
In patients undergoing percutaneous coronary intervention (PCI), there is a high risk of thrombotic complications such as stent thrombosis and myocardial infarction [1]. The use of dual antiplatelet therapy (DAPT) can reduce the incidence of such complications. However, the ideal length of DAPT following PCI is still debatable. Extension of the duration of DAPT can lower the residual ischemic risk at the expense of increased bleeding events [2, 3]. This can lead to early discontinuation of DAPT, which has been linked to increased rates of mortality and morbidity [3].
The available guidelines recommend the utilization of DAPT for a minimum duration of 12 months in individuals diagnosed with acute coronary syndrome (ACS), unless they are deemed to be at a high risk of bleeding [4, 5]. However, some trials have shown that the use of P2Y12 inhibitor monotherapy after short-term DAPT can significantly reduce the risk of hemorrhagic complications without increasing the risk of thrombotic events [6–8]. We conducted a systematic review and meta-analysis in light of recently published evidence to analyze the effectiveness of P2Y12 inhibitor monotherapy after short-term DAPT (1 to 3 months) compared to long-term (12 months) use of DAPT.
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting this study. The review protocol is registered with PROSPERO: CRD42024550288. Database searches were conducted from inception until April 2024 using PubMed/MEDLINE, EMBASE, Cochrane Library, and Google Scholar. Two independent investigators performed the literature search and selected the final list of included articles. The studies were included if they: (i) were randomized controlled trials (RCTs); (ii) reported data for patients who underwent PCI; (iii) compared the effects of extended use of P2Y12 inhibitor monotherapy after short-term DAPT (1–3 months) with long-term DAPT (12 months). Studies were excluded if they were only available as conference abstracts, observational studies, reviews or the comparative interventions were different. Baseline characteristics and primary outcome of Bleeding Academic Research Consortium (BARC) type 3 or 5 bleeding were extracted. The efficacy outcome was major adverse cardiovascular events (MACE) defined as the composite of all-cause mortality/CVD death, myocardial infarction, or stroke, while the secondary outcomes were all-cause mortality, myocardial infarction, ischemic stroke, and probable/definite stent thrombosis. The risk of bias assessment for the included RCTs was performed using version 2 of the Cochrane risk-of-bias tool. RevMan 5.4.1 (Cochrane Denmark, Copenhagen, Denmark) was used for performing data management and statistical analysis. Heterogeneity was assessed with the I2 statistic. The analysis estimated odd ratios (ORs) corresponding to 95% confidence intervals (CIs) for primary and secondary endpoints. We considered a p-value of less than 0.05 statistically significant for all clinical outcomes.
A total of 6 RCTs [6–11] were included in this meta-analysis. The trials reported data for 35,545 patients undergoing PCI who received antiplatelet therapy. 17,757 patients received extended P2Y12 inhibitor monotherapy after short-term DAPT while 17,788 patients received long-term DAPT. We found some concerns related to allocation concealment in 4 of the included RCTs. The baseline characteristics of each included study are summarized in Table I.
Table I
Baseline characteristics of the included studies and participants
| Trial | Year | Sample size (N) P2Y12 inhibitor/DAPT | Stent type | Duration of initial DAPT | Dose of P2Y12 inhibitor | Dose of DAPT | Follow-up | Age, mean ± SD | Males, N (%) | ACS, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| GLOBAL LEADERS | 2018 | 7980/7988 | Biolimus A9-eluting stent | 1 month | 90 mg ticagrelor twice | 75–100 mg aspirin + 75 mg clopidogrel/90 mg ticagrelor twice | 24 months | P2Y12 inhibitor = 64.5 ±10.3 DAPT = 64.6 ±10.3 | P2Y12 inhibitor = 6115/7980 (76.6) DAPT = 6139/7988 (76.9) | P2Y12 inhibitor = 3750/7980 (47.0) DAPT = 3737/7988 (46.8) |
| TWILIGHT | 2019 | 3555/3564 | 2nd generation drug eluting stent | 3 months | 90 mg ticagrelor twice | 81–100 mg aspirin + 90 mg ticagrelor twice | 12 months | P2Y12 inhibitor = 65.2 ±10.3 DAPT = 65.1 ±10.4 | P2Y12 inhibitor = females: 846 (23.8) DAPT = 852 (23.9) | P2Y12 inhibitor = 64% DAPT = 65.70% |
| STOPDAPT-2 | 2019 | 1500/1509 | CoCr-EES | 1 month | 75 mg clopidogrel | 81–200 mg aspirin + 75 mg clopidogrel | 12 months | P2Y12 inhibitor = 68.1 ±10.9 DAPT = 69.1 ±10.4 | P2Y12 inhibitor = 1183 (78.9) DAPT = 1154 (76.5) | P2Y12 inhibitor = 565 (37.7) DAPT = 583 (38.6) |
| SMART-CHOICE | 2019 | 1495/1498 | CoCr-EES PtCr-EES SES | 3 months | 75 mg clopidogrel/10 mg prasugrel/90 mg ticagrelor twice | 100 mg aspirin + 75 mg clopidogrel/10 mg prasugrel/90 mg ticagrelor twice | 12 months | P2Y12 inhibitor = 64.6 ±10.7 DAPT = 64.4 ±10.7 | P2Y12 inhibitor = 1087 (72.7) DAPT = 1111 (74.2) | P2Y12 inhibitor = 58.20% DAPT = 58.10% |
| TICO | 2020 | 1527/1529 | Ultrathin BP-SES | 3 months | 90 mg ticagrelor twice | 100 mg aspirin + 90 mg ticagrelor twice | 12 months | P2Y12 inhibitor = 61 ±11 DAPT = 61 ±11 | P2Y12 inhibitor = 1204 (79) DAPT = 1224 (80) | P2Y12 inhibitor = 100% DAPT = 100% |
| ULTIMATE-DAPT | 2024 | 1700/1700 | 2nd generation drug-eluting stent | 1 month | 90 mg ticagrelor twice daily plus a matching enteric-coated oral placebo | 90 mg ticagrelor twice daily plus 100 mg enteric-coated aspirin once daily | 12 months | P2Y12 inhibitor = 62 (54–70)* DAPT = 63 (54–69)* | P2Y12 inhibitor = 1264 (74.4) DAPT = 1257 (73.9) | P2Y12 inhibitor = 100% DAPT = 100% |
DAPT – dual antiplatelet therapy, CoCr-EES – cobalt-chromium everolimus-eluting stent, CoCr-EES PtCr-EES SES – drug-eluting stents made from cobalt-chromium (CoCr) or platinum-chromium (PtCr) alloy – and eluting different drugs such as everolimus (EES) or sirolimus (SES), ultrathin BP-SES – ultrathin biodegradable polymer sirolimus-eluting stent, ACS – acute coronary syndrome, N – number.
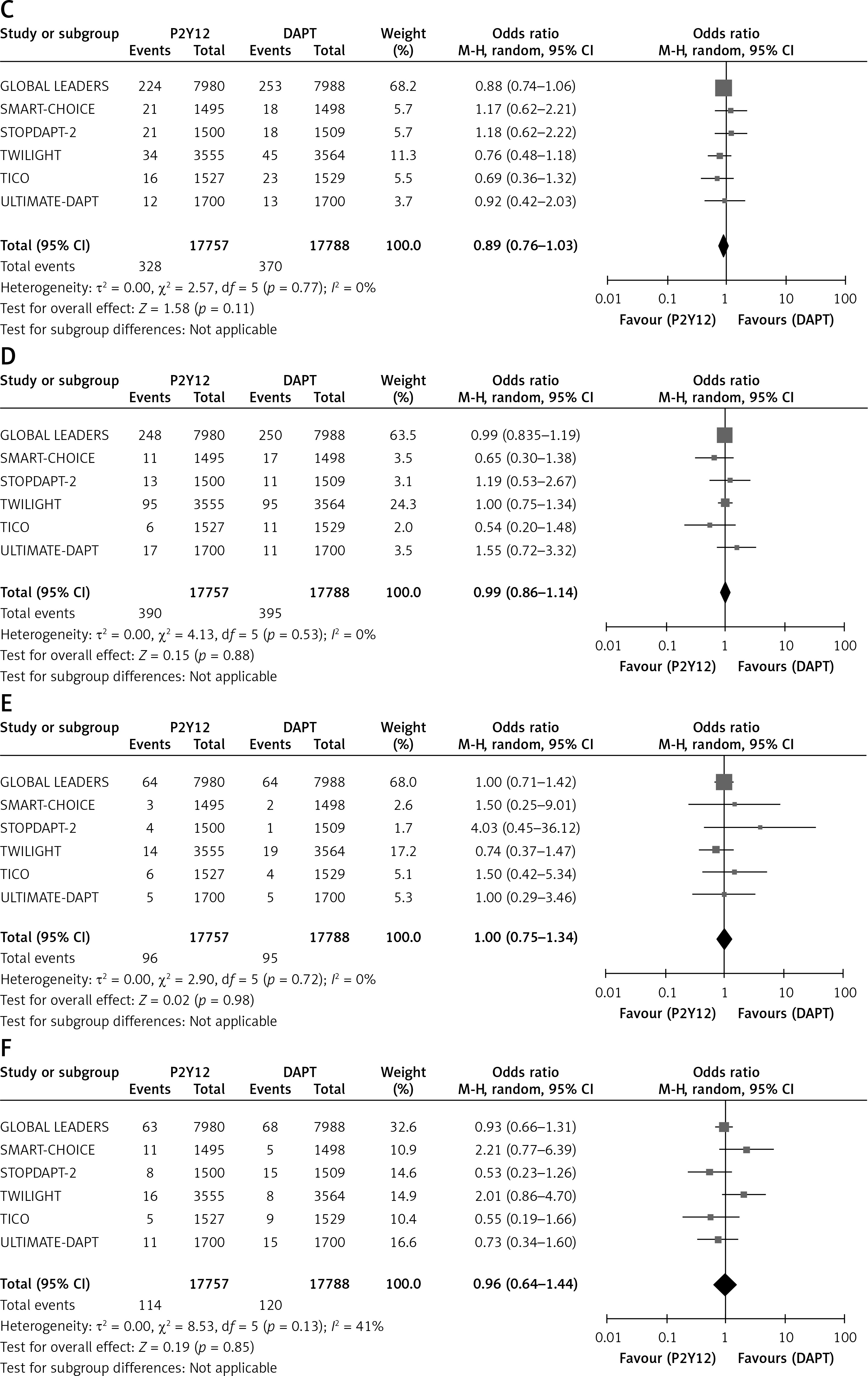
Our meta-analysis showed a significantly reduced incidence of BARC type 3 or 5 bleeding in patients who received P2Y12 inhibitor monotherapy compared with DAPT (OR = 0.59, 95% CI: 0.41–0.85, p = 0.005. Figure 1 A). The heterogeneity was moderate (I2 = 74%). The incidence of MACE in patients who received P2Y12 inhibitor monotherapy was 3.7% compared to 4.1% MACE in the patients who received DAPT for 12 months. P2Y12 inhibitor monotherapy was associated with a significantly decreased incidence of MACE (OR = 0.89, 95% CI: 0.80–1.00, p = 0.04, Figure 1 B). The incidence of secondary endpoints, which included all-cause mortality (OR = 0.89, 95% CI: 0.76–1.03, p = 0.11, Figure 1 C), myocardial infarction (OR = 0.99, 95% CI: 0.86–1.14, p = 0.88, Figure 1 D), stent thrombosis (OR = 1.00; 95% CI: 0.75–1.34, p = 0.98, Figure 1 E) and ischemic stroke (OR = 0.96, 95% CI: 0.64–1.44, p = 0.85, Figure 1 F), remained comparable between the two groups.
Figure 1
Forest plot showing pooled effect sizes for BARC type 3 or 5 bleeding (A), MACE (B), All-cause mortality (C), myocardial infarction (D), stent thrombosis (E), ischemic stroke (F)
BARC – Bleeding Academic Research Consortium, MACE – major adverse cardiovascular events.

Our meta-analysis of 35,545 patients showed that extended use of P2Y12 inhibitor monotherapy after short-term DAPT can significantly reduce the incidence of BARC type 3 or 5 bleeding and MACE compared with long-term DAPT. Moreover, the incidence of all-cause mortality, myocardial infarction, ischemic stroke, and probable/definite stent thrombosis remained comparable across the two groups.
This is the largest meta-analysis on this subject, as we pooled results of the ULTIMATE-DAPT trial not analyzed by the previous investigators. Aspirin monotherapy is recommended by the current guidelines in the case of discontinuation of DAPT [12, 13]. However, long-term aspirin monotherapy can offset the clinical benefit by increasing the risk of thrombotic complications. P2Y12 inhibitors result in a better and faster antiplatelet effect compared to aspirin. These drugs can be used for an extended period after a short course of DAPT and result in a reduced risk of major bleeding without increasing the risk of thrombotic events in patients. Hence, the use of intravascular imaging during PCI [14, 15] followed by an optimal course of antiplatelet therapy can lead to better clinical outcomes.
This study has some limitations. Firstly, we could not perform subgroup analyses stratified by sex, age, and other effect modifiers due to the small number of included studies. As most of the trials included in the study were open-label, bias may be present due to the absence of blinding. Additionally, the diagnostic criteria for the endpoints were different across the pooled studies, which could have caused effect modification. Tests for funnel plot asymmetry could not be used for evaluating publication, as only 6 trials were included in the study.
In conclusion, this study provides evidence of the extended use of P2Y12 inhibitor monotherapy after short-term DAPT for lowering the risk of bleeding and its subsequent adverse events. Further randomized controlled trials are required to evaluate the potency of different types of P2Y12 inhibitors along with their net clinical benefit in patients undergoing PCI.