, low molecular weight heparin (LMWH) was started and the patient was successfully treated with surgical thrombectomy with 3–4 Fr Fogarty catheters. Fogarty catheters from the left femoral artery was performed under local anaesthesia to remove the clot in the left popliteal-tibioperoneal artery with a small skin incision. After the revascularization, the coldness of the foot was decreased, but swelling did not change significantly. Approximately, 10 h after the procedure, a temporary inferior vena cava (IVC) filter (Inca, Invamed, Turkey) was placed through the right common femoral vein to prevent possible pulmonary thromboembolism associated with the treatment of acute left iliofemoral venous thrombosis by PMT with the catheter directed thrombolysis (CDT) procedure (Mantis, Invamed, Turkey). Ultrasound-guided PMT with CDT treatment was performed in the prone position under local anaesthesia through the left popliteal vein. His complaints were started to regress approximately 24 h after this procedure (Figure 3). The temporary IVC filter was withdrawn 12 h after the procedure. No complication such as bleeding occurred after the procedure. The patient’s dorsalis pedis pulse was detected with palpation and hand-held Doppler USG and the patient was given medical treatment in the hospital for 2 days. LMWH and acetylsalicylic acid were given for 2 weeks and the patient was recommended to use anticoagulant treatment. Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Figure 1
The patient had severe pain, swelling, cyanosis and oedema of the left lower limb with purplish discoloration

Figure 2
Thrombosis of the left external iliac vein and ipsilateral popliteal artery were determined on CT angiography
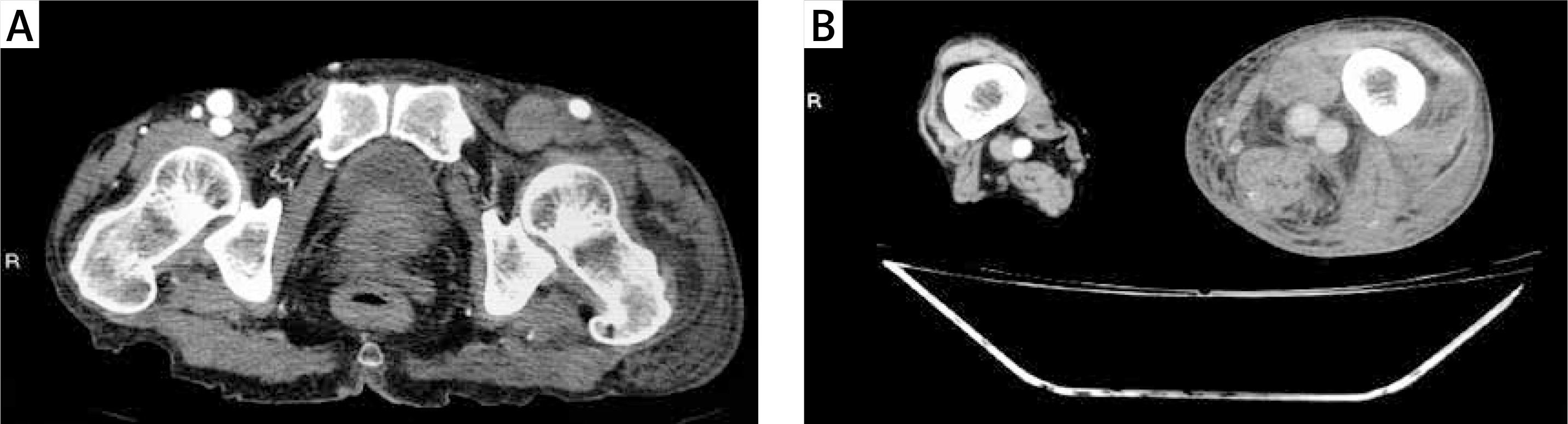
Figure 3
Left lower extremity complaints started to regress approximately 24 h after the interventional therapy

Venous stasis, hypercoagulability and endothelial damage contribute to the formation of thrombus [6]. Surgery, trauma, malignancy, prolonged immobility, congestive heart failure, pregnancy, obesity, advanced age and previous DVT are risk factors that predispose to a new thrombosis [6]. Although atrial fibrillation, heart valve diseases, prosthetic valve replacement, and common atherosclerotic disease are among the risk factors for systemic embolism [5], it was reported that short-term complications such as DVT in 1 patient and distal arterial thromboembolism in 10 patients in a study performed in patients with open repair of infrarenal aortic aneurysm [8]. Diagnosis of paradoxical embolism is based on showing arterial thromboembolism, DVT and right-to-left cardiac shunt in patients with persistent embolism attacks and no risk factors, and transthoracic echocardiography is recommended for systemic embolism cases [5]. Advanced age and major surgical history, such as open abdominal aortic aneurysm repair in our patient with no risk factors for embolism in ECG and echocardiography may increase the number of prolonged immobility periods, and may have a procoagulant effect and increase the risk of AAO and DVT.
Ramanan et al. reported that vascular surgery is an independent risk factor for the development of DVT, and the incidence of DVT after AAA surgery is between 1% and 24% [2]. The patients who have undergone aortic surgery can develop venous thromboembolism (VTE) at the rate of 2.5% to 2.9% during hospitalization or in the first 3 months after discharge, and it depends on the type of surgery and prophylaxis [2, 9–11]. Although there are few studies on the development of DVT after AAA surgery in the literature, de Maistre et al. reported that the rate of total DVT was 8.5% and proximal DVT rate was 1.5% after AAA surgery [10]. Our patient had a history of prolonged hospitalization and immobilization after AAA surgery, which could lead to DVT, and it was learned that he did not use anticoagulants regularly after discharge. We recommended combined treatment of LMWH and ASA for 2 weeks after the arterial thromboembolectomy and iliofemoral vein PMT + CDT treatments, followed by anticoagulant therapy.
Smoking causes an increase in plasma catecholamine release, sympathetic nerve stimulation, arterial stiffness, chronic low-grade inflammation, endothelial dysfunction, blood pressure changes and hypertension, and these mechanisms that accelerate atherosclerosis lead to plaque rupture and acute arterial occlusion [12]. Lower extremity acute ischemia secondary to distal arterial embolization, which is reported to develop rarely after abdominal aortic surgery, is a serious complication that can cause reoperation and even amputations [13, 14]. Thromboembolectomy is an effective treatment option in the proximal segment thromboembolism of the lower extremity, and it is known that CDT is more effective and safe than systemic thrombolysis especially in distal thromboembolism [13–15]. Although there are many case reports and studies in the literature regarding arterial and venous thrombosis, the coexistence of them in the same extremity is a rare clinical finding. Similar to this case report, Herity et al. reported a 61-year-old man with arterial and venous thrombus in the left lower extremity in 1997 [5]. Acute arterial thromboembolism can be treated by surgical thromboembolectomy or CDT thrombolytic therapy, whereas in acute proximal DVT, CDT thrombolysis and/or PMT modalities are effective treatment methods that reduce morbidity [13, 16]. In our current smoker patient who was learned to have been operated for AAA, we successfully performed surgical thromboembolectomy for the treatment of left popliteal-tibioperoneal artery thromboembolism and PMT + CDT for the treatment of acute left iliofemoral venous thrombosis. At first we performed thromboembolectomy under local anaesthesia for the treatment of acute popliteal-tibioperoneal arterial thromboembolism, and started LMWH treatment. Despite this, in the follow-up of our patient in the ICU, it was observed that the temperature was normalized in the left lower extremity, oedema and cyanotic colour changes did not improve, and PMT + CDT therapy was performed to treat acute left iliofemoral vein thrombosis. Approximately 24 h after the last procedure, decrease in skin tension, change of purplish colorization and warm up of limb were observed in the patient. The patient’s dorsalis pedis pulse was detected with palpation and hand-held Doppler USG and the patient was given medical treatment in the hospital for 2 days.
Phlegmasia cerulea dolens (PCD), a serious complication of iliofemoral venous thrombosis, should be considered in the differential diagnosis of acute arterial thromboembolism. In severe PCD patients, even amputation may be required due to suppression of arterial blood flow secondary to venous occlusion and ischemia [17, 18].
We think that in our elderly patient, arterial thromboembolism may have developed due to possible low flow due to clamping during a recent abdominal aortic surgery and possible atherosclerotic background and deep vein thrombosis developed secondary to immobilization. As a conclusion, it is important to recognize and differentiate acute arterial and deep venous thrombosis at the first admission to the ED in terms of optimal treatment and patient management, but physicians should remember that these clinical conditions can be seen together especially in patients with risk factors. It should be kept in mind that surgical and/or interventional treatments may be effective in order to obtain rapid results in patients in the presence of these two diseases.