Accordion phenomenon is a guide-wire-induced pseudolesion observed during the course of percutaneous coronary intervention (PCI) in tortuous vessels. This condition is usually seen as a consequence of the straightening effect and shortening of the tortuous artery precipitated by a stiff guidewire during coronary interventions [1]. Sometimes it leads to unnecessary intervention by inexperienced operators. Rarely this phenomenon can cause ischaemia and haemodynamic compromise due to the diminished or total loss of flow if not managed promptly [2]. Here we present a patient with non-ST segment elevation myocardial infarction (NSTEMI), who developed multiple pseudolesions in the tortuous left anterior descending coronary artery (LAD) during PCI.
A 59-year-old female with a history of hypertension and smoking presented to emergency department with chest pain. The patient was transferred to a coronary care unit after being diagnosed as NSTEMI. Early invasive strategy was planned because the patient had high-risk criteria. Coronary angiography via a right radial approach showed severe tortuosity in the LAD and right coronary artery, and severe stenotic lesion in the distal part of the LAD (Figures 1 and 2). Coronary angioplasty of the LAD was decided upon. The left main coronary ostium was engaged by a 6-F 4 Judkins (Cordis, Johnson& Johnson, Miami, FL, USA) guiding catheter. A 0.014-inch hi-torque balance middleweight (Abbott Vascular, Santa Clara, CA, USA) floppy guidewire was advanced across the stenosis. Control angiography showed straightened vessel with multiple filling defects and lesions in the mid segment of the LAD and total loss of the distal flow (Figure 3) while the patient had severe chest pain. Intracoronary nitrate was administrated in order to clarify the possibility of coronary spasm, but the angiographic appearance of the LAD did not change. Then we predilated the lesion using a 1.5 × 15 mm balloon (Invader, Alvimedica, Turkey), and a 2.75 × 18 mm drug-eluting stent (Xience, Abbott Vascular, Santa Clara, CA, USA) was deployed after predilatation (Figures 4 and 5). After successful stent deployment the guidewire was removed, and angiography showed complete resolution of the pseudolesions and recovered distal flow (Figure 6).
Figure 1
The coronary angiography showed severe tortuosity in the LAD and critical stenosis in the distal part

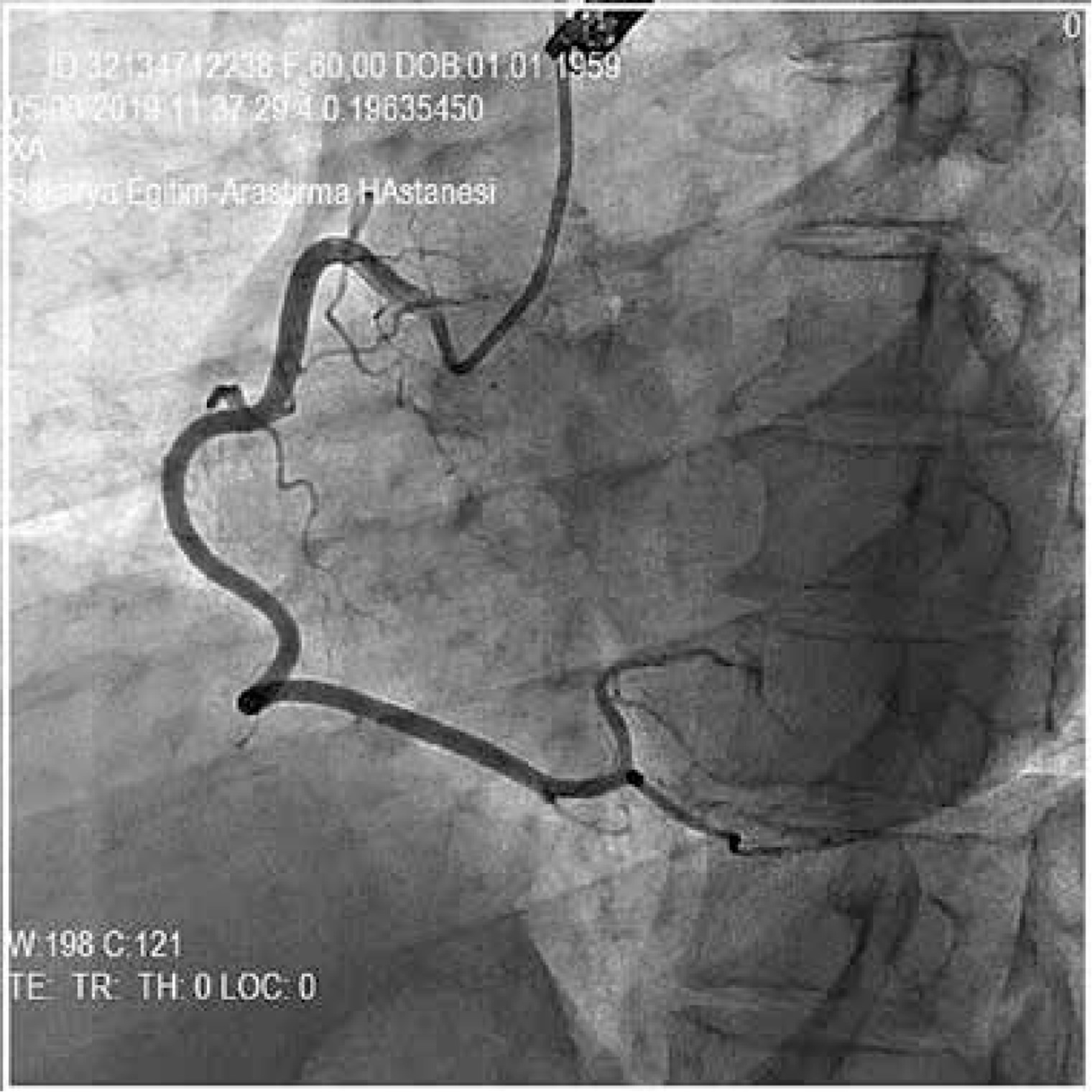
Figure 3
After advancing the guidewire, the control angiography showed straightened vessel with multiple filling defects and lesions in the mid segment of the LAD and total loss of the distal flow


Figure 6
After successful stent deployment the guidewire was removed, and angiography showed complete resolution of the pseudolesions and recovered distal flow

Accordion phenomenon during coronary intervention is a rare condition. This condition can be inappropriately identified as coronary spasm or dissection, which may falsely lead to unnecessary stenting [3]. It is more predictable in tortuous coronary arteries, and it can cause reversible narrowing and transient transmural myocardial ischaemia and rarely total loss of the distal flow in the presence of stenotic lesions [2, 4]. It is important to identify such iatrogenic pseudocomplications because they are generally benign and can be managed uneventfully by pulling back the guidewire and re-establishing of the coronary geometry.